Metastatic spinal cord compression: diagnosis and management
BMJ 2016; 353 doi: https://doi.org/10.1136/bmj.i2539 (Published 19 May 2016) Cite this as: BMJ 2016;353:i2539
Chinese translation
该文章的中文翻译

- Rasha Al-Qurainy, consultant in palliative medicine1,
- Emily Collis, consultant in palliative medicine2
- 1Pembridge Palliative Care Centre—Community Service, St Charles Centre for Health and Wellbeing, London W10 6DZ, UK
- 2Camden, Islington ELiPSe and UCLH and HCA Palliative Care Service, London NW1 2PG, UK
- Correspondence to: R Al-Qurainy rasha.al-qurainy{at}nhs.net
What you need to know
Metastatic spinal cord compression is an oncological emergency and may be the first presentation of a cancer
Magnetic resonance imaging of the whole spine is the investigation of choice
Offer corticosteroids and analgesia and consider spinal stability while the patient is assessed
Timely referral for neurosurgery or radiotherapy, or both, provides better outcomes longer term, but palliative care is the treatment of choice for some patients
Between five and 10 in every 200 patients with terminal cancer will have metastatic spinal cord compression (MSCC) within their last two years of life. It is an oncological emergency.1 2 MSCC is caused by compression of the dural sac and its contents (spinal cord or cauda equina) by an extradural or intradural mass,3 and it leads to irreversible neurological damage such as paraplegia or tetraplegia depending on the level of the lesion. Extradural masses are the more common, and their causes and presentation are the focus of this review.
Haematogenous spread with bony metastasis to the vertebral spine causes collapse and compression, accounting for over 85% of MSCC.4 5 However, local tumour extension into the spinal cord and deposition of tumour cells directly within the spinal cord from a distant tumour are two other recognised mechanisms.6 7
Early diagnosis and treatment are essential to prevent permanent neurological damage, so early recognition by non-specialists coupled with rapid referral pathways and treatment are required.
Sources and selection criteria
We carried out a search through Medline of articles published in English up to February 2016 using the terms “malignant spinal cord compression” and “metastatic spinal cord compression” and through the National Cancer Institute and Cochrane Library using the term “spinal cord compression.” We also searched the UK NICE (National Institute for Health and Care Excellence) Library for published guidance and the National Collaborating Centre for Cancer for full guidance documents. In addition to this we used personal archived references to identify peer-reviewed articles. We gave priority to randomised controlled trials, systematic reviews, meta-analyses, and prospective epidemiological studies. As appropriate we also reviewed observational, retrospective, and non-randomised studies and case reports.
Who gets MSCC?
Vertebral metastases occurs in 3–5% of all patients with cancer. As well as MSCC, they can cause pain and vertebral collapse. Most adult series highlight that cancers of the prostate, breast, and lung account for 15-20% of cases each.6 However, virtually any systemic cancer can metastasise to the spine. A recent UK hospital evaluation of current practice guidelines noted that 30% of their MSCC referrals were from cancer groups outside those most commonly associated with this complication.7
In practice, we do not know the true incidence of MSCC as most countries do not have a systematic way of recording it. However, evidence from a Scottish audit carried out in the late 1990s and from a Canadian population based study suggests that the incidence may be up to 80 cases per million people per year.8 9 UK NICE guidance has approximated this to 4000 cases each year in England and Wales.6 As cancer survival times increase, we may see a proportional rise in the incidence of MSCC as it is related to the duration of disease.
How does it present?
MSCC may be the presenting symptom of cancer. A prospective audit from the United States reported that 23% of patients presenting with MSCC were not known to have cancer.5 A more recent UK retrospective cohort study reported that 21% (27/127) of the MSCC patients presenting to a London cancer centre over a year had no pre-existing cancer diagnosis.7 MSCC can be particularly hard to diagnose in those with poor functional status, advanced age, or comorbidities.
Figure 1⇓ shows the most common sites for MSCC. However, 30-50% of patients show multi-level involvement, so whole spine imaging is imperative when MSCC is suspected.
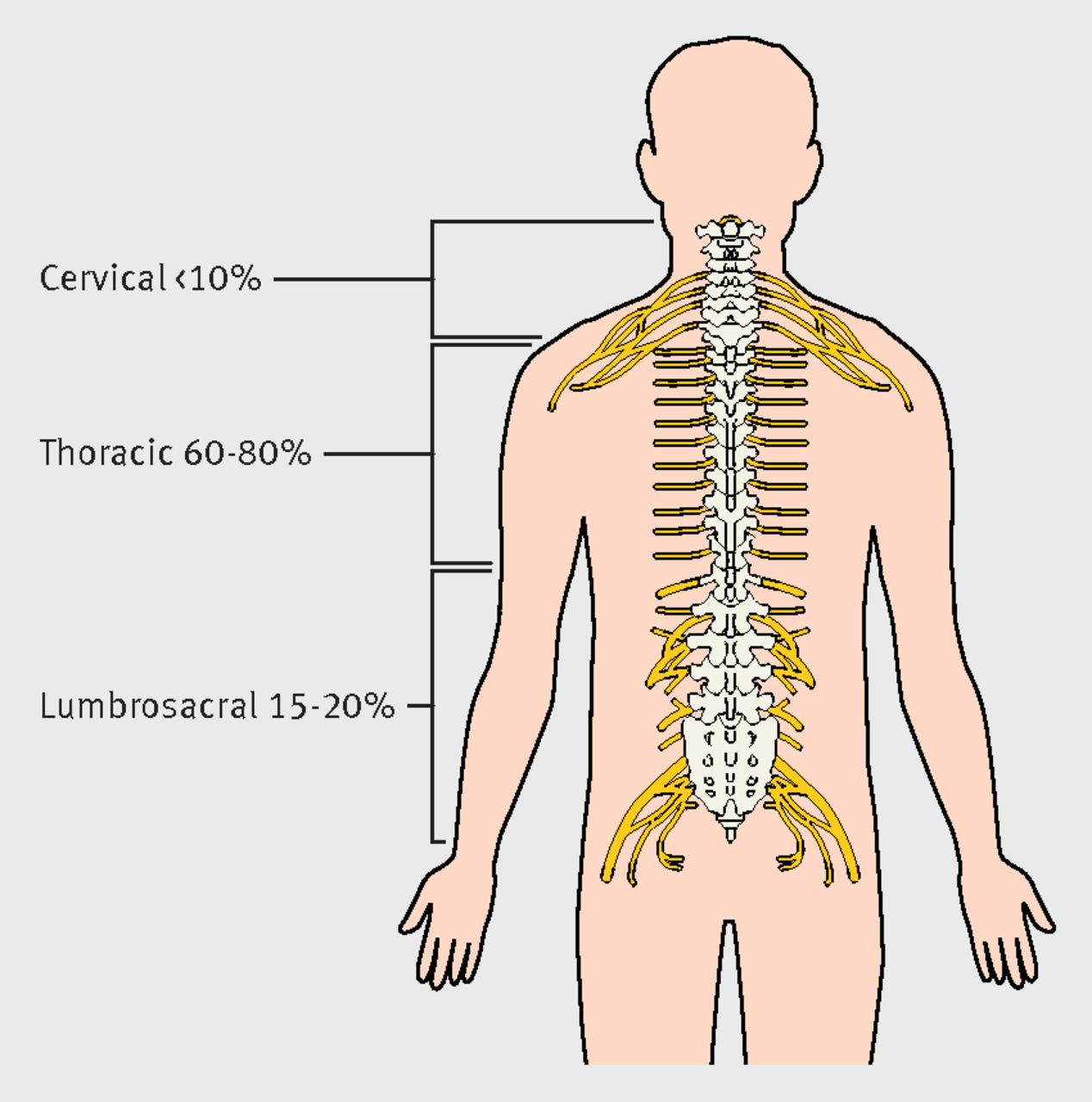
Fig 1 Distribution of sites for metastatic spinal cord compression1
{kind=link}
Pain
Back pain is the most common first symptom, occurring in 95% of patients for up to two months before signs related to MSCC appear.5 The pain can be either localised (in and around the spinal column) or radicular (nerve root pain affecting one or both sides of the body). In the Scottish audit of 319 patients with MSCC, 37% of patients had radicular pain, 15% had localised spinal pain, and 47% had both.8 Patients may report lower thoracic and upper lumbar radicular pain as abdominal pain.
Pain often increases in severity over time and may be worse on straining or coughing or on lying down due to epidural plexus distension. It is often difficult to distinguish those at risk from MSCC from those with simple back pain. UK NICE guidance recommends having a higher index of suspicion in those with a known cancer diagnosis or severe unremitting pain, especially if it is localised to the upper or middle spine or the pain is aggravated by increased intra-abdominal pressure.6
It can also be difficult to distinguish pain in those with spinal metastases from pain that has progressed to cord compression. UK NICE guidance provides a checklist (see box 1) for distinguishing between the two and recommends magnetic resonance imaging (MRI) of the whole spine within seven days for those with pain alone (in whom the suspected diagnosis is spinal metastases) compared with an MRI whole spine within 24 hours for those with pain and neurological signs, indicating possible MSCC (fig 2⇓).6
Box 1: NICE recommendations for diagnosis and management of patients at risk of or with metastatic spinal cord compression (MSCC)6
Contact the relevant team (ideally via a designated MSCC coordinator) urgently (within 24 hours) to discuss the care of patients with cancer and pain with any of the following characteristics suggestive of spinal metastases:
Pain in the middle (thoracic) or upper (cervical) spine
Progressive lower (lumbar) spinal pain
Severe unremitting lower spinal pain
Spinal pain aggravated by straining (for example, at stool) or when coughing or sneezing
Localised spinal tenderness
Nocturnal spinal pain preventing sleep.
Contact the MSCC coordinator (or equivalent) immediately to discuss the care of patients with cancer and symptoms suggestive of spinal metastases, who have any of the following neurological symptoms or signs suggestive of MSCC and view them as an oncological emergency:
Neurological symptoms (including radicular pain, any limb weakness, difficulty in walking, sensory loss, and bladder or bowel dysfunction)
Neurological signs of spinal cord or cauda equina compression
Perform frequent clinical reviews (such as daily, depending on setting) of patients with cancer who develop lower spinal pain that is clinically thought to be of non-specific origin (that is, not progressive, severe, or aggravated by straining and has no accompanying neurological symptoms). In particular, look for:
Development of progressive pain or other symptoms suggestive of spinal metastases (contact the MSCC coordinator within 24 hours)
Development of neurological symptoms or signs suggestive of MSCC (contact the MSCC coordinator immediately)
Perform frequent clinical reviews of patients without a prior diagnosis of cancer who develop suspicious spinal pain (with the characteristics outlined above) with or without neurological symptoms. Treat or refer patients with stable and mild symptoms by normal non-specific spinal pathways, or refer by cancer pathway if concerned. In particular, look for:
Development of progressive pain or other symptoms suggestive of spinal metastases (contact the MSCC coordinator within 24 hours)
Development of neurological symptoms or signs suggestive of MSCC (contact the MSCC coordinator immediately)

Fig 2 Care management pathway for metastatic spinal cord compression as outlined by the National Collaborating Centre for Cancer.6
{kind=link}
Motor deficit
Limb weakness is the second most common symptom, affecting 60-85% of patients at the time of diagnosis of MSCC.1 5 Patients may complain of an unsteady gait or a rapid onset of difficulty in walking, standing, or transferring from bed to chair that has progressed over days or a few weeks. Frail patients with advanced disease may not report the weakness, but carers may note a sudden deterioration in functional ability. Most published guidance focuses on the importance of minimising delays before starting treatment in a bid to prevent paraplegia.2 8 9 The strongest predictor of neurologic outcome with treatment is the neurologic status when treatment is initiated.10 A large, well designed German retrospective cohort study found an association between slower development of motor deficits before the start of radiotherapy and a better functional outcome after treatment.11
Sensory deficit
Sensory symptoms are less common and may predate objective sensory signs. Patients may complain of paraesthesia, decreased sensation and numbness of toes and fingers which may extend 1-5 dermatomes below the true level of cord compression. Radicular sensory loss and loss of tendon reflex on clinical examination map to the anatomical level of compression more accurately than subjective symptoms. A combination of rapid onset sensory and motor symptoms should raise a high degree of suspicion of MSCC.
Autonomic dysfunction
This is often a late consequence of MSCC and may present as bladder and bowel dysfunction such as urinary retention, urinary or faecal incontinence, or constipation.4
Direct questioning to exclude this is recommended (for example, “Are you able to open your bowels and pass urine normally?” “Have you had any accidents where your bowels have opened or you have passed urine without warning?”). Patients with advanced disease may have multifactorial constipation (such as from immobility or analgesia), which may also adversely affect bladder function. Constipation was the commonest bowel symptom in a prospective audit and occurred in 67% of all patients with MSCC.5
Cauda equina syndrome
The site of the lesion is below the first lumbar vertebra. Patients with cauda equina syndrome present differently. They often report decreased awareness at presentation on passing urine or opening bowels, without a motor deficit and sometimes in the absence of pain. The main clinical signs are decreased sensation over the buttocks, posterior-superior thighs, and perineal region in a saddle distribution, with most patients exhibiting decreased anal sphincter tone on examination. Urinary retention with overflow incontinence is an important predictor, with a sensitivity of 90% and a specificity of 95%.12
How to confirm the diagnosis
Magnetic resonance imaging (fig 3⇓) of the whole spine is the imaging method of choice and has a sensitivity of 93% and specificity of 97%.2 13 14 The implication is therefore that a few patients (7%) will have the diagnosis missed on MRI and a smaller number (3%) will have a false positive result. In the UK, NICE guidance recommends MRI is carried out within 24 hours of clinical suspicion.6 Many UK cancer centres have created a dedicated care pathway for patients referred from the community, allowing their imaging, multidisciplinary team decision making, and treatment to be conducted in a timely fashion and overseen by a named MSCC coordinator (whether or not they have a pre-established diagnosis of cancer).

Fig 3 Sagittal T2 weighted magnetic resonance image of the thoracic spine showing a tumour mass in the upper thoracic spinal canal (solid arrow) and in the prevertebral region just in front of the spine (dashed arrow). The spinal canal component is causing compression of the underlying spinal cord.
{kind=link}
Computed tomography (CT) is often used to aid surgical or radiotherapy treatment planning, but it is not recommended for definitive diagnosis of MSCC. CT myelography is now rarely used except in those with contraindications to MRI. Bone scintography and plain radiography have no role in the diagnosis.
When not to investigate or treat
In some situations where MSCC is suspected, it might be more appropriate not to investigate or treat if there is little or no prospect of a favourable outcome and the benefits and burdens have been discussed fully with the patient. Such situations include well established paralysis of more than a week’s duration, poor baseline performance status, and predicted lifespan of only days to weeks from underlying disease. In these cases, palliative care with consideration of empirical corticosteroids (oral or subcutaneous dexamethasone 8 mg twice daily) may be the preferred treatment.
What should you do while awaiting diagnosis?
Current advice is to give steroids and analgesia and to protect vulnerable spinal alignment from further damage through rest and appropriate immobilisation.
What is the role of steroids?
Evidence from randomised controlled trials suggests corticosteroids provide a beneficial adjunctive therapy in patients with myelopathy from epidural compression.15 16 One randomised study detected higher ambulation rates in patients with MSCC who received dexamethasone before radiotherapy compared with those who did not (81% v 63% at 3 months, P=0.046).17
UK guidelines recommend that, unless contraindicated, all patients with MSCC are offered an immediate loading dose of 16 mg of dexamethasone (given intravenously or orally) followed by a short course of 16 mg dexamethasone daily (given in divided doses, such as 8 mg twice daily orally).6 Steroids are contraindicated if lymphoma is the suspected cause of the MSCC as the oncolytic effect of the steroids may impair tissue diagnosis. Canadian advice recommends dexamethasone 16 mg daily as soon as MSCC is suspected and advises against using higher dose corticosteroids.14 This is in keeping with findings from a Norwegian prospective study that reported a high incidence of serious side effects and no change in ambulation with higher dose (96 mg) dexamethasone in MSCC patients.18 Anecdotal evidence suggests that patients who respond neurologically to the initiation of steroid therapy tend to respond better to radiotherapy.
Weaning steroids
Corticosteroids may provide analgesic benefit and initial improvement of neurological function.19 Long term benefit is limited, however, with no evidence of improved survival and unacceptable side effects that can be debilitating and occasionally fatal.20
After radiotherapy or surgery, UK guidelines recommend weaning steroid dose gradually and completely over 4-6 weeks, or to the lowest dose that maintains stability of symptoms. For those patients who do not proceed to surgery or radiotherapy, discussions should be undertaken about reduction in dexamethasone with a view to stopping it. In this case, a Norwegian study advises a quicker dose reduction from 16 mg to zero in 14 days.21 A large scale UK prospective audit in the hospice setting showed steroid dose was not regularly reviewed and patients often remained on steroids inappropriately, resulting in 40% experiencing side effects, most commonly proximal myopathy and peripheral oedema.20
What analgesia to prescribe?
Pain associated with MSCC usually has both bony and neuropathic elements. The mechanism of bony pain is partially through inflammatory mediators and therefore responds well to treatment with steroids. The WHO pain ladder should be used to guide analgesia, with appropriate use of neuropathic adjuvant analgesics. Seek specialist advice from the pain or palliative care team where necessary and remember to prescribe both regular analgesia plus “as needed” analgesia.
Alignment
Regardless of setting, patients with severe pain on movement suggestive of spinal instability, or any neurological symptoms or signs suggestive of MSCC, should ideally be nursed flat with neutral spine alignment (including “log rolling” with use of a slipper bed pan for toileting) until bony and neurological stability are ensured (ideally after MRI and neurosurgical review) and cautious remobilisation with physiotherapy input may begin.6
Treatment
Definitive treatment may include any combination of radiotherapy, surgery, and chemotherapy. If therapy is appropriate and the patient wants this, it should be started before any further neurological deterioration occurs and ideally within 24 hours of the confirmed diagnosis of MSCC.6
To guide treatment plans, it is important for patients to have a histological or cytological diagnosis of malignancy. If this was not established earlier in the patient’s course, needle biopsy or open biopsy should be undertaken as soon as possible and ideally before radiotherapy or surgery.1 22
When deciding on definitive treatment with the patient, consider the patient’s performance status, extent of metastatic disease, spinal stability, underlying tumour radiosensitivity, and degree of spinal cord compression.22
Radiotherapy
Historically, radiotherapy has been viewed as first line treatment because it has been shown to be as effective as a decompressive laminectomy with a lower incidence of complications.15 It also improves outcomes (including reducing local recurrence rates) after surgery and in patients who are not surgical candidates.10
There are three goals of treatment with radiotherapy:
Prevention of neurological deterioration
Improvement of neurological function
Pain relief.
For patients with a good prognosis (ambulant or with immobility for <24 hours), urgent treatment is indicated within 24 hours of diagnosis. Many radiotherapy regimens are used worldwide, with current consensus that 20 Gy in five daily fractions or 30 Gy in 10 daily fractions are acceptable regimens. The latter may reduce the risk of in-field recurrence.22
Patients with a poor prognosis include those with less than six months life expectancy, poor performance status, and established paraplegia for >24 hours. In these patients the median survival is of the order of 1-2 months with poor chance of neurological recovery. Radiotherapy is indicated only for pain relief, but in rare cases some patients may show neurological recovery. A single dose of 8 Gy is suitable.22
One randomised trial reported similar functional outcome with the three different radiotherapy schedules, but the single radiation dose was associated with higher in-field recurrence.22 23
Surgery
The goals of surgery are to achieve a circumferential decompression of the spinal cord, and to reconstruct and immediately stabilise the spinal column. A growing body of evidence indicates that surgery is superior to radiotherapy in retaining or regaining neurological function and relieving pain. A US randomised controlled trial reported 42/50 (84%) of patients randomised to neurosurgery plus postoperative radiotherapy achieved the primary endpoint of the ability to walk on completion of treatment, compared with 29/51 (57%) of those randomised to radiotherapy alone.24
The choice of surgery versus other treatments can be hard to determine. Discussions with patients should take into account their overall fitness, prognosis, and preferences.6 Surgeons increasingly base their decisions on objective scores that focus on prognosis, such as the validated Tomita and modified Tokuhashi scores.25
Patients with spinal instability, good life expectancy, or radio-resistant tumours are likely to have a much better neurological outcome with tumour resection and spinal stabilisation before radiation.10 The Spinal Instability Neoplastic Score (SINS) is a validated tool to determine clinical instability (defined as “loss of spinal integrity as a result of a neoplastic process that is associated with movement-related pain, symptomatic or progressive deformity and/or neural compromise under physiological loads”).26
A Canadian systematic review found no direct evidence to support the type of surgery best undertaken nor whether surgical salvage should be attempted if a patient is progressing on or shortly after radiotherapy. The reviewers advised consideration of pretreatment ambulatory status, comorbidities, technical surgical factors, the presence of bony compression and spinal instability, potential surgical or radiotherapy complications, and patient preferences.14
The timing of surgical intervention has also been debated. A recent small retrospective Chinese study suggests that surgery may benefit even non-ambulant patients if it is performed within 48 hours of diagnosis of MSCC.27
Chemotherapy
Chemotherapy may have a role in the management of chemo-sensitive malignancies such as lymphoma, plasma cell tumours, germ cell tumours, and small cell carcinoma of the lung.22
Rehabilitation
Discharge planning and ongoing care, including rehabilitation, starts at admission and is ideally led by a named individual within the clinical team. Successful planning involves the patient and his or her carers, oncology team, rehabilitation team, and community support, including primary care and specialist palliative care, as required. The aim is to focus on patient centred goals of care, maximising physical function in the context of overall quality of life. Rehabilitation should be provided in the patient’s preferred place of care, usually started in the acute setting and then continued in the community, hospice, or specialised inpatient rehabilitation unit.
Quality of life
Little is known about the psychological impact of MSCC.14 A recent literature review using thematic analysis concluded that patients with MSCC report good quality of life and low levels of distress in over 50% of cases, with only a minority reporting severe distress. Greater awareness of and further research into the psychological impact are required to determine those at risk and the most effective strategies for support.28
Questions for the future
Does stereotactic radiotherapy improve mobility in patients with spinal metastasis from radio-resistant tumours or patients who have received prior standard radiotherapy?
Does early surgical intervention reduce the incidence of metastatic spinal cord compression (MSCC) in those with spinal metastases?
Does vertebroplasty or kyphoplasty reduce the incidence of MSCC in those with spinal metastases?
What is the most clinically effective and cost effective regimen of radiotherapy to treat patients with established MSCC?
How patients were involved in the creation of this article
No patients were asked for input in the creation of this article.
Additional educational resources
For healthcare professionals
National Institute for Health and Care Excellence. Metastatic spinal cord compression: diagnosis and management of patients at risk of or with metastatic spinal cord compression. Full guideline. 2008. www.nice.org.uk/guidance/cg75/evidence/full-guideline-242052589
Loblaw DA, Mitera G, Ford M, Laperriere NJ. A 2011 updated systematic review and clinical practice guideline for the management of malignant extradural spinal cord compression. Int J Radiat Oncol Biol Phys 2012;84:312-7. doi:10.1016/j.ijrobp.2012.01.014
Royal College of Radiologists. Radiotherapy dose-fractionation. 2006. www.rcr.ac.uk/sites/default/files/publication/Dose-Fractionation_Final.pdf
L'Esperance S, Vincent F, Gaudreault M, et al. Treatment of metastatic spinal cord compression: CEPO review and clinical recommendations. Curr Oncol 2012;19:e478-90
For patients
National Institute for Health and Care Excellence. Metastatic spinal cord compression in adults: diagnosis and management (clinical guideline 75). Information for the public. 2008. www.nice.org.uk/guidance/cg75/ifp/chapter/About-this-information
The NICE website provides information for the public relating to its guidance. Open access. No registration required
Footnotes
Competing interests: We have read and understood BMJ policy on declaration of interests and have no relevant interests to declare.
Provenance and peer review: Commissioned; externally peer reviewed.