Article Text

Abstract
Background Age-related alterations in the clinical characteristics and performance of severity scoring systems for community-acquired pneumonia (CAP) are unknown.
Methods Consecutive patients with CAP presenting to the emergency department were prospectively studied. Patients were classified as younger adults (age 18–64 years), elderly (age 65–84 years) and very old subjects (age ≥85 years). Clinical characteristics, complications, outcomes and validity of the pneumonia severity index (PSI) and CURB-65 categories were compared across these three age categories.
Results Analysis involved 348 (35.3%) younger adult patients, 438 (44.3%) elderly patients and 201 (20.0%) very old patients. Compared with younger adults, elderly and very old patients had a higher burden of comorbidities and a higher incidence of CAP-related complications. The 30-day mortality rate was 5.2% in younger adults, 7.1% in elderly patients and 9.5% in very old patients. The area under the ROC curve (AUCs) for PSI were 0.87 (95% CI 0.77 to 0.97), 0.85 (95% CI 0.803 to 0.897) and 0.69 (95% CI 0.597 to 0.787) and the AUCs for CURB-65 were 0.80 (95% CI 0.67 to 0.93), 0.73 (95% CI 0.65 to 0.82) and 0.60 (95% CI 0.47 to 0.73) in the younger adult, elderly and very old patients, respectively. A modified PSI or CURB-65 excluding the age variable increased the AUC in most age categories. There was no significant effect of age on 30-day mortality after adjusting for other PSI or CURB-65 variables.
Conclusion Elderly patients with CAP have more atypical clinical manifestations and worse outcomes. The underperformance of the PSI in elderly patients may be due to the inappropriate weight given to the age variable. A modification of the cut-off point for PSI or CURB-65 to define severe pneumonia may improve the score performance in elderly patients.
- Community-acquired pneumonia
- very old
- elderly
- pneumonia severity index
- CURB-65
- area under the ROC curve
- clinical epidemiology
- pneumonia
Statistics from Altmetric.com
- Community-acquired pneumonia
- very old
- elderly
- pneumonia severity index
- CURB-65
- area under the ROC curve
- clinical epidemiology
- pneumonia
Introduction
Community-acquired pneumonia (CAP) is a common cause of increased morbidity and mortality in older patients.1 2 Elderly patients, with many chronic diseases and diminished physiological reserve, are especially susceptible to CAP, which is often accompanied by serious complications and worse prognosis.3–5 Clinically, elderly patients with CAP often have non-specific clinical symptoms or subtle functional decline, making an accurate diagnosis and early antimicrobial treatment difficult and further worsening the prognosis.6 7
Although CAP is a major cause of mortality and morbidity in elderly patients, previous studies on signs or symptoms of CAP in elderly patients have limited sample sizes and lack age-related comparisons or details of another fast-growing age population, the very old patients (age ≥85 years).2–9 In addition, although the use of the pneumonia severity index (PSI) or CURB-65 has been widely validated and confirmed,10–18 there have been concerns of their validity in the elderly population.19–21
We have undertaken an age-related comparative analysis of a cohort of consecutive patients with CAP in a large emergency department of a university hospital. We sought to show the age-related contrasts of coexisting chronic diseases, clinical manifestations and CAP-related complications and outcomes among younger adults (age 18–64 years), elderly patients (age 65–84 years) and very old patients (age ≥85 years). We also sought to investigate how the validity of prognostic scoring systems differs across the three age groups of patients.
Methods
Study design and setting
We conducted a prospective observational study between 1 August 2008 and 28 February 2009 in the emergency department (ED) of a university hospital. The university hospital is a 2000-bed primary and tertiary care medical centre with annual visits of 60 000 medical patients.
Selection of participants and data collection
The study population consisted of adults aged ≥18 years consecutively admitted to the ED with a diagnosis of CAP. The diagnosis of CAP was based on the presence of new infiltrates on the chest x-ray together with a compatible history and/or physical findings. Compatible history is defined as having had fever (tympanic temperature >38.0°C) or hypothermia (tympanic temperature <36.0°C), cough with or without sputum production, pleuritic chest pain, dyspnoea or conscious change in the eldery patients. Compatible physical findings included tachypnoea (respiratory rate >25 breaths/min), cyanosis, strenuous respiratory pattern and changes in breathing sound such as crackles or wheezes on auscultation. Patients diagnosed with nosocomial pneumonia were not eligible for the study. Nosocomial pneumonia was defined as development of pneumonia >48 h after admission. For patients with repeated episodes of CAP during the study period, only the first episode was considered for the analysis. For all eligible patients, data on demographic characteristics, pre-existing comorbidities, initial vital signs, routine laboratory test results, admission diagnoses and variables needed to determine the PSI and CURB-65 were prospectively collected. Data on arterial blood gas analysis were only available for those with clinical signs of respiratory distress judged by primary care emergency physicians. Patients lacking arterial blood gas data were assumed to have partial pressure of arterial oxygen >60 mm Hg and arterial pH >7.35.
Definitions
Three groups of patients were defined by age as younger adults (18–64 years), elderly patients (65–84 years) and very old patients (≥85 years). Laboratory data were classified as normal or abnormal with commonly-used ranges. Organ failures assessed at ED admission and during hospitalisation were recorded based on the pre-established definitions characterised as follows: (1) acute renal failure, indicated by serum creatinine level >3.0 mg/dl (>265 μmol/l) or, in the case of pre-existing renal dysfunction, a doubling of previous serum creatinine values; (2) acute respiratory distress, indicated by pulse oxygen saturation <90% at fraction of inspired oxygen (Fio2) 21% on ED admission; (3) acute liver function impairment, indicated by serum aspartate aminotransferase level >70 IU/l or, in the case of pre-existing chronic liver disease, a doubling of previous values; and (4) shock, indicated by arterial systolic blood pressure <90 mm Hg requiring vasopressors.22–24 For parapneumonic effusions, both complicated and uncomplicated ones were included. Comorbidities were recorded according to the weighted score proposed by Charlson et al.25 The severity of the illness was quantified using the validated PSI and CURB-65. The PSI developed by Fine et al10 uses 20 clinical variables to define five severity classes; we used classes IV and V to define severe pneumonia. The CURB-65 index uses five core clinical features: new onset confusion, urea >7 mmol/l, respiratory rate 30 breaths/min, systolic blood pressure <90 mm Hg and/or diastolic blood pressure 60 mm Hg, and age 65 years.11 We defined severe pneumonia as the presence of three or more criteria. The primary outcome of interest was 30-day mortality due to any cause. The secondary outcomes of interest were hospital admission, ICU admission, mechanical ventilation and length of hospital stay.
Statistical analysis
Numerical variables were first examined by q-q plot and Shapiro–Wilk test for normality of distribution. If the variable was measured in ordinal scale or had a non-normal distribution, the non-parametric Kruskall–Wallis test or Mann–Whitney U test was used for comparison. For categorical variables, a χ2 test or Fisher exact test was used for univariate comparison. The predictive value of the PSI and CURB-65 categories in the three age groups was assessed in two dimensions of metrics, discrimination and calibration. Discrimination was determined by computing the area under the ROC curve (AUC) with 95% CI. The best cut-off value was determined by the Youden index to optimise the differentiating ability of the test with equal weight given to sensitivity and specificity. To compare the calibration, the crude number and relative frequencies of observed events in each PSI or CURB-65 risk categories were tabulated. To evaluate the influence of the age variable on the performance of the two scoring systems, we removed age from the two scoring systems and compared the AUC of the modified scores with that of the original scores containing age. To examine whether age has an independent effect on the 30-day mortality after adjusting for the remaining PSI or CURB score variables, we performed a multiple logistic regression analysis. Age was entered into the model as a categorical variable with six equally-distanced categories. Category-specific adjusted odd ratios with reference to the youngest age categories were estimated and the log-odds ratios were plotted against the age categories. A test of linear trend was also performed to examine whether there was a significant linear relationship between age and 30-day mortality. All tests were two-tailed and p values <0.05 were considered statistically significant. Data were analysed with SAS Version 9.1.3 (SAS Institute Inc) and STATA Version 10 (STATA Inc).
Results
Patient population
During the study period, 1310 episodes of CAP confirmed by x-ray were identified upon admission to the ED, of which 74 were excluded because of missing data, 162 were excluded due to a change to the final discharge diagnosis of pulmonary oedema, malignant effusion or metastatic cancer, 50 were excluded because of repeated episodes and 37 were excluded due to do-not-attempt-resuscitation order or terminal illness with palliative care. Ultimately, a total of 987 patients entered the analysis (348 younger adult patients, 294 elderly patients and 345 very old patients).
Patient characteristics and comorbidity
The characteristics of the studied patients are summarised in table 1. The mean age of the study population was 68.0±19.3 years and the male to female ratio was 0.62. The elderly and very old patients had more diabetes mellitus, stroke, dementia, chronic lung and renal disease so they had higher mean Charlson scores. Compared with the elderly or younger adult patients, the very old patients had a higher prevalence of stroke and dementia. We did not find malignancies over-represented in the elderly patients in our sample, but we did find a relatively higher proportion of patients with head and neck or oesophageal cancer in younger adults. These types of cancer are more likely to develop in younger adults and predispose them to recurrent aspiration pneumonia due to swallowing dysfunction.
Characteristics and underlying comorbidities of the studied groups
Clinical and laboratory manifestations
The clinical manifestations and laboratory results are summarised in table 2. Compared with younger adult patients, the elderly and very old patients had significantly less tachycardia and a self-reported history of fever and significantly more tachypnoea and syncope or falls. We did not find significantly more elderly or very old patients to have lower measured body temperature on ED admission. For laboratory findings, the elderly and very old patients had significantly higher prevalence of anaemia, leukocytosis and hyponatraemia than younger adult patients. The laboratory findings of the very old patients are generally comparable to the elderly patients.
Clinical and laboratory manifestations of community-acquired pneumonia among three different age groups
Complications, organ failure and outcome
CAP-related complications, organ failures and outcomes are also summarised in table 2. For complications, we did not find the elderly or very old patients to be more likely to develop empyema, parapneumonic pleural effusions, bacteraemia or adult respiratory distress syndrome. However, we found that the elderly and very old patients were more prone to develop acute gastrointestinal bleeding and organ dysfunction. A significantly higher proportion of younger adult patients also developed acute liver impairment, which is a rarely reported finding. For major outcomes, the study cohort had a 30-day all-cause mortality of 6.9%, an ICU admission probability of 14.3% and a mean length of hospital stay of 10.6±16.3 days. Although the trend of higher mortality with increasing age is significant (ptrend=0.019), the sample size is not sufficiently powered to detect the mortality difference between the three groups of patients. Other than mortality, the elderly and very old patients had a significantly higher probability of ward and ICU admissions, a higher probability of ICU admission, higher demand for mechanical ventilation and longer length of stay in hospital.
Validity of PSI and CURB-65
Table 3 shows the predictive accuracy of the PSI and CURB-65 for 30-day mortality. Both PSI and CURB-65 showed a trend of decreasing AUC in relation to higher age categories (figure 2). The best discriminative power of PSI and CURB-65 was achieved by different cut-off points in different age groups. Younger adult patients require a lower threshold value to distinguish severe from non-severe pneumonia than elderly or very old patients. On average, the PSI had high sensitivity and a high negative predictive value (NPV) while CURB-65 had low sensitivity but also a high NPV in predicting 30-day mortality. For both PSI and CURB-65, the NPV remained stable across age groups based on the recommended threshold value, while the positive predictive value (PPV) declined dramatically with advancing age categories. Table 4 summarises the crude number and proportion of non-survivors in each risk prediction category stratified by age groups.
Comparative validation of CURB-65 and pneumonia severity index (PSI) in three age groups of patients
30-day mortality by different severity classes of CURB-65 and pneumonia severity index (PSI) in three age groups of patients
Influence of age variable
As the PSI gives linear weight to the age variable, the severity scores of elderly and very old patients were indiscriminately upgraded, resulting in a low specificity in predicting 30-day mortality. To evaluate whether age was still linearly associated with the risk of 30-day mortality after adjusting for PSI and CURB variables, we performed logistic regression analysis and plotted log-OR versus 10-year age categories (figure 1). Compared with the reference population (age ≤50 years), the crude risk of 30-day mortality increased linearly with advancing 10-year age categories (ptrend=0.027, figure 1A). After adjusting for PSI or CURB variables, there were no significant residual effects of age on 30-day mortality (ptrend=0.907 for PSI, figure 1B; ptrend=0.357, figure 1C). We also performed ROC analysis for modified PSI and CURB that excluded the age variable. Compared with the original scores, the modified PSI or CURB scores had better AUC in most age categories, except the slightly decreased AUC of the modified CURB-65 score in the very old patients (figure 2A–D). Due to sample size limitation, none of these comparisons was statistically significant.
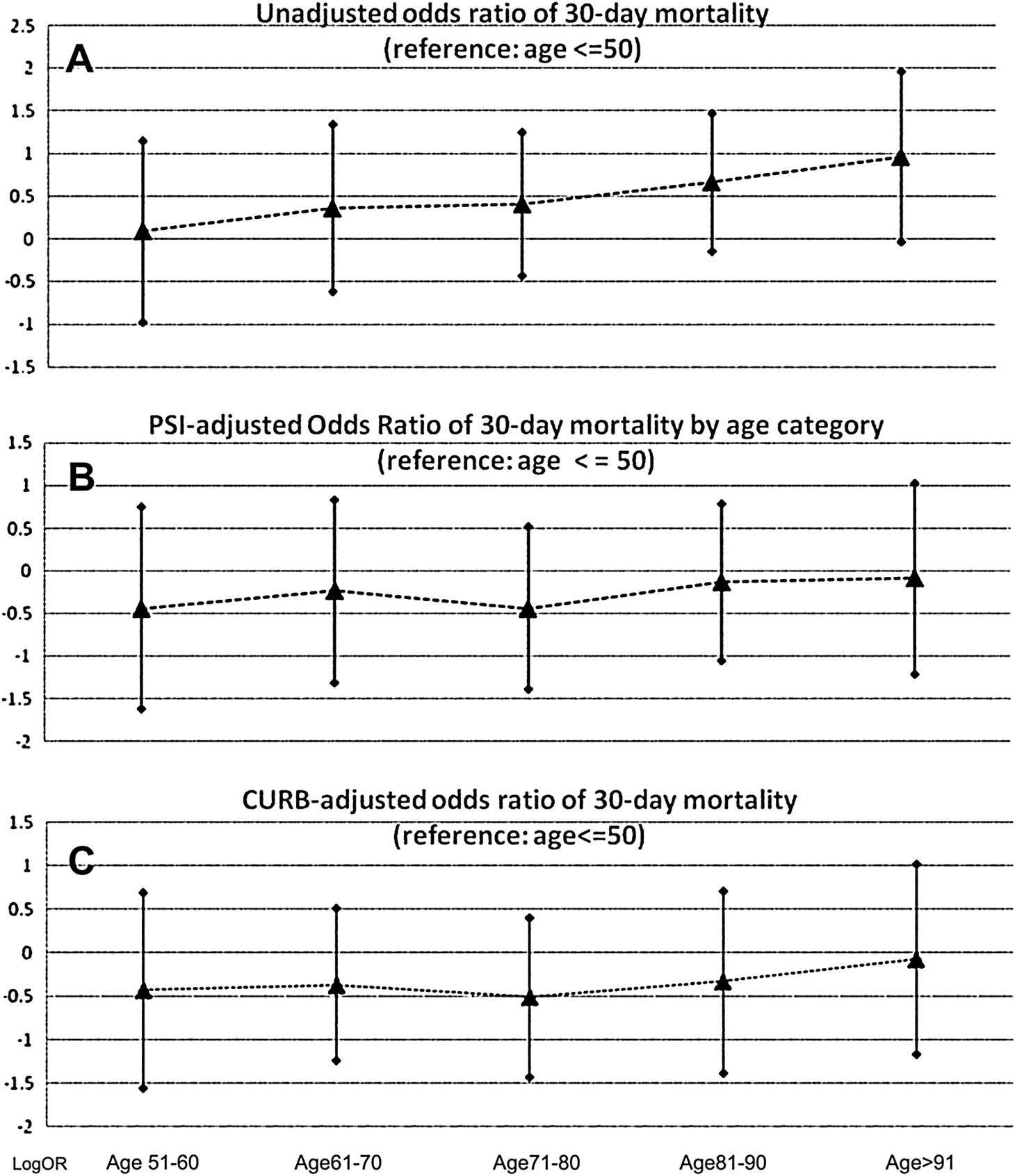
(A–C) Crude or adjusted log-odds ratio of 30-day mortality for different age groups. After adjustment with pneumonia severity index (PSI) or confusion, urea, respiratory rate, blood pressure (CURB) variables, the effect of age on 30-day mortality was not significant.

{kind=link}
{kind=link}
(A–D) ROC curves of pneumonia severity index (PSI) with/without age variable and confusion, urea, respiratory rate, blood pressure (CURB)-65/CURB for 30-day mortality in different age populations. Compared with the original scores, the modified scores generally had a larger area under the ROC curve, except the CURB score in the very old patients.
Discussion
The geriatric population (≥65 years) represents the fastest growing segment of the general population, with the very old segment (≥85 years) expanding most rapidly.26 Despite this fact, there have rarely been studies comparing the outcomes or clinical characteristics of CAP between younger adults and elderly subjects. Our study shows that elderly and very old patients have significantly different clinical presentations of CAP compared with younger adult patients. Both elderly and very old patients had a higher burden of chronic diseases, higher prevalence of anaemia, leukocytosis and hyponatraemia, were more likely to present with atypical clinical manifestations and were more prone to develop organ failure or gastrointestinal bleeding. The very old patients have an even higher propensity to develop organ failure, longer hospital stay and worse outcomes than elderly patients.3–9
It has been shown that the established scoring systems for CAP severity may not perform well in elderly patients because their atypical clinical presentations may make the cut-off values for the scoring system unreliable.19 20 Our results corroborate this finding by showing a decreasing discriminative power (measured by AUC) of PSI and CURB-65 with advancing age categories.19 20 27–29 An obvious reason for the underperformance of the PSI in elderly patients is the undue weights given to the age variable in the PSI score. As shown in figure 1, there were minimal (if any) residual effects of age on 30-day mortality after adjusting for PSI component variables other than age. Moreover, excluding the age variable from PSI or CURB-65 increased the AUC in most age categories. To improve the performance of PSI in elderly and very old patients, it is imperative to develop a non-linear weight for the age variable in PSI. Before such study is available, we suggest a modification of PSI cut-off points. As shown in our study, a higher PSI cut-off of 105 points (compared with the original 91 points) could achieve a sensitivity of 100% and a specificity of 55.7% in the elderly population, and a cut-off of 108 points could achieve a sensitivity of 90% and a specificity of 40% in the very old population.
Although ROC analysis is a popular method of evaluating score performance, judging the performance of a scoring system solely by AUC may lead to misinterpretation in real clinical settings. The AUC is not the probability that individuals are classified correctly, but mainly describes how well cases are ranked higher than non-cases for a given risk classification rule. Cook recently showed that differences between two individuals with very low risk (eg, 1.0% vs 1.1%) have the same effect on the AUC as two individuals with higher risk and a greater risk difference (eg, 5% vs 20%).30 In a hypothetical extreme situation, the AUC may remain high even if most non-survivors are misclassified to the low-risk categories as long as the non-survivors are ranked higher than survivors within those low-risk categories. The scenario is demonstrated in our study where the younger adult patient group had better AUC for CURB-65 (0.80) than the elderly (0.73) or very old patients (0.60), but 14 out of 18 (77.8%) non-survivors in the younger adult group were misclassified as low risk compared with 11 of 31 (35.4%) in the elderly group and 10 of 19 (52.6%) in the very old group. We therefore discourage the use of the traditional cut-off point of CURB-65 on the low-risk younger population despite its better AUC. Under the recommended cut-off point, the severity of the younger low-risk patients was probably underestimated.
Past efforts to improve the performance of risk prediction in the elderly population have mainly focused on the development of new scores or the modification of PSI or CURB-65 variables. Pilotto et al stated that the multidimensional prognostic index (MPI) composed of social, educational, functional and medical variables performed better than the PSI in predicting death in elderly patients with CAP.31 Naito et al showed that a modified PSI with addition of performance, anorexia and hypercapnia variables may greatly enhance the sensitivity of the original PSI at the cost of dramatically lower specificity.28 Mint et al showed that the systolic blood pressure, oxygenation, age and respiratory rate score (SOAR) was comparable but not superior to PSI or CURB-65 in elderly patients.29 We agree with these authors that some prognostic information, such as bilateral lobar infiltrates on the x-ray or underlying functional status, are not fully captured by PSI variables but we do not think the addition of one or two variables will greatly improve the performance.9 28 Again, we think the main problem of the poor performance of PSI or CURB-65 in elderly patients lies in the inappropriate weight of the age variable or the inappropriate threshold value to define severe disease.
Compared with previous studies, our study has the strengths of having a prospective design, comparison groups across different age strata, relatively large sample sizes in the elderly and very old populations and inclusion of both inpatients and outpatients. Owing to the inclusion of outpatients, the overall severity of CAP in this study cohort was reduced. The thresholds found in this study may not apply to other patient populations with very different demographic backgrounds. One of the limitations of this study is that multiple comparisons were made in the univariate analysis so we cannot exclude the possibility of false positive findings. We chose not to use the Bonferroni correction because the clinical characteristics were highly correlated and the independency assumption of the Bonferroni correction was violated.
In conclusion, we have shown that the clinical manifestations and outcomes differ in three age groups of patients with CAP. The discriminative capability of PSI or CURB-65 in predicting 30-day mortality for CAP decreased with advancing age. Using the originally recommended cut-off points for PSI or CURB-65 may underestimate the severity in the younger adult population and overestimate the severity in the elderly and very old populations. Future large prospective studies are required to determine the best weight for the age variable in the PSI score or the best age-adjusted threshold value to define severe pneumonia.
References
Footnotes
Linked articles 138131.
Funding This work is supported by grant NSC 97-2321-B-002-014 from the National Science Council of Taiwan.
Competing interests None.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of the Institutional Review Board, National Taiwan University Hospital.
Provenance and peer review Not commissioned; externally peer reviewed.