The hospital bed: on its way out?
BMJ 2013; 346 doi: https://doi.org/10.1136/bmj.f1563 (Published 12 March 2013) Cite this as: BMJ 2013;346:f1563
In 1967 the King Edward’s Hospital Fund for London, now known as the King’s Fund, published a new specification for the design of a “hospital bedstead.”1 This had followed an evaluation of various bed designs in collaboration with Bruce Archer, an engineering designer at London’s Royal College of Art.2 As Lawrence notes, the evaluation was intensive and “relied on extensive data collection, mathematical modelling of solutions, and field trials . . . 1000 hospitals completed a televisual survey on beds, and . . . 20 prototype beds were installed for three months at Chase Farm Hospital, Enfield. Trained observers recorded all bed-related activities from 0600 h to 2200 h daily.” The project cost £35 000—over £500 000 (€580 000; $750 000) at today’s prices.3 Over time the King’s Fund bed came to replace the many hundreds of different bed designs used in the NHS.
Coincidentally, just as the King’s Fund embarked on its bed redesign project in 1962, concern was being raised by the then minister of health, Enoch Powell, and others at the Ministry of Health about the need to save money and improve labour efficiency in the light of a shortage of nurses and general pressures on health service budgets.3
As Lawrence reports Enoch Powell at the time, a key question was “what mechanical and powered assistance would be necessary if the same quantity of care and attention had to be given with half the present quantity of woman-hours?”3 Standardising the hospital bed to improve nurse productivity and reduce procurement costs was one project on his list that, fortuitously, the King’s Fund had started to address.
Nearly half a century later, concerns about productivity remain—as does, to an extent, the King’s Fund bed, modified and redesigned. What has changed— and not just in the English NHS but in most countries—is the number of beds in use in hospitals.
In England, for example, over the 33 years since 1979, beds used for acute care fell by 35%, for maternity by 58%, for geriatric care by 65%, and for mental illness and learning disability by 74% and 96%, respectively (fig 1⇓). If allowance is made for increases in population, these bed reductions are proportionately higher—a drop of 42% in the number of acute beds per 1000 population, for example. And over the decade to 2009, the US and UK have experienced similar proportionate reductions in acute beds.
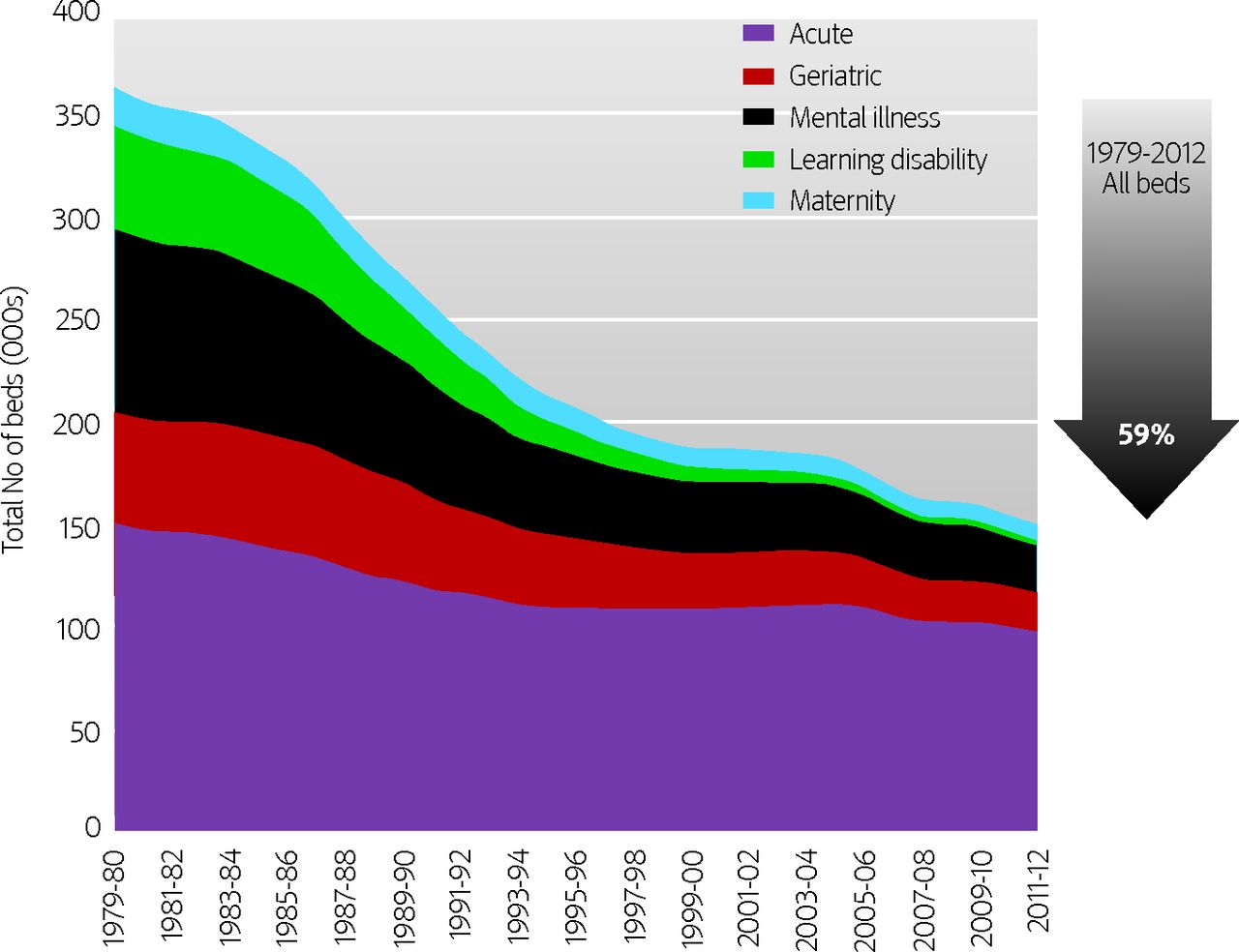
{kind=link}
The fact that the number of hospital beds has fallen in almost all countries in the Organisation for Economic Cooperation and Development (fig 2⇓) provides some clue to the reasons for these trends. Changes in medical practice have shortened the time patients spend in hospital—the average length of stay for an acute case in England has shrunk from around 9.4 days in 1979 to about three days in 2011. And new practices, drugs, and diagnostic procedures have helped shift care from the ward to the outpatient department and beyond the walls of hospitals.

Fig 2 Average annual changes in acute care beds per 1000 population (calculated from total change from 1995-2010) in selected OECD countries7
{kind=link}
The introduction of deliberate policies to move some types of care out of hospital and into the community has had a dramatic effect on hospital beds too. In England, for example, care in the community policies have changed the proportion of the hospital bed stock taken up by mental health, learning disability, and geriatric services from around 54% to 30% in just over 30 years (fig 1⇑).
With more patients being treated but fewer beds, there’s no doubt that beds are being used more efficiently. But more intensive use could be a problem. Daily bed occupancy data for England in 2011-12 reveal that average occupancy across all hospitals reached over 90% on several days (fig 3⇓). Such high occupancy rates reduce the time available for cleaning between patients and increase the chances of infection.

Fig 3 Daily bed occupancy (%) in English NHS, 2011-128
{kind=link}
Is the hospital slowly but inexorably on its way out to be replaced perhaps by “virtual wards”9 and new configurations of care facilities? Or are we already close to the limit of substitution and technology development that would allow significant further reductions?
Notes
Cite this as: BMJ 2013;346:f1563
Footnotes
Competing interests: I have read and understood the BMJ Group policy on declaration of interests and have no relevant interests to declare.
Provenance and peer review: Commissioned; externally peer reviewed.