Relief of pain
BMJ 1999; 318 doi: https://doi.org/10.1136/bmj.318.7188.927 (Published 03 April 1999) Cite this as: BMJ 1999;318:927
- Inger Findley,
- Geoffrey Chamberlain
Labour is usually painful. Exceptionally, a very few women may not feel pain; others can control their response so as to reduce pain. Most women think that pain is going to be a major part of giving birth. Professionals can help to reduce women's fears by giving precise, accurate, and relevant information beforehand and explaining what pain relief will be available at the place where the woman will be in labour. If a women has plans about the sort of pain relief she wants, these should be discussed in advance with the woman and her partner.
Causes of labour pain
Stretch of the cervix during dilatation
Ischaemia of the muscle wall of the uterus with build up of lactate
Stretch of the vagina and perineum in the second stage
Percentages of women using pain relief (based on the reports of the National Birthday Trust surveys)
The National Birthday Trust has performed nationwide surveys since the second world war, and the table shows the proportions of women going through labour using various methods of analgesia. Chloroform and trilene are no longer used; pethidine achieved a popularity that is now waning;nitrous oxide is a mainstay; and epidural and spinal methods are increasing in use.

Equipment for self administration of nitrous oxide and oxygen (Entonox) with a mouth piece (top) and a face mask (bottom
The trust's 1990 report, Pain Relief in Labour, is based on the experiences of over 10 000 women who delivered in the United Kingdom during one week. It is the best source of national statistics on both pharmacological and non-pharmacological analgesics. Much of this article is based on the report; some practices may have changed in the years since the survey—for example, the increased use of epidural and spinal anaesthesia for caesarean section.
Pharmacological methods
Nitrous oxide
Premixed nitrous oxide and oxygen is now provided as Entonox. It is a 50:50 mixture and is available at virtually all places of delivery.
Nitrous oxide is self administered, but women cannot take too much as the flow stops before consciousness is lost. The mixture improves fetal oxygeneration and has a very short half life. About 85% of women find it helpful.

Percentage of women using nitrous oxide by distribution of numbers of labour units in Britain
Pethidine
This analgesic and antispasmodic drug is usually given intramuscularly (50-150 mg). It is decreasing in popularity as nausea, drowsiness, and lack of control are important adverse effects.
Pethidine is considered a better analgesic by professionals than by women themselves. It works when given intramuscularly in about 20 minutes, giving good pain relief for some and sedation for most. Because a fifth of women are nauseous with pethidine, an antiemetic—for example, metoclopramide 10 mg—is commonly given at the same time.

Percentage of women using pethidine by distribution of numbers of labour units in Britain
Pethidine crosses the placenta and is a neonatal respiratory depressant. It should be avoided in the last two hours of labour, but this is sometimes hard to judge. Naloxone reverses its effect, and the subject is considered in a later article in this series.
Morphia and diamorphine
Opiates are still used for pain relief in labour in about 5% of women in Britain, usually if epidural analgesia is not available; some 85% of women experience good pain relief with them, but they have depressive effects on neonatal respiration. In addition, morphine is frequently used after a caesarean section, via patient controlled pumps.
Epidural analgesia
Epidural analgesia provides the most effective pain relief. An indwelling plastic catheter is introduced into the epidural space through a needle with a curved tip. After the initial dose, analgesia can be extended with intermittent top ups by midwives or increasingly by the patient herself. Epidural analgesia can be given by continuous infusion via a syringe pump. It is used by about a fifth of women in England and Wales.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Traditionally, analgesia is produced with a local anaesthetic agent such as bupivacaine. This may cause motor blockade, which can be distressing. By reducing the concentration of local anaesthetic and adding an opiate such as fentanyl, good pain relief can be given in many cases with sparing of motor function. This technique is called a mobile epidural. It is not yet available in all centres.
An epidural service requires full cardiorespiratory resuscitation facilities and resident anaesthetic staff and so may not be available in small hospitals. Epidural analgesia has a very high acceptance rate: in the National Birthday Trust's latest survey over 90% of women found it to be good or very good and 85% would choose it again.
Mobile epidurals
Analgesia with bupivacaine affects motor function, leading to weakness of the lower limbs
Decreasing the concentration and adding an opiate provides good pain relief with sparing of motor function
Ambulatory epidural service is not yet available in all centres

Percentage of women wishing to use epidural at next delivery
{kind=link}

Percentage of units in United Kingdom reporting 24 hour epidural cover for labour, 1994
{kind=link}
Epidurals have some potential disadvantages. The dura may be accidentally punctured; this happens in less than 1% of cases, but it causes a severe postural headache in about 80% of these. This can be cured in most cases with an autologous epidural blood patch; the blood clots in the epidural space and presumably works by sealing the leak of cerebrospinal fluid, thus restoring intracranial pressure. Any severe case of headache after epidural should always be referred to the anaesthetist.
Rates of instrumental delivery may be higher among women using an epidural because in the more painful prolonged labours with malpositions women are more likely to receive epidural analgesia
Urinary retention after an epidural is best prevented by careful attention to bladder emptying
There is debate about backache after epidurals. Backache mostly occurs in patients with pre-existing problems that are exacerbated by pregnancy. Nevertheless, women should be warned of the possibility of back pain so that strain on the back can be avoided by careful positioning during the epidural.
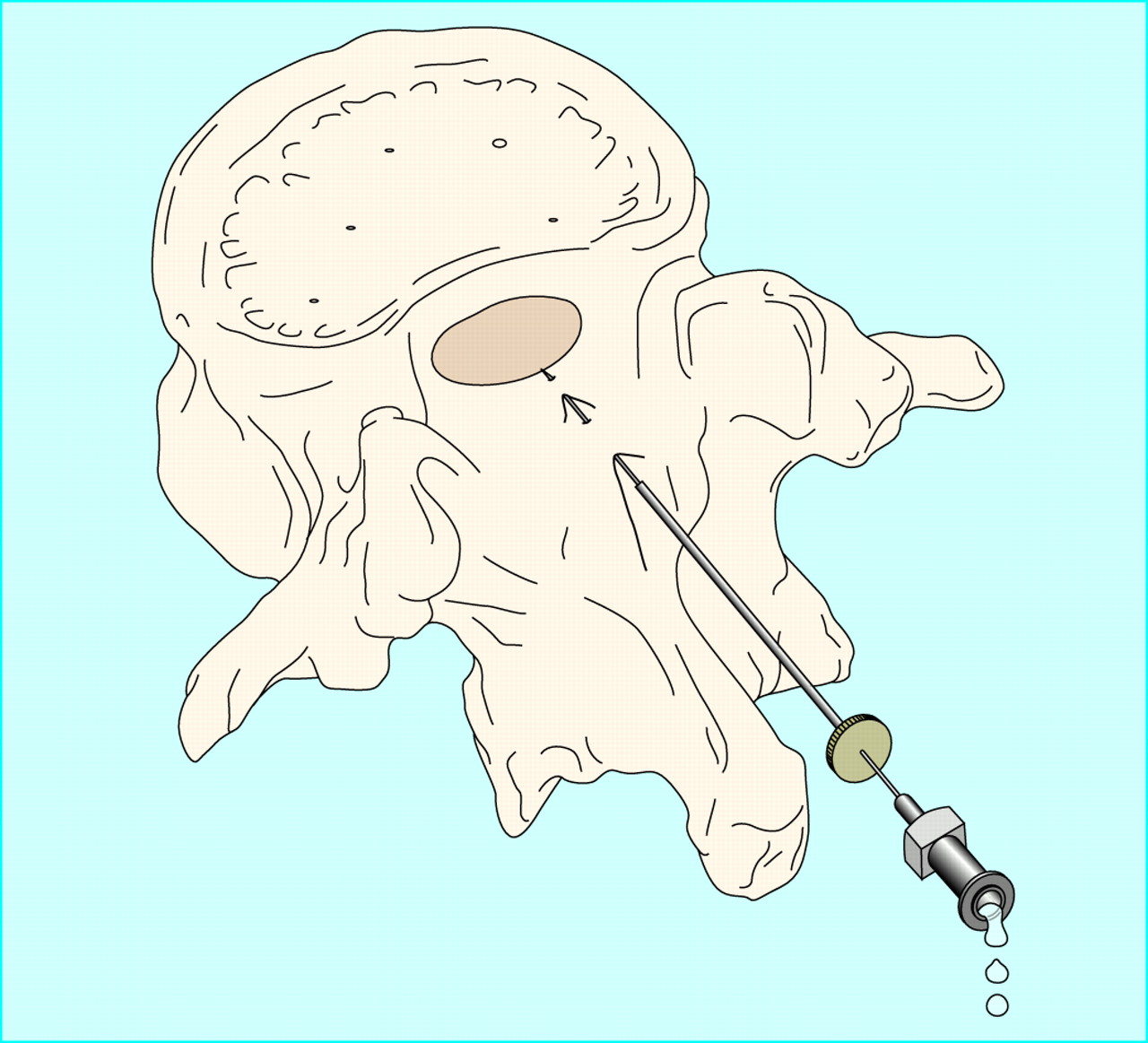
Spinal anaesthesia
Spinal anaesthesia is increasingly used for operative procedures: caesarean section, instrumental delivery, and manual removal of the placenta. The local anaesthetic is injected into the cerebrospinal fluid through a very fine (25G) atraumatic needle. The onset of action is rapid, and the effect lasts for about two hours. Headache after a spinal injection is rare nowadays.

Siting of spinal anaesthetic with specially pointed atraumatic needle
{kind=link}

Differentiation of regional blocks (usually done by anaesthetist) and field blocks (commonly performed by obstetrician)
{kind=link}
Nerve blocks
A pudendal nerve block with lignocaine plus an infiltration of the perineum with local anaesthetic gives good pain relief for low cavity, forceps, or vacuum extraction, but it would be unkind to use Keilland's forceps, which should be reserved for use with an epidural or spinal block. Local nerve block is an easy technique, which is performed by the obstetrician at the time of delivery, and has few complications. Repair of an episiotomy is readily done under this type of analgesia.

Pudendal block technique. The injection is into the pudendal nerve in the region of the ischial spine each side. The nerve usually leaves and re-enters the pelvis around this spine, but because this is not constant, anaesthesia should be located around the spine
{kind=link}
General anaesthesia
In Britain general anaesthesia is still used for some caesarean sections, about 30% of elective procedures, and 40% of emergency procedures. It is also used for manual removal of the placenta, especially when major blood loss is anticipated.
Although general anaesthesia is relatively safe, regional anaesthesia is about eight times safer as the risks of inhaling gastric contents and of airway problems are avoided. General anaesthesia in labour is therefore decreasing.
Non-pharmacological methods
Anything that helps a woman's pain is acceptable if it does no harm. Increasing numbers of women use non-drug centred methods, possibly to maintain control, a matter of great importance to some. The least formal of these methods is the removal of anxiety—through educating the woman and a trusted companion who will be present at the birth.
Relaxation and massage
Relaxation and massage are usually taught in antenatal classes. Some 90% of women find relaxation and massage to be good for pain relief. Its effectiveness depends very much on the compliance of the woman, the stage of labour at which it is used, and the availability of the partner to help.

Percentage of women using relaxation methods by distribution of numbers of labour units in Britain
{kind=link}
TENS
Transcutaneous electrical nerve stimulation (TENS) is a popular method of distraction therapy. Low grade stimulatory electrical waves act on the posterior roots of the nerves supplying the uterus. TENS may postpone the need for pharmacological analgesia.
According to the National Birthday Trust's latest survey, only about 5.5% of women use TENS. A quarter of these women thought that it gave very good pain relief, but another quarter did not find it helpful. Other surveys have confirmed that it often provides only limited benefit. Machines are not usually available in NHS hospitals and have to be hired by the mother.

Transcutaneous electrical nerve stimulation equipment
{kind=link}
Warm water baths
Although the professionals may be divided about underwater births, women in labour like to use warm water baths in the first and early second stages of labour. The heat is analgesic and the buoyancy of water is relaxing. Warm water baths seem to be a good method of pain relief, although few reliable trials have been performed.
Key references
Chamberlain G, Wraight A, Steer P. Pain and its relief in labour. London: Parthenon Press, 1997
Russell R, Dundas R, Reynolds R. Long term backache after childbirth. BMJ 1996;312:1384-8.
Reynolds F. Analgesia for labour. Prescribers Journal 1998;38:26-31.
Leaflets on epidural pain relief are available from the Midwives' Information and Resource Unit, PO Box 669, Bristol BS99 5FG.
Coping with pain
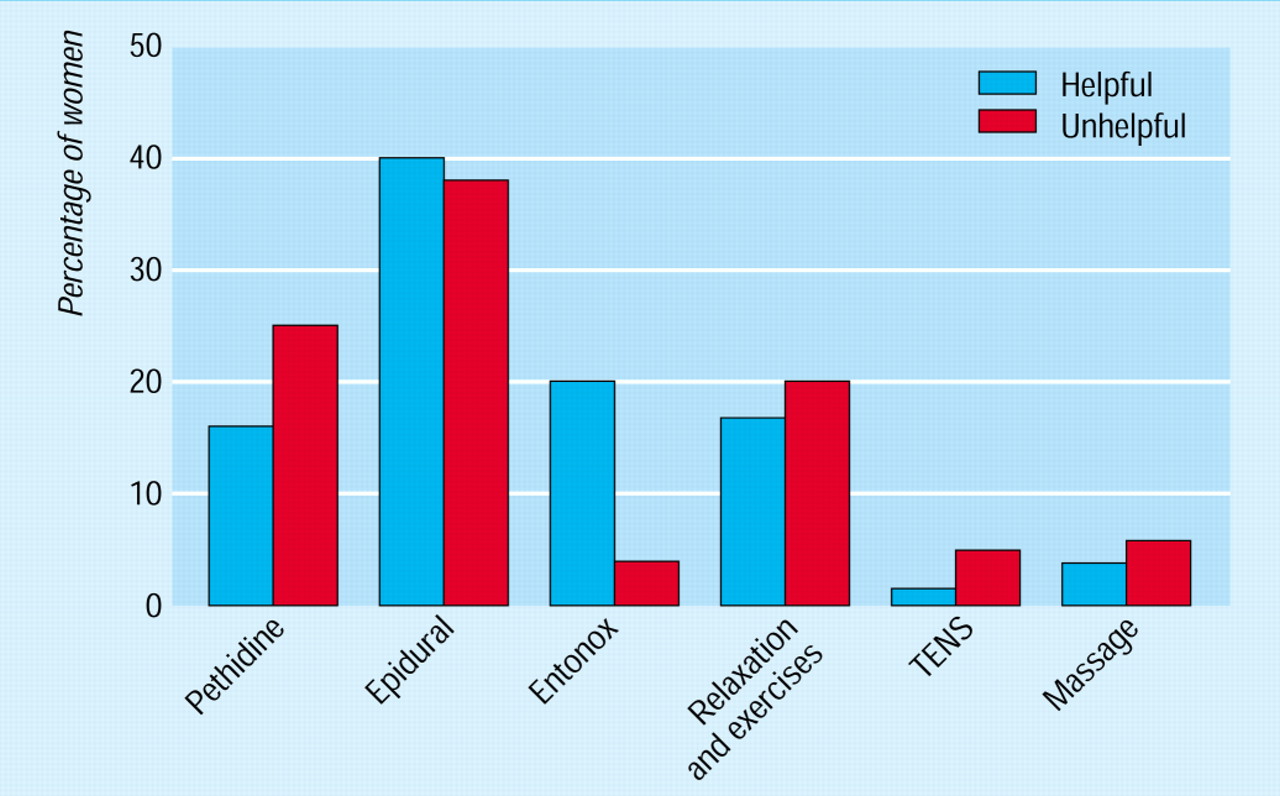
In the National Birthday Trust's survey, mothers, partners, and midwives all assessed relaxation and massage as giving good or very good pain relief in almost 90% of cases. They agreed that Entonox and epidural were good in about 90% and 97% of cases respectively, but pethidine was useful in only 58% of cases.
Suitable pain relief in labour is difficult to predict; a woman's wishes should be assessed to see if such methods are available in the unit where she plans to deliver
Ideal pain relief*
Should:
Provide good analgesia
Be safe for the mother and baby
Be predictable and constant in its effects
Be reversible if necessary
Be easy to administer
Be under the control of the mother
Should not:
Interfere with uterine contractions
Interfere with mobility
*A method that fulfils all of these criteria does not yet exist
Many women find it unhelpful to be confined to bed during labour or to have to use unwanted positions. Women usually find the presence of a companion and an individual midwife helpful in the relief of pain.
Women are often dissatisfied when they have to use a formal method of analgesia which they had initially not wished to use. This is a difficult area, which should be discussed well before labour. Women should not feel guilty about changing their mind about pain relief.

Percentage of women using various methods of pain relief and whether they found them helpful
{kind=link}
Acknowledgments
All the graphs are adapted with permission from Pain Relief in Labour, the report by the National Birthday Trust.
Footnotes
-
Inger Findley is a consultant obstetric anaesthetist at St George's Hospital, London.
The ABC of Labour Care is edited by Geoffrey Chamberlain, emeritus professor of obstetrics and gynaecology at the Singleton Hospital, Swansea. It will be published as a book in the summer.