Why cancer screening has never been shown to “save lives”—and what we can do about it
BMJ 2016; 352 doi: https://doi.org/10.1136/bmj.h6080 (Published 06 January 2016) Cite this as: BMJ 2016;352:h6080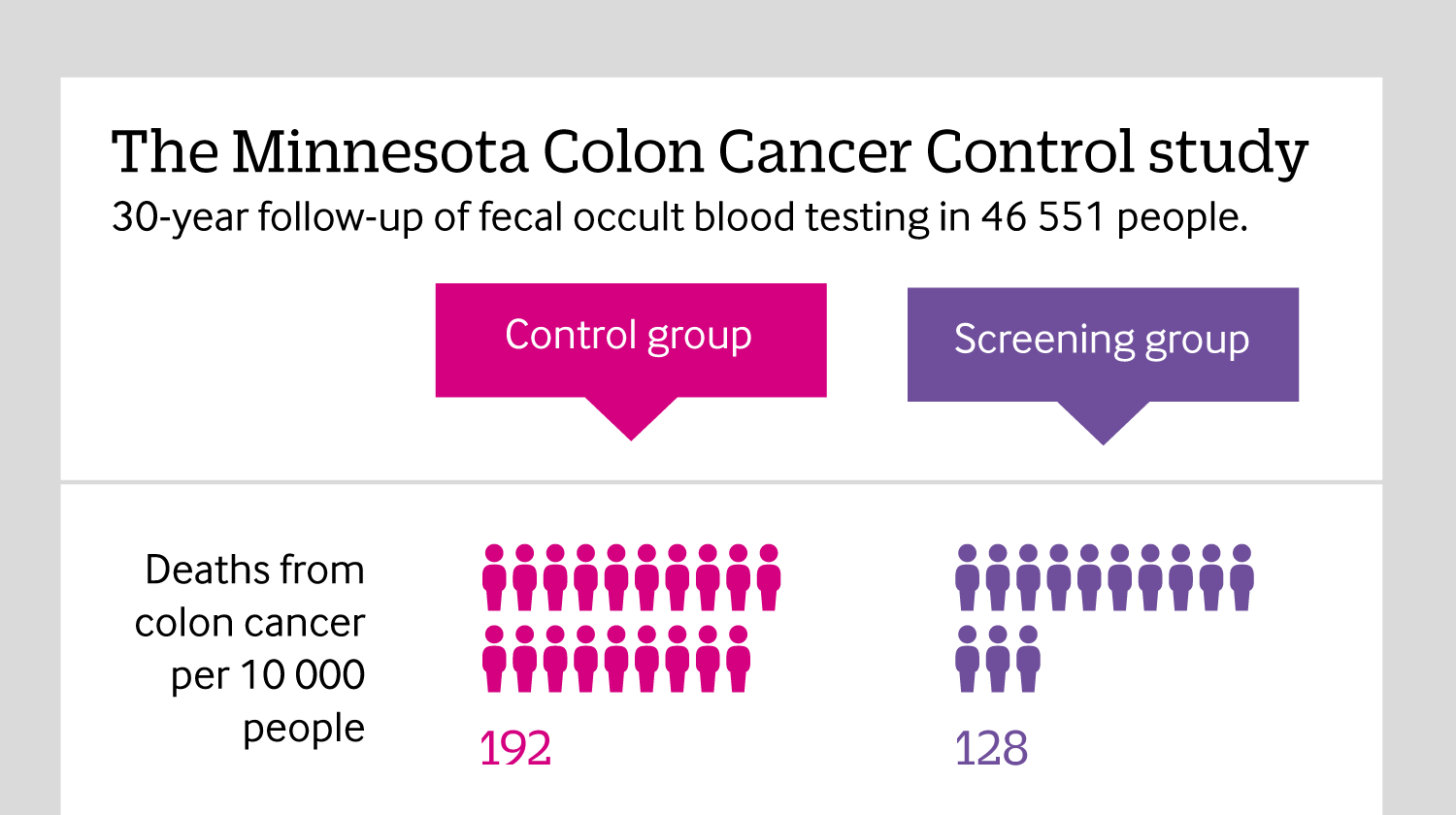
Including all mortality
Click here to see an infographic, explaining why reporting all causes of mortality in cancer screening trials is so important.

All rapid responses
Rapid responses are electronic comments to the editor. They enable our users to debate issues raised in articles published on bmj.com. A rapid response is first posted online. If you need the URL (web address) of an individual response, simply click on the response headline and copy the URL from the browser window. A proportion of responses will, after editing, be published online and in the print journal as letters, which are indexed in PubMed. Rapid responses are not indexed in PubMed and they are not journal articles. The BMJ reserves the right to remove responses which are being wilfully misrepresented as published articles or when it is brought to our attention that a response spreads misinformation.
From March 2022, the word limit for rapid responses will be 600 words not including references and author details. We will no longer post responses that exceed this limit.
The word limit for letters selected from posted responses remains 300 words.
In their analysis of cancer screening, Prasad et al. focus solely on mortality figures. In screening research counting mortality is quickest, easiest and least expensive to do. It is also insufficient.
The authors only mention morbidity resulting from false positive screening results, not the reduced morbidity in cancers detected and treated early. This is misleading.
Patients value quality of life at least as much as mere survival. Perhaps that is where screening proves its value more than in saving lives. For instance, screening detects many breast cancers at a stage where tumours can be treated with breast conserving surgery, radiotherapy and hormone treatment. Without screening, diagnosis is delayed until the cancer becomes symptomatic. At that stage, mastectomy, axillary lymph node clearance and chemotherapy may be necessary. This adds a burden of major surgery (more so with reconstruction), longer hospital stay, longer time off work, toxicity of chemotherapy, and increased risks of complications, neutropenic sepsis, and long term sequelae such as lymphedema and cognitive loss (‘chemo brain’) [1].
Similarly, even when it does not save lives, cervical cancer screening saves women’s fertility and avoids more radical surgery and pelvic radiotherapy for those women who would otherwise have developed larger invasive cancers. These treatments have great impact on quality of life.
Focusing solely on mortality figures is shortsighted. It is imperative that future research evaluates burden of treatment, morbidity and quality of life as well as mortality statistics. Only then can people be given adequate information to make an informed decision on whether to take up screening or not.
[1] Kesler SR, Blayney DW. Neurotoxic Effects of Anthracycline- vs Nonanthracycline-Based Chemotherapy on Cognition in Breast Cancer Survivors. JAMA oncology. 2015: 1-8.
Competing interests: No competing interests
Prasad et al’s article exposes a well recognized fallacy in preventive medicine – use of all-cause mortality when studying an intervention to prevent deaths from a specific cause. The problem is that total mortality is too insensitive a measure to determine efficacy and also to identify unsuspected hazards. Preventing all cases of polio has an imperceptible effect on total mortality yet it would be absurd to regard the value of polio vaccination as unproven. The fallacy is one that we and our colleagues regularly teach on. It is surprising to see it appearing in the BMJ.
A trial with 100,000 people, 50,000 randomized to each of an intervention and a control arm might yield the following results: 400 deaths from cancer X, and 7400 deaths overall in controls, 200 from cancer X and 7200 overall in the screening arm - a highly significant 50% reduction in mortality from cancer X but the difference in overall mortality is not statistically significant. There is clear evidence of efficacy. The assessment of possible adverse effects should be determined by examining causes of death other than cancer X, and if any are significantly increased whether this is consistent in other trials to exclude a chance difference that was not specified a priori. In relation to cancer X it would be unnecessary and therefore unethical to continue randomizing patients into a trial until a significant difference was observed in all-cause mortality.
It would be a serious mistake to adopt what Prasad et al propose.
Competing interests: No competing interests
Dear BMJ Editor
Re Why cancer screening has never been shown to “save lives”—and what we can do about it BMJ 2016; 352 doi: http://dx.doi.org/10.1136/bmj.h6080 (Published 06 January 2016) : BMJ 2016;352:h6080
Attached are graphs showing trends Standardized Death Rates (SDRs) from breast cancer in the UK and selected countries for all ages and 0-65, as well as female life expectancy at birth. Also shown are SDRs for cancer of cervix and lung rate (total population). Theses graphs are derived from WHO Europe Health for All Data Base, December 2015.
The dramatic improvements in declining mortality from breast cancer in the UK and elsewhere may in part be due to improved treatment, but are more likely mainly due to earlier case finding from mammography programs. The reduction in cancer of cervix mortality is also impressive and likely due to the improved screening in the UK and Western European countries. Poor implementation of Pap smear screening in countries of Eastern Europe leave Cancer of Cervix mortality rates high.
The value of screening for women's health issues should take these trends into account when addressing the issues discussed in the Pradas article and accompanying editorial.
Ted Tulchinsky MD MPH
Emeritus, Braun School of Public Health, Hebrew University-Hadassah, Ein Karem, Jerusalem, Israel 91220
Head of School of Health Sciences, Ashkelon College, Ashkelon, Israel
Deputy Editor Public Health Reviews
Email: tulchinskyted@hotmail.com
Competing interests: No competing interests
The overall mortality studies wouldn't bring too many benefits if not properly designed. I am sure that, if we would compare mortality over 100 year of a population of Indios living somewhere in Amazonas without any medical care, and a population of high-class citizens living in West Europe, that we would get a difference of 0%. I am even sure that overall mortality of all people on the Earth is definitely the same, independent of the screening or therapy used. Eventually, they will all die. So the proper measurement would not be the overall mortality detection but rather the mean life duration of the compared populations (as mentioned in one of the cited studies in the article).
Competing interests: No competing interests
The authors argued that cancer screening is not useful to reduce overall mortality, although it reduces disease specific mortality, and gave reasons why it does not decrease overall mortality. The way of analyzing the facts targeted in trials are with the purpose of screening specifically is to bring down morbidity and mortality due to a specific disease and not to reduce the overall mortality. For example, cervical cancer screening is to catch up the pre-neoplastic lesions rather than neoplastic lesions for decrease in that cancer related morbidity and mortality which can also be called clinical down staging of that disease in the community. Moreover, it appears rather impractical to weigh it against overall mortality as the proportion of cancer cases is also meager in comparison to deaths due to all causes. The main aim of screening is to detect the cancer lesion early before it grows to an advanced stage for effective treatment. In advanced disease, treatment becomes difficult. In view of the burden to health resources the cost of treatment to advanced stage disease or full blown cancer is much higher as compared to pre-cancer and early cancer. Another advantage is screening tests are supposed to be cheaper and cost effective when applied on a mass scale on specific population to reduce burden of specific disease in a community and along with a proportion of burden of overall disease on health care infrastructure.
Screening for preventable indolent lesions has a potential benefit from available low cost screening tests. These low cost tests can be useful even in a low resource setting. These tests are useful only in case of cancers which have a long pre-invasive stage with a long latent phase as compared to tests for highly malignant tumors with a non-significant pre-invasive stage. However, the harms of over-diagnosis should not be ignored for any screening, for example, in breast and prostate cancer. A proper counselling and adequate referral facility are needed before planning a screening programme.
The authors emphasized the need for large screening trials for reducing mortality infect trials for reducing disease specific mortality can be more beneficial if focused for high risk group, say, for example, oral screening in smokers and tobacco users. Conducting big trials with the objective to record overall reduction in mortality due to a specific disease first and of all cause mortality will cause a huge burden on resources. Quality control of such a big trial can also be a major issue. In conclusion, decrease in mortality due to screening is not a good statistical indicator of reduction in overall mortality but an excellent indicator for disease specific mortality. We agree with the recommendations of authors as use of cancer registries and civil registrations for monitoring overall mortality changes.
Dr Smita Asthana, Scientist D
Dr Satyanarayana Labani, Scientist G
Institute of Cytology &Preventive Oncology (ICMR)
Sec 39 Noida, India
Competing interests: No competing interests
We thank Prof. Dickinson and others for their comments on cervical cancer screening. In fact, we do take a slightly softer approach to cytological based cervical cancer screening for the reasons they outline--and the authors of this commentary all have slightly different opinions. In a draft of our commentary, we suggested undertaking trials of cervical cancer screening study in order to determine the appropriate interval of follow up – not whether it should be performed. By this method, we may test longer and longer intervals, if trials show equal results. Nevertheless, it must be recognized that ecological data merely suggest that such screening is effective, and is not proof of it. Interpreting such data in the setting of large changes in behavior, diet, lifestyle and exposure is a very uncertain science, and may easily confirm one's preconceived biases. Finally, cytologically based screening is considered impractical and unaffordable in many parts of the world; thus, alternatives are needed, and these can be rigorously tested.
Regarding Dr. Dickinson argument: 'You don't need a randomized trial to show smoking is harmful.' We see this argument often and wish to clarify one point. Randomized trials are conducted to test interventions of putative benefit. They are not done to evaluate for putative harms. In the case of smoking, the increased risk of lung cancer is large and consistent, so it is reasonably to pursue policies to curb smoking among healthy people. At the same time, in other settings, it may be reasonable to pursue randomized trials-- not of smoking-- but, of the converse, strategies to reduce smoking. For instance, some researchers argue that patients with metastatic lung cancer (a poor prognosis) should be urged to quit. Others find this recommendation implausible-- unlikely to extend life, and likely to reduce quality. In this situation, a randomized trial of smoking cessation seems reasonable.
But Dr. Dickinson’s broader point is that one doesn’t need a randomized trial to determine benefit from interventions that are overwhelmingly positive. We agree that this may be true in some instances; for example, no randomized controlled trial has been conducted to prove that penicillin improves outcomes for pneumococcal pneumonia. However, we have all been fooled by presumptions of overwhelming benefit for many years, such as with Class 1c anti-arrhythmic drugs that successfully abolished or reduced serious arrhythmias, but are estimated to have killed tens of thousands of individuals over the many years they were in use. The rate of cervical cancer (and not just deaths) in other nations versus the United States is dramatically different [1]. While it’s possible that screening, by intervening on early cellular changes might account for this, it is also possible that the difference in rates may be partially or wholly due to other differences. We believe that even some seemingly obviously beneficial interventions may need closer scrutiny.
[1] http://www.wcrf.org/int/cancer-facts-figures/data-specific-cancers/cervi...
Competing interests: No competing interests
In their enthusiasm, screening advocates established programmes in advance of evidence of benefit, and have omitted to mention, even investigate, what screening means for potential participants, including the price they pay for a chance of benefit. For a host of sensible reasons people may decline without danger, but persuasive recruitment methods have engendered public fear.
Wording of public information is a critical matter. Claims must be warranted by evidence. The claim that screening for X saves lives means that some people screened for X live longer than they would have without screening. Fewer deaths from X does not entail that, and does not warrant the claim that screening for X saves lives.
In the case of breast screening, nobody ever even tried to show that it saves lives: the trials aimed only to find out if breast cancer mortality was reduced. None of them reliably showed even that.
Attempting to mend past errors, screening professionals now talk of the benefits – plural – and harms of breast screening. Only one benefit is aimed for, that of longer life. That is unproven, and there are no others.
Screening professionals often claim that screening does more good than harm. People need to know that this value judgment applies to a population: to screeners the harm sustained by the many is less than the good of somewhat fewer deaths from the target disease without knowing who benefits. That screening for X benefits some anonymous members of a population in terms of what is important to screeners does not entail that screening for X benefits each member of the population in terms of what is important to them. To the participant, neither exchanging one cause of death for another, nor the very low probability for them of even that, is important.
Potential participants also need to know what happens to the rest of the screened population, with the range of estimated numbers, not cherry-picked figures, and on what kind of evidence these are based. Thus they see each outcome that may affect them, not just the outcome that interests screeners, how likely it is, and how certain, or otherwise, the estimates are.
In a recent radio broadcast Ann Mackie of Public Health England, now responsible for breast screening, defended the programme claiming that it saves lives and that it does more good than harm, and praised the revised information because 25 improperly informed potential participants were asked what it should say.(1) The resulting leaflet makes unwarranted claims of benefit and remains unclear and misleading about the nature and risks of harm.(2) People don’t know what the deal is.
More important than research, such as the LORIS trial which cannot make breast screening effective but only reduce the numbers harmed, is to stop harming people while telling them they are benefitting.
Professionals involved in breast screening could be paid to inform rather than screen people and paid extra for every informed woman who declines.
1) http://www.bbc.co.uk/programmes/p03cg3lb#play
2) https://www.gov.uk/government/uploads/system/uploads/attachment_data/fil...
Competing interests: Diagnosed through screening
The present article has brought out the controversy of the benefits of cancer screening programmes in reducing mortality. While the authors have brought out the fact that cancer screening does not save lives, the benefits of screening for certain cancers such as cervical cancer cannot be overruled. The concept of early detection by pap smear often helps in reducing the chances of mortality due to cervical cancer. Detection at a late stage does not, however, reduce the mortality. This is true even for breast cancer.
The problem with the presently available methods of early detection of cancers is that they are not very sensitive and specific and often lead to false positive results which may adversely affect the quality of life of the affected persons, including causing psychological problems. We need to develop skills to detect cancers at an early stage so that mortality can be reduced and lives saved. There is also a need to understand the natural history at the bio-molecular level so that we can better understand the stages of carcinogenesis and hence early detection could be done.
Competing interests: No competing interests
Cancer screening: who should choose?
To the editor,
Dear Sir
We agree with V. Prasad and colleagues’ conclusions (1).
The benefits of cancer screening programs are very uncertain. They are often presented as relative risk decreasing, giving a deceptive feeling that these benefits are highly significant. However, studies including several hundreds of thousand people followed for many years just could not demonstrate an overall mortality benefit. This obviously means that if such a benefit does exist, it can only be very small.
A few people certainly benefit from cancer screening. But many other suffer from it. Harms are linked to overdiagnosis and overtreatment. Many people have to cope with the idea that they suffer from a very severe illness, which is often unreal. Many have to endure aggressive treatments for a non-existent illness. And quite often, they are grateful to screening because they think it allowed them to “survive cancer”.
In a word, cancer screening is a game of chance, with very few winners, and a lot of losers. But if benefits are pointed out, harms are hidden.
For all these reasons, it is unethical to promote any cancer-screening program without giving to every people the best available information and time to think before asking to their personal consent (2). This information should be neutral, independent, fair, as exhaustive as possible and true, but also understandable for people that do not necessarily have a scientific background. This last requirement may come into conflict with the others. To be understandable, information may have to be less comprehensive, or less accurate. Last, but not least, information should not be too emotional. It should not play with the fears of severe suffering or death, or with guilt.
Several studies have shown that official information on cancer screening is not adequate, especially in France (2-5). All around the planet, breast-cancer screening is probably the most advertised, notably during the pink October campaigns. Pink October slogans are quite simplistic: earlier is better; more is better; to be in is good for you… This is why a multidisciplinary group of French health professionals and patients, independent of all organisation or administration, and without any conflict of interest, has voluntarily developed an information leaflet intended for women, in an attempt to give them back the power of a really informed decision. This fully referenced leaflet is freely downloadable, in French and in English, in colour or black and white (6). We hope that remarks from readers will help improve it year after year.
1- Prasad V, Lenzer J, Newman D. Why cancer screening has never been shown to “save lives”—and what we can do about it. BMJ 2016;352:h6080.
2- Hersch J and all. How do we achieve informed choice for women considering breast screening? Prev Med. 2011 Sep;53(3):144-6.
3- Slaytor EK, Ward JE . How risks of breast cancer and the benefits of screening are communicated to women: analysis of 58 pamphlets. BMJ 1998; 317: 263–4.
4- Domenighetti G and all. Women’s perception of the benefits of mammography screening: population-based survey in four countries. International Journal of Epidemiology 2003;32:816–821.
5- Braillon A, Nicot P. Cancer screening and informed consent. A new French exception? Prev Med. 2011 Dec;53(6):437; author reply 438.
6- Bour C and all. Screening breast cancer? A decision that belongs to every woman. Avalaible at: http://cancer-rose.fr/wp-content/uploads/2015/10/Cancer-Rose_16pUK2-2-co...
Competing interests: No competing interests
Re: Why cancer screening has never been shown to “save lives”—and what we can do about it
I am pleased that Prasad and colleagues take a “slightly softer line” on cervical screening. They are right that newer methods of screening in this field should be carefully assessed, in particular by trials of interval, to determine their relative benefits and harms.
However, they also set a very high standard for proof of causation. More important in practical terms: how high a level of certainty is needed before decisions can be made to mobilise large amounts of resources for screening in the health care system? Decisions in the United States largely appear to be made by physicians and lobby groups without necessarily using much science1. In countries with national health systems, decisions about programs are mostly made by hard-headed public servants, who require high levels of evidence. This has led to programs being established at different times and with different features. They provide quasi-experimental cohort data series. Matti Hakama and his team demonstrated that program introduction in the Nordic countries was followed by cause-specific mortality declines that matched the timing and intensity of the screening.2 This and further evidence has been summarised exhaustively, for example by the International Agency for Research on Cancer.3
Prasad and colleagues conclude that “some seemingly obviously beneficial interventions may need closer scrutiny.” Cervical screening has been subjected to such scrutiny, and has proven its value: not to reduce overall mortality, which cannot be demonstrated for a cancer that "only" affects 2% of women, but to reduce premature and awful deaths.
1. Mukherjee,S. The Emperor of All Maladies: a biography of cancer. 2010 Scribner, New York.
2. Laara E, Day NE, Hakama M. Trends in mortality form cervical cancer in the Nordic countries: associations with organised screening programmes. Lancet 1987, 1247-1249
3. Hakama M, Miller AB, Day NE, eds. Screening for Cancer of the Uterine Cervix. Lyon, IARC Scientific Publications,1986.
Competing interests: I was the lead author for the report on Cervical Screening of the Canadian Task Force on Preventive Health Care