Comparative safety of direct oral anticoagulants and warfarin in venous thromboembolism: multicentre, population based, observational study
BMJ 2017; 359 doi: https://doi.org/10.1136/bmj.j4323 (Published 17 October 2017) Cite this as: BMJ 2017;359:j4323
- Min Jun, senior lecturer1 2 3,
- Lisa M Lix, professor4,
- Madeleine Durand, assistant clinical professor5,
- Matt Dahl, data analyst6,
- J Michael Paterson, assistant professor7 8 9,
- Colin R Dormuth, associate professor10,
- Pierre Ernst, professor11 12,
- Shenzhen Yao, PhD student13,
- Christel Renoux, assistant professor11 14 15,
- Hala Tamim, associate professor16 17,
- Cynthia Wu, associate professor18,
- Salaheddin M Mahmud, associate professor19,
- Brenda R Hemmelgarn, professor1
- for the Canadian Network for Observational Drug Effect Studies (CNODES) Investigators
- 1Departments of Medicine and Community Health Sciences, University of Calgary, AB, Canada
- 2The George Institute for Global Health, Sydney, NSW, Australia
- 3Faculty of Medicine, UNSW Sydney, NSW, Australia
- 4Department of Community Health Sciences, University of Manitoba, MB, Canada
- 5Department of Internal Medicine, University of Montreal Health Centre, Montreal, QC, Canada
- 6Manitoba Centre for Health Policy, Department of Community Health Sciences, University of Manitoba, Winnipeg, MB, Canada
- 7Department of Family Medicine, McMaster University, Hamilton, ON, Canada
- 8Institute for Clinical Evaluative Sciences, Toronto, ON, Canada
- 9Institute of Health Policy, Management and Evaluation, University of Toronto, ON, Toronto
- 10Department of Anesthesiology, Pharmacology and Therapeutics, University of British Columbia, Vancouver, BC, Canada
- 11Center for Clinical Epidemiology, Lady Davis Research Institute, Jewish General Hospital, Montreal, QC, Canada
- 12Department of Medicine, McGill University, Montreal, QC, Canada
- 13College of Pharmacy and Nutrition, Department of Pharmacy, University of Saskatchewan, SK, Canada
- 14Department of Neurology and Neurosurgery, McGill University, Montréal, QC, Canada
- 15Department of Epidemiology and Biostatistics, McGill University, Montréal, QC, Canada
- 16School of Kinesiology and Health Science, York University, Toronto, ON, Canada
- 17Department of Community Health and Epidemiology, Dalhousie University, Halifax, NS, Canada
- 18Department of Medicine, University of Alberta, Edmonton, AB, Canada
- 19Department of Community Health Sciences, University of Manitoba, Winnipeg, MB, Canada
- Correspondence to: B Hemmelgarn Brenda.Hemmelgarn{at}ahs.ca
- Accepted 11 September 2017
Abstract
Objective To determine the safety of direct oral anticoagulant (DOAC) use compared with warfarin use for the treatment of venous thromboembolism.
Design Retrospective matched cohort study conducted between 1 January 2009 and 31 March 2016.
Setting Community based, using healthcare data from six jurisdictions in Canada and the United States.
Participants 59 525 adults (12 489 DOAC users; 47 036 warfarin users) with a new diagnosis of venous thromboembolism and a prescription for a DOAC or warfarin within 30 days of diagnosis.
Main outcome measures Outcomes included hospital admission or emergency department visit for major bleeding and all cause mortality within 90 days after starting treatment. Propensity score matching and shared frailty models were used to estimate adjusted hazard ratios of the outcomes comparing DOACs with warfarin. Analyses were conducted independently at each site, with meta-analytical methods used to estimate pooled hazard ratios across sites.
Results Of the 59 525 participants, 1967 (3.3%) had a major bleed and 1029 (1.7%) died over a mean follow-up of 85.2 days. The risk of major bleeding was similar for DOAC compared with warfarin use (pooled hazard ratio 0.92, 95% confidence interval 0.82 to 1.03), with the overall direction of the association favouring DOAC use. No difference was found in the risk of death (pooled hazard ratio 0.99, 0.84 to 1.16) for DOACs compared with warfarin use. There was no evidence of heterogeneity across centres, between patients with and without chronic kidney disease, across age groups, or between male and female patients.
Conclusions In this analysis of adults with incident venous thromboembolism, treatment with DOACs, compared with warfarin, was not associated with an increased risk of major bleeding or all cause mortality in the first 90 days of treatment.
Trial registration Clinical trials NCT02833987.
Introduction
Venous thromboembolism, a condition that includes deep venous thrombosis and pulmonary embolism, is common with an annual incidence of approximately one case per 1000 people.1 As the third most common cause of vascular related death after myocardial infarction and stroke, venous thromboembolism is associated with considerable morbidity and premature mortality.2
Warfarin has been the primary oral anticoagulant used for treatment of venous thromboembolism but has inherent limitations that detract from its therapeutic utility, with a narrow therapeutic index and variability in patients’ responses dependent on a range of factors including diet and concomitant drugs.3 In contrast, direct oral anticoagulants (DOACs) have relatively stable pharmacokinetics that remove the need for regular monitoring and dose adjustment.4 Recent non-inferiority trials assessing the efficacy and safety of DOACs compared with warfarin in the treatment of acute venous thromboembolism and prevention of recurrent venous thromboembolism have shown comparable efficacy without significantly increased risk of major bleeding.5678 However, trials are not typically designed to detect differences in safety outcomes. In addition, bleeding rates are underestimated in randomised trials,9 as patients with a history of bleeding are usually excluded. Population based comparative assessments of the safety of DOACs for treatment of venous thromboembolism are lacking. With DOACs being increasingly used in clinical practice, a need exists to better delineate their safety using real world, population based data sources to inform clinical practice.
We used a multicentre, population based, propensity score matched cohort of adults with incident venous thromboembolism to assess the safety (major bleeding and all cause mortality) of DOACs (dabigatran, apixaban, or rivaroxaban) compared with warfarin for the treatment of incident venous thromboembolism.
Methods
Study design and source population
We conducted a retrospective, propensity score matched cohort study using healthcare data from six jurisdictions (the Canadian provinces of Alberta, Manitoba, Ontario, Quebec, and Saskatchewan and the United States (MarketScan)) according to a prespecified common protocol (https://clinicaltrials.gov/ct2/show/NCT02833987).
Cohort definition
The study cohort included adults aged 18 years or over (66 years or over in Ontario) newly dispensed either a DOAC (apixaban, dabigatran, or rivaroxaban) or warfarin between 1 January 2009 and 180 days before the end date of the available database at each site (the latest end date was 31 March 2016). Patients were eligible for inclusion if they had a new diagnosis of venous thromboembolism, defined as at least one diagnostic code for venous thromboembolism within 30 days before the date of the first prescription for a DOAC or warfarin (the diagnosis ascertainment period). Our definition for venous thromboembolism included deep venous thrombosis and pulmonary embolism,101112 and we identified venous thromboembolism events by using hospital admission, emergency department, and/or physician claims databases. ICD (international classification of diseases) diagnosis codes from the 9th (ICD-9) and 10th (ICD-10-CA) revisions are shown in supplementary table A. We excluded patients who had a previous diagnosis of venous thromboembolism or atrial fibrillation 335 days or less before this first venous thromboembolism diagnosis, less than one year of information in the database before the date of the incident venous thromboembolism diagnosis, a prescription for a DOAC or warfarin within one year before the cohort entry date, or both a DOAC and warfarin prescribed on the date of their first prescription.
We defined cohort entry as the date of the first prescription for a DOAC or warfarin. We matched up to five warfarin users with each DOAC user. A warfarin user could serve as a match for more than one DOAC user, but only once. Matching was based on age at cohort entry (within one year either side), sex, date of cohort entry (within one year either side), and a propensity score reflecting the probability of being treated with a DOAC at the time of cohort entry (detailed below). We considered exposure to a DOAC or warfarin as a time fixed variable throughout the study follow-up.
Outcome definition
The primary outcome was time to an incident major bleed (see supplementary table A for a list of the validated ICD-9 and ICD-10-CA diagnosis codes), defined as first hospital admission or emergency department visit for intracranial, gastrointestinal, or other bleeding in the 90 days after cohort entry. This algorithm for major bleeding has 94% sensitivity and 83% specificity.1314 The secondary outcome was all cause mortality in the 90 days after cohort entry. We followed participants from cohort entry until the earliest of the major bleeding event, death, out-migration (out of the province for Canadian sites), or study end (defined as 90 days after the cohort entry for the primary analysis). We were unable to ascertain the outcome of mortality in the US MarketScan database, as this information was unavailable.
Covariates
Information on demographic characteristics and comorbid conditions came from the healthcare data files of the included sites. We defined comorbid conditions a priori on the basis of previous research,15 and we defined clinical expertise by inpatient or outpatient ICD-9 and ICD-10-CA diagnosis codes based on information available for the 365 days before cohort entry. Comorbid conditions included diabetes, hypertension, chronic kidney disease, acute kidney injury, history of cardiovascular disease (including ischaemic heart disease, congestive heart failure, cardiomyopathy, valvular heart disease, and pacemaker or defibrillator), peripheral vascular disease, cerebrovascular disease (including transient ischaemic attack and all stroke subtypes), chronic obstructive pulmonary disease, liver disease, and cancer. We also included history of major bleeding (hospital admission or emergency department visit in the previous 365 days) and residence in long term care (for sites that could identify this). Antiplatelet agent, non-steroidal anti-inflammatory drug, or gastroprotective drug use, defined as at least one dispensed prescription within 90 days before cohort entry, came from prescription drug records.
Statistical analysis
We developed a multivariable logistic regression model that included demographic information, comorbid conditions (listed above), and prescription antiplatelet agents, non-steroidal anti-inflammatory drugs, and gastroprotective drugs to estimate the probability (propensity) of being treated with a DOAC, conditional on the included covariates. We excluded 5% of patients at each end of the propensity score distribution. We matched up to five warfarin users with each DOAC user (with replacement) on age at cohort entry date, sex, cohort entry date, and the propensity score (based on a calliper width of 0.02 of the log odds of the propensity score). We assessed the balance in the covariates between the DOAC and warfarin exposure groups before and after matching by using the standardised mean difference (expressed as a percentage), whereby an absolute standardised mean difference below 10% implied acceptable balance.16
We fitted a shared frailty model based on the matched cohort to estimate hazard ratios of study outcomes (and their 95% confidence intervals) in the 90 days after cohort entry among patients dispensed prescriptions for DOACs, using warfarin as the reference treatment. This model accounts for the clustering of individuals in the matching process and is akin to a random effects survival model.17 We constructed separate models to assess the risk of major bleeding and all cause mortality associated with DOAC use compared with warfarin use. Analyses were conducted independently at each study site using linked, encoded data and SAS software.
Secondary analyses
In secondary analyses, we assessed the risk of major bleeding associated with DOACs compared with warfarin for the treatment of incident venous thromboembolism according to chronic kidney disease status (defined on the basis of on a validated algorithm, using ICD-9 (403 and 585) and ICD-10-CA (E102, E112, E132, E142, I12, I13, N08, N18, and N19) codes).181920 We also assessed the risk of major bleeding and all cause mortality outcomes associated with DOAC use compared with warfarin use stratified by age group (≤65, 66-75, 76-85, and >85 years) and sex.
Sensitivity analyses
We did several sensitivity analyses to confirm the robustness of our findings. We repeated all analyses using a venous thromboembolism diagnosis ascertainment period of 15 days, excluding all patients with a diagnosis of venous thromboembolism or atrial fibrillation during a period of 1065 days before the new venous thromboembolism diagnosis, and using an extended duration of follow-up (180 days).
Meta-analysis
Analyses were conducted independently at each participating site according to a common analytical protocol and then pooled using meta-analysis techniques with a fixed effects model, which assumes that variation between studies is the estimate associated with sampling error. We calculated inverse variance weighted pooled risk estimates and 95% confidence intervals. We used Review Manager software, version 5.3, for analyses.
Exclusion of Clinical Practice Research Database and province of Nova Scotia
As specified in the study protocol, we had sought to include data from the UK based Clinical Practice Research Database (CPRD). However, the results on mortality obtained in the CPRD were clearly different from those at other sites. On review of the literature on venous thromboembolism and mortality using the CPRD,21 we determined that mortality from venous thromboembolism based on CPRD data are substantially underestimated using the general practice electronic records.22 We therefore excluded CPRD data. We also sought to include data from the Canadian province of Nova Scotia. However, owing to the small size of the matched cohort (n=60), the limited number of major bleeding events observed across the DOAC and warfarin exposure groups (none observed in the DOAC group), and the subsequent non-convergence of models and limited ability to do additional secondary and sensitivity analyses, we excluded Nova Scotia from all analyses.
Patient involvement
This study involved the secondary use of existing data sources and did not include patients as study participants. No patients were involved in setting the research question, the study design, or the overall conduct of the study. There are no plans to involve patients in the dissemination of study findings.
Results
Patients’ characteristics
We identified 148 972 adults aged 18 years or over with a new prescription for a DOAC (n=13 813; 9.3%) or warfarin (n=135 159; 90.7%) and an incident diagnosis of venous thromboembolism within 30 days before this prescription (fig 1⇓). Of these, we included 59 525 adults in the matched analyses (12 489 (21.0%) DOAC users; 47 036 (79.0%) warfarin users). Overall, after matching, balance was achieved across all included covariates (supplementary table B). The mean age of the matched cohort (n=59 525) was 64.3 (SD 15.9) years, and 53.6% were female (table 1⇓). Among DOAC users, most prescriptions were dispensed between 2013 and 2015 (88.8%) and rivaroxaban was the most common DOAC used overall (94.9%). The proportion of patients who switched from DOACs to warfarin or from warfarin to DOACs during the follow-up period was small (374 (3.0%) and 2476 (5.3%), respectively).

Fig 1 Flow chart for defining study cohort. Cells of tables with patient counts <5 were suppressed (S) by participating sites owing to privacy restrictions. The sum of count data may thus differ slightly from the presented total
{kind=link}
Baseline characteristics of overall study population (patients with incident VTE newly prescribed DOACs or warfarin), matched and unmatched on propensity score*. Values are numbers (percentages) unless stated otherwise
Incidence rates of major bleeding and all cause mortality
Over a mean follow-up of 85.2 days, 1029 (1.7%) deaths occurred and 1967 (3.3%) patients had a major bleed, of which 131 (6.7%), 758 (38.7%), and 1070 (54.6%) were due to an intracranial, gastrointestinal, and other bleed, respectively. Bleeding rates at 30 days ranged between 0.2% and 2.9% for DOACs and 0.2% and 2.9% for warfarin. Bleeding rates at 60 days ranged between 0.4% and 4.3% for DOACs and 0.4% and 4.3% for warfarin.
Hazard ratios for major bleeding and all cause mortality
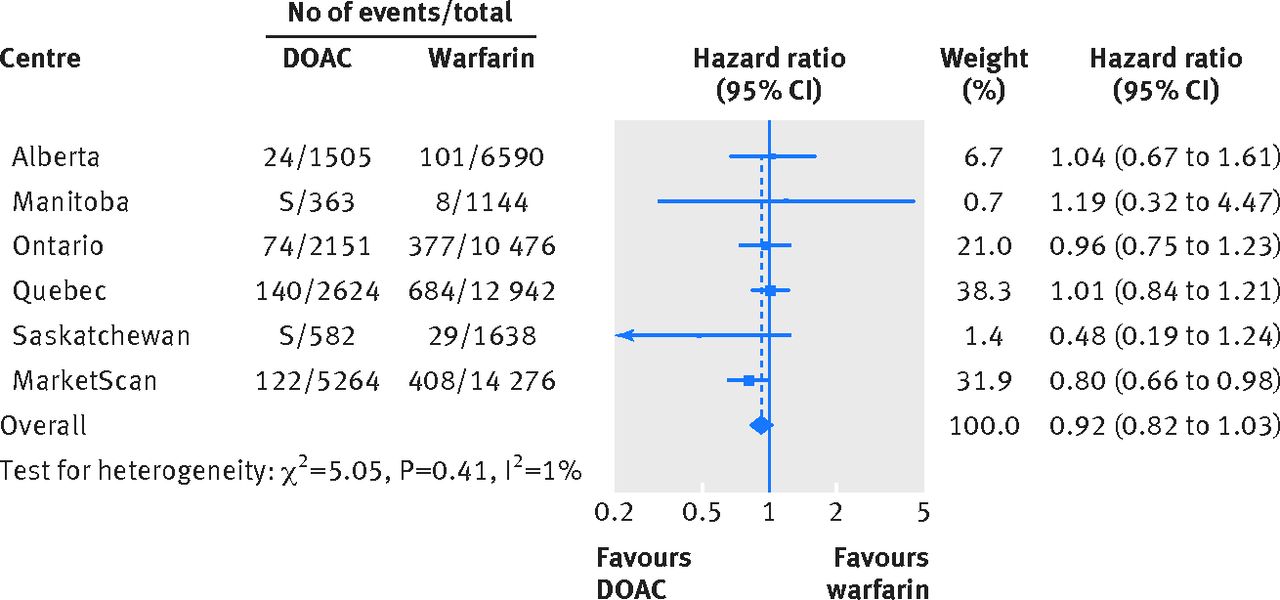
Overall, the risk of major bleeding associated with DOAC use among patients with incident venous thromboembolism was similar to that with warfarin use (hazard ratio 0.92, 95% confidence interval 0.82 to 1.03; fig 2⇓), with the direction of the association favouring DOACs. We observed no evidence of heterogeneity across included sites (I2=1%, P for heterogeneity=0.41). We observed similar results for the outcome of all cause mortality (hazard ratio 0.99, 0.84 to 1.16; I2=0%; P for heterogeneity=0.66; fig 3⇓).

Fig 2 Hazard ratios (95% CIs) of major bleeding associated with direct oral anticoagulant (DOAC) use compared with warfarin use (reference category was warfarin users). S=events were <5 and cells were suppressed
{kind=link}
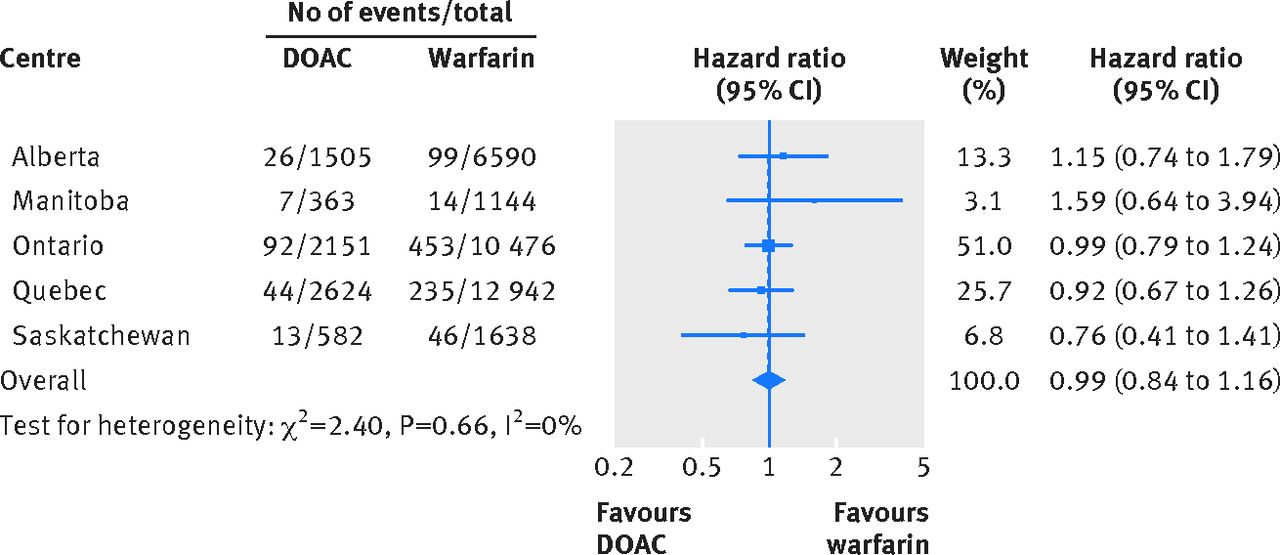
Fig 3 Hazard ratios (95% CIs) of all cause mortality associated with direct oral anticoagulant (DOAC) use compared with warfarin use (reference category was warfarin users)
{kind=link}
Hazard ratios for major bleeding and all cause mortality according to chronic kidney disease status, age groups, and sex
We found no significant heterogeneity in the risk of major bleeding and all cause mortality associated with DOAC use when we assessed patients according to chronic kidney disease status (fig 4⇓), age (supplementary figures A and B), and sex (supplementary figure C).

Fig 4 Hazard ratios (95% CIs) of major bleeding and all cause mortality associated with DOAC use compared with warfarin use according to chronic kidney disease (CKD) status (reference category was warfarin users). S=events were <5 and cells were suppressed. Some sites were not included in analysis owing to small number of DOAC users identified as having CKD (Manitoba and Saskatchewan) or small number of events observed across DOAC and warfarin groups (including zero events in DOAC group)
{kind=link}
Sensitivity analysis
Overall results remained unchanged in all sensitivity analyses, including when a longer period of follow-up (180 days) was used (supplementary figures D and E).
Discussion
In our multicentre, population based, propensity score matched cohort study of 59 525 adults with incident venous thromboembolism, we observed that treatment with DOACs compared with warfarin was not associated with an increased risk of major bleeding or all cause mortality in the first 90 days of treatment. We found similar results for patients with and without chronic kidney disease, across all age groups, and for men and women.
Implications and comparison with other studies
Randomised trials assessing the efficacy and safety of DOAC use compared with vitamin K antagonists for the treatment of venous thromboembolism have shown favourable risk-benefit profiles for DOAC treatment.23 Although we did not observe a lower risk of major bleeding with DOAC treatment in our study, given the absence of an increased bleeding risk and the advantages associated with its use particularly around frequency of monitoring and dosing, our results suggest that DOACs may be considered as a treatment option for patients with venous thromboembolism who are candidates for anticoagulation.
A recent systematic review assessing the efficacy and safety of DOACs for the treatment of acute venous thromboembolism based on data from nine trials (28 554 participants and 228 major bleeding events) showed that bleeding risks were either similar (hazard ratio for dabigatran versus warfarin 0.76, 95% confidence interval 0.48 to 1.18) or reduced (hazard ratio for apixaban and rivaroxaban versus warfarin 0.33 (0.18 to 0.56) and 0.55 (0.37 to 0.80), respectively) for DOAC use compared with warfarin.24 The study also reported no differences in the risk of all cause mortality with DOAC use. Large studies on the assessment of the safety of DOAC for the treatment of venous thromboembolism in routine clinical practice have been limited. Several relatively small cohort studies of rivaroxaban have reported similarly favourable safety profiles associated with its use in patients with venous thromboembolism.92526272829 In addition, a recent cohort study of 12 318 venous thromboembolism patients comparing 5411 rivaroxaban users with 6907 vitamin K antagonist users showed no difference in major bleeding risk (hazard ratio 1.08, 0.84 to 1.39). However, these studies are limited by their small sample size (n=361 to 4768 patients2527283031), lack of a comparator,2629 and inclusion of cases of major bleeding in patients admitted to hospital only, which probably led to an underestimation of the bleeding rates.32 Our study, using a large population based cohort of DOAC and warfarin users in whom major bleeding was identified across in-hospital and emergency department data sources, has thus important implications for the management of patients with venous thromboembolism at risk of having a recurrent event.
However, DOAC use has also been associated with increased risk of bleeding in relation to specific subtypes of bleeding episodes, including gastrointestinal bleeding, in other patient populations including those with atrial fibrillation.333435 A systematic review of 43 trials including patients with venous thromboembolism, atrial fibrillation, and acute coronary syndrome and those who had received orthopaedic surgery showed that the overall risk of gastrointestinal bleeding was 45% (95% confidence interval 7% to 97%) greater in patients treated with DOACs than in those who received standard care such as treatment with warfarin or low molecular weight heparin.34 Among venous thromboembolism patients only, treatment with DOACs increased the risk of gastrointestinal bleeding by 59% (3% to 244%) compared with standard care, although only two trials reported data on patients with venous thromboembolism. Our results show no increased risk of gastrointestinal bleeding associated with DOAC use.
Although our analysis of the safety of DOACs according to chronic kidney disease status showed similar bleeding risks across DOAC and warfarin groups, the safety profile of DOACs can vary by agent type depending on the percentage renal excretion. A systematic review assessing the safety of DOACs in patients with an estimated glomerular filtration rate of less than 50 mL/min showed that the magnitude of relative reduction in major bleeding with DOAC use compared with warfarin was linearly associated with percentage renal excretion of the agent.36 The greatest relative reduction of major bleeding was observed for DOACs with renal excretion below 50% (including rivaroxaban and apixaban), whereas those with renal excretion above 50% (such as dabigatran) showed no reduction in the risk of major bleeding compared with warfarin.
Strengths and limitations of study
Our study formally pooled results from multiple healthcare settings, contributing to the generalisability of our findings. In addition, we assessed the safety of new DOAC and warfarin use, which removes the biases associated with safety assessments of prevalent drug use such as the underestimation of bleeding events.
Our study has some limitations. Despite the achieved balance in the included range of variables, owing to the observational nature of our study design, the possibility of residual confounding arising from differences in unmeasured variables remains. Although we assessed study outcomes within 90 and 180 days, the longer term safety of DOAC treatment for venous thromboembolism is less certain. Furthermore, most (95%) DOAC users in our study used rivaroxaban, so we were unable to assess the safety of DOACs among venous thromboembolism patients by different DOAC agents. Future studies assessing the safety of other DOAC agents for the treatment of venous thromboembolism, including apixaban and dabigatran, are needed. Among warfarin users who had a major bleeding event, owing to the limited availability of international normalised ratio measurements in the study cohort, we were unable to determine the time within the therapeutic range or to adjust for over the counter use of aspirin or other non-steroidal anti-inflammatory drugs.
Our algorithm for treated venous thromboembolism did not allow for an assessment according to deep venous thrombosis and pulmonary embolism status; nor could we differentiate distal from proximal venous thromboembolism or subsegmental from proximal pulmonary embolism. However, given the inclusion of oral anticoagulation as part of our venous thromboembolism algorithm, all events included in our study were associated with a treatment indication. Although the duration of DOAC or warfarin use was not assessed, given the short length of follow-up (90 days), the incident nature of the venous thromboembolism diagnosis, and the guideline recommended treatment of venous thromboembolism of at least 90 days,37 substantial misclassification of drug exposure is unlikely. The potential exists for misclassification of chronic kidney disease status based on ICD codes, but the high specificity of this algorithm (99%18) would suggest that the small number of chronic kidney disease patients who may be misclassified would be minimal. Nonetheless, given the use of administrative codes, we were limited in our ability to ascertain whether a differential association between major bleeding risk and DOAC use exists according to level of kidney function. Additional studies are needed to further elucidate the safety of DOACs among venous thromboembolism patients with advanced chronic kidney disease. Although we used matching with replacement of warfarin users to maximise the number of DOAC users retained in the cohort, this results in a lack of independence among the warfarin users. However, we did sensitivity analyses that showed no effect on the precision of study findings. Finally, a random effects model for combining effect size estimates could have been selected instead of a fixed effects model. The former assumes that variation in effect size estimates can be attributed to both between study and within study variation. The selection of a random effects model can result in slightly larger confidence intervals and hence a more conservative test. However, the selection of a random effects model had no effect on the final conclusions as regards statistical significance.
Conclusions
In this analysis of data from large cohorts of adults with incident venous thromboembolism, treatment with DOACs, compared with warfarin, was not associated with an increased risk of major bleeding or all cause mortality in the first 90 days of treatment. These results were consistent for patients with and without chronic kidney disease, across all age groups, and for men and women.
What is already known on this topic
Non-inferiority randomised trials have shown similar efficacy and a reduced or similar risk of major bleeding complications for direct oral anticoagulants (DOACs) compared with warfarin in the treatment of venous thromboembolism
Clinical trials include a highly selected patient group, so the rate of safety events such as major bleeding reported in trials often does not reflect those observed in routine clinical practice
What this study adds
This large multicentre, population based study suggests that DOAC use is not associated with higher major bleeding risk in venous thromboembolism
A series of sensitivity and subgroup analyses ensured the robustness of study findings and showed consistent findings in different patient groups
Footnotes
Canadian Network for Observational Drug Effect Studies (CNODES) Investigators: Samy Suissa (principal investigator); Colin R Dormuth (British Columbia); Brenda R Hemmelgarn (Alberta); Gary F Teare (Saskatchewan); Patricia Caetano and Dan Chateau (Manitoba); David A Henry and J Michael Paterson (Ontario); Jacques LeLorier (Québec); Adrian R Levy (Atlantic: NS, NL, NB, PEI); Pierre Ernst and Kristian B Filion (UK CPRD); Robert W Platt (methods); and Ingrid S Sketris (knowledge translation).
We acknowledge the contributions of Alexis Matteau (Quebec) and the programming support of Zhihai Ma and Jianguo Zhang (Alberta), Sophie Dell'Aniello (CPRD), Yan Wang (Nova Scotia), Caixia Fangyun Wu (Ontario), Thierry Ducruet (Quebec), Nianping Hu (Saskatchewan), and Gregory A Carney (US MarketScan). We also acknowledge the important contributions of the CNODES collaborators and assistants at each site. This study was made possible through data sharing agreements between CNODES member research centres and the respective provincial governments of Alberta, Manitoba (HIPC # 2015/2016 – 47), Nova Scotia, Ontario, Quebec, and Saskatchewan. The opinions, results, and conclusions reported in this paper are those of the authors. No endorsement by the provinces is intended or should be inferred. Parts of this material are based on data and information compiled and provided by the Canadian Institute for Health Information (CIHI). However, the analyses, conclusions, opinions, and statements expressed herein are those of the authors and not necessarily those of CIHI.
Contributors: MJ, LML, MDurand, MDahl, MJP, CRD, PE, SY, HT, SMM, and BRH were responsible for study concept and design; data collection, analysis, and interpretation; and manuscript preparation. MJ and BRH drafted the initial manuscript, and all authors contributed to data interpretation and critical revision of the report. BRH is the guarantor.
Funding: MJ was supported by postdoctoral fellowships from the Canadian Institutes of Health Research (CIHR) and Alberta Innovates Health Solutions (AIHS) and an early career fellowship from the National Health and Medical Research Council of Australia (NHMRC). MDurand is supported by a salary award from the Fonds de Recherche du Québec-Santé. BRH was supported by the Roy and Vi Baay Chair in Kidney Research. LML was supported by a Manitoba Research Chair. CNODES, a collaborating centre of the Drug Safety and Effectiveness Network (DSEN), is funded by the CIHR (grant number DSE-146021). The funding organisations had no role in the design and conduct of the study; in the collection, analysis, and interpretation of the data; or in the preparation, review, or approval of the manuscript.
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare: support for the submitted work as described above; CW has received honorariums (for advisory board meetings as well as speaking engagements) from Leo Pharma and Pfizer (makers of tinzaparin and dalteparin, respectively); SMM has received research grants for work unrelated to this project from GlaxoSmithKline, Merck, Pfizer, and Sanofi; no other relationships or activities that could appear to have influenced the submitted work.
Ethical approval: The study protocol was approved by the institutional review boards at all participating sites and by the Independent Scientific Advisory Committee (ISAC; protocol number 16_110R) of the CPRD. The study protocol is registered at www.clinicaltrials.gov (NCT02833987). The data are anonymous, and the requirement for informed consent was therefore waived.
Data sharing: No additional data available.
Transparency: The lead author affirms that the manuscript is an honest, accurate and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.