What's new in the other general journals
BMJ 2005; 331 doi: https://doi.org/10.1136/bmj.331.7519.721 (Published 29 September 2005) Cite this as: BMJ 2005;331:721
- Alison Tonks, associate editor (atonks{at}bmj.com)
US funding for biomedical research has doubled since 1994
It is difficult to get a detailed picture of funding for biomedical research. The whole enterprise is too vast, the funding too varied, and the record of funding too patchy. In the latest attempt to pin down who pays and how much, the researchers report that in the United States yearly investment in biomedical research doubled to more than $94bn (£52bn; €77bn) between 1994 and 2003. Industry, including manufacturers of drugs and devices, and biotechnology companies invested 57% of the total, and the National Institutes for Health—the next largest payer—invested 28%. Other government sources, charities, independent foundations, and free standing research institutions account for most of the rest.

The proportion of biomedical research paid for by industry has changed little during the past 10 years, but the pharmaceutical industry has shifted its focus away from preclinical research and towards clinical trials. It has also become less innovative, producing fewer new chemical compounds each year and lagging behind the more productive medical devices sector.
The authors of the report estimate that 5.6% of all US health expenditure goes on biomedical research, a large investment that is poorly targeted and badly monitored. Better data, and tracking where the money comes from and goes to, would help. But the biggest challenge for sponsors is to change the way they invest so that research money is systematically channelled into areas of greatest clinical need.
JAMA 2005;294: 1333-42
Choosing between second generation antidepressants for people with major depression is still difficult
All new generation antidepressants work better than placebo for patients with major depression, but there doesn't seem much to choose between them. A systematic review of 46 head to head trials found few important differences in response rates between a range of antidepressants that included selective serotonin reuptake inhibitors, venlafaxine, bupropion, duloxetine, and mirtazapine. The type of side effects varied from drug to drug, but the overall incidence of side effects did not.
Almost all (96%) of these trials were sponsored by the pharmaceutical industry or led by researchers with financial ties to the industry. Sponsorship was associated with a 5% advantage for the sponsor's drug over the comparator drug, and publication bias obscured the evidence even further.
So despite a huge amount of effort, people with major depression and their doctors still do not have enough unbiased information to make an informed choice about treatment. The authors and the American Psychiatric Association say the final word should go to patients, after a detailed discussion about the kind of side effects they might prefer. The trials in this review suggest that venlafaxine is more likely than selective serotonin reuptake inhibitors to induce nausea (mean incidence 31%, 95% CI 27% to 34%) and that paroxetine, sertraline, and mirtazapine are more likely than bupropion to upset patients' sex lives.
Annals of Internal Medicine 2005;143: 415-26
Neural tube defects are common in rural India
To find the incidence of neural tube defects in some of the poorest villages in India, researchers recruited local women to knock on doors and interview new mothers and their relatives, armed with an album of explanatory photographs. A careful search in a representative sample of 30 villages found 10 babies born with neural tube defects in the previous year, one affected baby for every 121 live births. The three with anencephaly had died, but seven others were still alive at the time of the survey (four with closed spina bifida, two with open spina bifida, and one with an occipital meningocele).
The researchers estimate that the incidence of neural tube defects in this population is between 6.6 and 8.2 per 1000 live births, one of the highest rates in the world. The true incidence is likely to be even higher; stillborn babies were excluded from this study because new mothers often don't see them.
Maternal deficiencies in folate must be responsible for at least part of the excess incidence in these rural villages. But no government policies as yet acknowledge the problem or take steps to remedy it.
Lancet 2005;336: 930-1
Academic medicine in US may be recovering
Medical academics are a rare breed in the United States, and they are getting older. Fortunately, government and other initiatives to attract more doctors into medical research seem to be having some success, says a recent report. Data from the National Institutes of Health (NIH), the Association of American Medical Colleges, and the American Medical Association show that, although the US has no more medical academics now than in 1995 (14 340) and considerably fewer than in 1985 (23 680), increasing numbers of graduating students are at least thinking about a career in research. Interest in an academic career has increased slowly but steadily since about 1997—possibly because debt relief programmes now exist for young academics to help keep them afloat during the first few years of low pay. American medical students graduate with an average debt of over $100 000 (£56 000; €82 000), and tuition fees are increasing faster than wages.

Over 2000 young researchers were awarded debt relief during the first four years of these programmes. If their success is sustained and debt relief programmes continue or expand, this new blood could eventually halt the relentless ageing of the US academic community. The change will not be evident for a while, however. In 2004 the NIH still awarded 44% of its research grants to academics aged over 50.
JAMA 2005;294: 1343-51
Online drugs cheaper from Canadian than US websites
Many Americans buy their prescription medicines online from Canada because they think it's cheaper than buying them online from pharmacies in their own country. They are right. A study comparing online pharmacies in both countries found that brand name drugs were 24% cheaper in Canada than in the United States, so buying from Canada saves US consumers an average of US$0.76 (£0.42; €0.63) per pill. Patients buying the Zyprexa brand of olanzapine saved most ($1159 a year), but savings were also substantial for patients taking 40 of the 43 other drugs studied, especially pioglitazone (Actos; saving $852) and esomeprazole (Nexium; $722). For 80% of drugs, even the most expensive Canadian pharmacy was cheaper than the cheapest US pharmacy.

Drug treatments for erectile dysfunction were the only drugs that were more expensive in Canada, with an average yearly cost to US consumers (based on 48 pills annually) of $550. The corresponding cost from US pharmacies was only $476.
The study included 44 of the 50 most popular drugs bought online, and it compared 12 Canadian pharmacies with the three largest US pharmacies with online capability. The authors, who are Canadian, say the differences are probably due to price controls set by the Canadian government. Controls are absent in the US, and drug manufacturers can charge whatever the prevailing market will allow.
Annals of Internal Medicine 2005;143: 397-403
Home support is essential for breastfeeding women in Brazil
Many new mothers need encouragement and support to breast feed successfully. Sustained support starting in hospital and continuing at home worked best in a randomised trial from a poor area of Brazil. The 350 women had their babies in two hospitals staffed by midwives who had been trained to encourage breast feeding. After discharge, 175 women were visited regularly by community workers, who encouraged them to continue exclusive breast feeding for at least six months. The other women had no professional help with breast feeding after they left hospital.
Overall, 70% (244/349) of the babies were exclusively breast fed in hospital. Ten days after discharge, that had to fallen to just 30% (53/175) in the group without home support. Exclusive breastfeeding was down to 15% (26/168) by the end of the first month at home. Only 13% of the women without home visits managed to breast feed exclusively for the full six months, compared with 45% of the women who had home visits (P < 0.0001)
The researchers conclude that a good start in hospital has a limited impact on breast feeding once the mother goes home. Continued support is particularly important in poorer communities, such as this one, where women stay in hospital for only 24-36 hours after the birth.
Lancet 2005;366: 1094-100
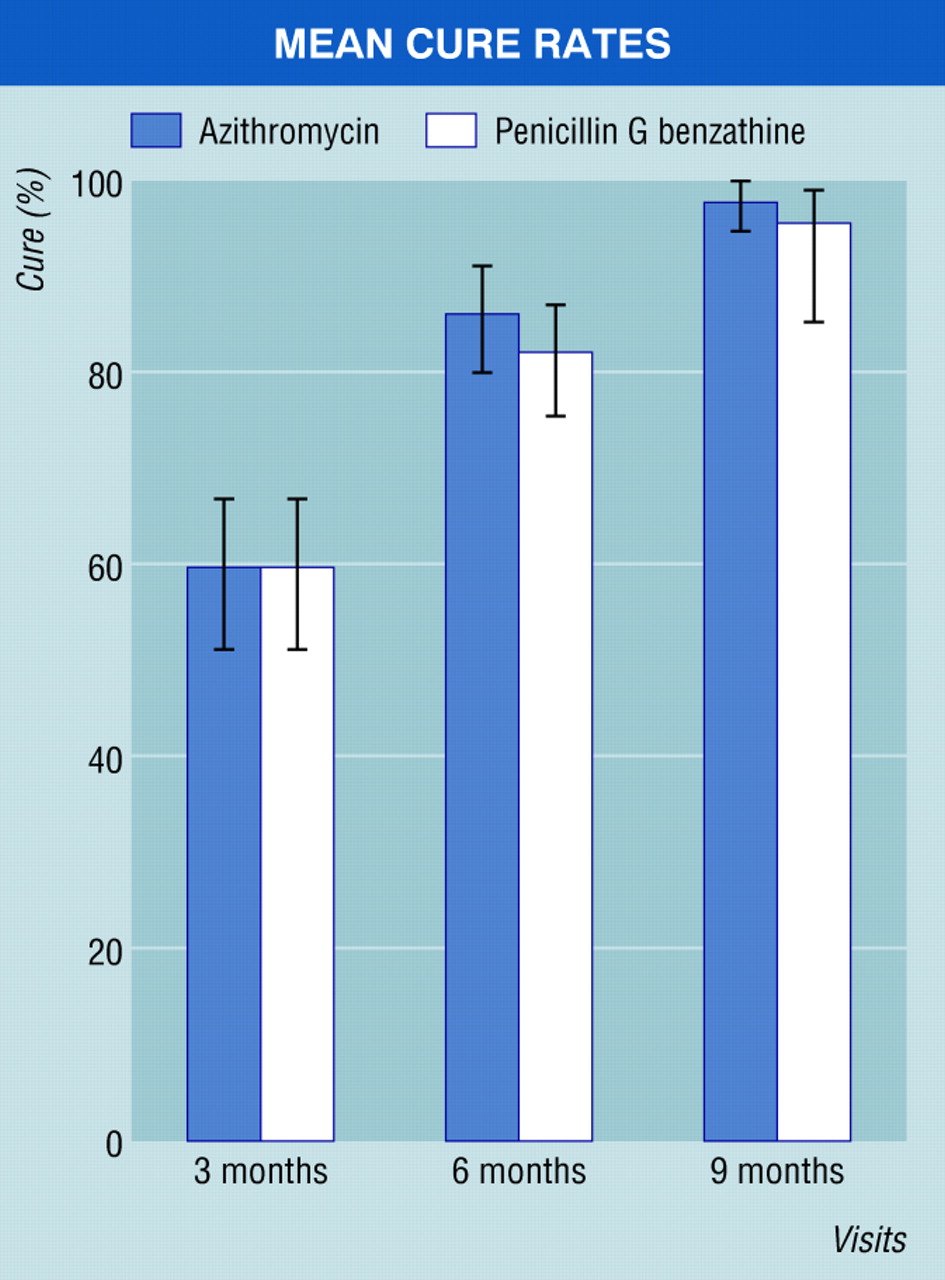
Penicillin should remain the standard treatment for early syphilis—for now
A single 2 g dose of oral azithromycin sounds like a better treatment for early syphilis than a high volume (4 ml) injection of intramuscular penicillin G. The oral treatment works just as well, according to a randomised trial from Tanzania, and it's more convenient than the standard intramuscular treatment, especially where trained staff and injecting equipment are in short supply.
Penicillin G has been a safe and effective treatment for early syphilis for over 50 years. Is it time for a change to azithromycin? A linked editorial (p 1291-3) from the US warns against it. Previous attempts to control syphilis with azithromycin in high risk populations in Vancouver, Canada, had a modest and short lived impact. Worse, there have been a series of high profile treatment failures caused by antibacterial resistance in the US and Ireland. There's no evidence of resistant Treponema pallidum in the developing world, but researchers have yet to look carefully for it. The patchy success of azothiaprine treatment programmes and the very real threat of resistance contrasts starkly with the excellent and sustained results given by intramuscular penicillin. The editorial concludes that it's too early to think about a wholesale change in policy in Africa, or anywhere else.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
New England Journal of Medicine 2005;353: 1236-44
Obese women with breast cancer do worse after reduced dose chemotherapy
Reanalysis of data from four randomised trials suggests that obese women with breast cancer may be getting a lower dose of chemotherapy than they need. Oncologists often reduce the recommended dose of chemotherapy (which is calculated from patients' body surface area) because of concerns about toxicity. In these trials, which were done between 1978 and 1993, 39% (97/249) of women with a body mass index of 30 or more were given a reduced dose, compared with only 16% (298/1891) of women with a body mass index less than 30 (P < 0.0001). Most women had cyclophosphamide, methotrexate, and 5-fluorouracil.
The reduced dose mattered most for obese women with cancers that were negative for oestrogen receptors. In this group, women who received less than 85% of the full recommended dose of chemotherapy had shorter disease-free survival (hazard ratio 0.55, 95% CI 0.33 to 0.93) and shorter overall survival (0.5, 0.28 to 0.88) than women who received more than 85%. Reducing the dose did not reduce the incidence of serious side effects in these women.
Lancet 2005;366: 1108-10