Intended for healthcare professionals
Rapid response to:
Analysis
Why cancer screening has never been shown to “save lives”—and what we can do about it
BMJ 2016; 352 doi: https://doi.org/10.1136/bmj.h6080 (Published 06 January 2016) Cite this as: BMJ 2016;352:h6080
Including all mortality
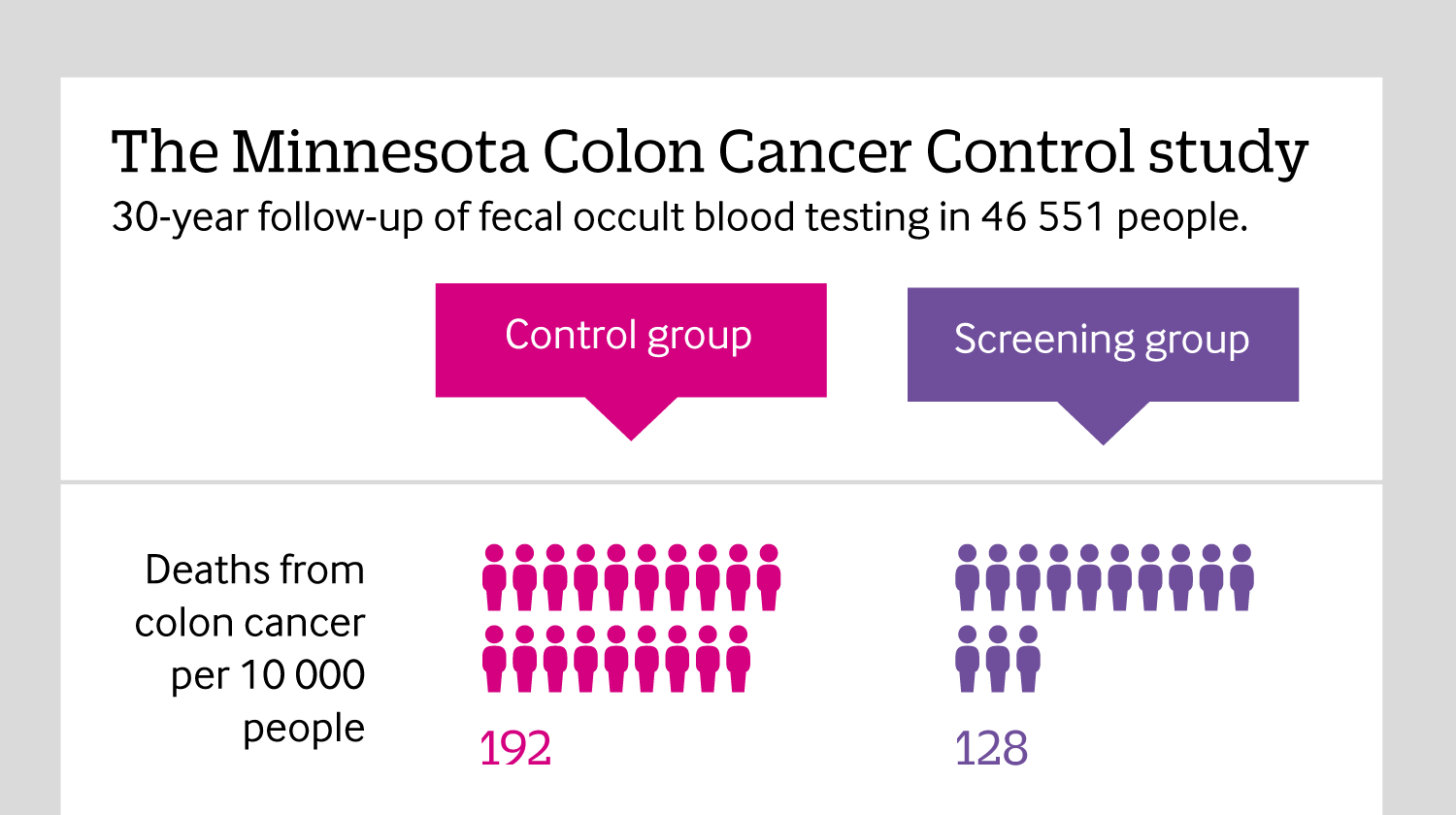
Click here to see an infographic, explaining why reporting all causes of mortality in cancer screening trials is so important.
Rapid Response:
Re: Why cancer screening has never been shown to “save lives”—and what we can do about it
Cervical screening does reduce mortality.
These authors are right to point out that most cancer screening has not been shown to save lives, because single trials to prove reduction in total mortality from screening for any one cancer at a time would be too large to be practicable. So decisions have to be made on the best available evidence. Part of the problem is that evidence that was good enough in the past is now regarded by purists as methodologically inadequate. But that does not mean that we should discard it. Simply because a proposition has not been demonstrated with a randomised trial does not mean it is wrong. RCTs are necessary when the evidence is equivocal, not when it is overwhelming. No trials were performed to show that smoking caused lung cancer and other diseases, and no one would seriously suggest one. In the field of cancer, cervical screening is the best example.
This cancer that used to kill over 1% of women is now rare in countries that screen consistently. Because this cancer affects young to middle-aged women, for whom there are few other competing causes of death, and the size of the incidence and mortality reduction is so great, its value was demonstrated in the 1970s to 1980s with a series of ecological studies, comparing regions or countries that introduced screening at different time periods, and case control studies1. The consistency of these different types of studies and the current differences between countries that screen and those that do not is so great that it is difficult to ascribe any other cause but screening2,3.
Biologically, cervical screening works because it detects and permits treatment of pre-cancers and very early invasive cancers – admittedly at the price of substantial overdiagnosis and overtreatment, which should be minimised in an effective program. The authors are right to point out that screening is less effective for the other cancers they discuss: in part because they detect disease at a later stage and at later ages. Cervical screening is an exception to their general rule.
1. Miller AB, Lindsay J, Hill GB. Mortality from cancer of the uterus in Canada and its relationship to screening for cancer of the cervix. Int J Cancer 1976: 17, 602-612.
2. IARC Working Group on the Evaluation of Cancer-Preventive Strategies. Cervix cancer screening. IARC 2004: Lyon, France
(IARC Handbooks of Cancer Prevention; 10)
3. Arbyn M, Raifu AO, Autier P, Ferlay J. Burden of Cervical Cancer in Europe: estimates for 2004. Annals of Oncology 2007: 18, 1708-1715,
Competing interests: I was the lead author for the Canadian Task Force on Preventive Health Care recommendations on Cervical Screening.