Article Text

Abstract
Objective To undertake a systematic review and meta-analysis to assess the impact of cardiac rehabilitation (CR) on physical activity (PA) levels of patients with heart disease and the methodological quality of these studies.
Methods Databases (MEDLINE, EMBASE, CENTRAL, CINAHL, PsychINFO and SportDiscus) were searched without language restriction from inception to January 2017 for randomised controlled trials (RCTs) comparing CR to usual care control in adults with heart failure (HF) or coronary heart disease (CHD) and measuring PA subjectively or objectively. The direction of PA difference between CR and control was summarised using vote counting (ie, counting the positive, negative and non-significant results) and meta-analysis.
Results Forty RCTs, (6480 patients: 5825 CHD, 655 HF) were included with 26% (38/145) PA results showing a statistically significant improvement in PA levels with CR compared with control. This pattern of results appeared consistent regardless of type of CR intervention (comprehensive vs exercise-only) or PA measurement (objective vs subjective). Meta-analysis showed PA increases in the metrics of steps/day (1423, 95% CI 757.07 to 2089.43, p<0.0001) and proportion of patients categorised as physically active (relative risk 1.55, 95% CI 1.19 to 2.02, p=0.001). The included trials were at high risk of bias, and the quality of the PA assessment and reporting was relatively poor.
Conclusion Overall, there is moderate evidence of an increase in PA with CR participation compared with control. High-quality trials are required, with robust PA measurement and data analysis methods, to assess if CR definitely leads to important improvements in PA.
- cardiac rehabilitation
- coronary artery disease
- heart failure
- meta-analysis
- systemic review
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Physical activity (PA) is defined as any bodily movement produced by skeletal muscles resulting in energy expenditure beyond resting expenditure.1 The current UK recommendation for PA in adults and older adults is ≥150 min of moderate intensity PA per week.2 This is based on a number of systematic reviews and consensus statement, consistently identifying 150 min/week as providing considerable health benefits, including reduced all-cause mortality, reduced risk factors for chronic diseases, improved cardiovascular fitness and quality of life.2 3 This is also the standard PA recommendation for patients with cardiac disease by the British Association for Cardiovascular Prevention and Rehabilitation and the Scottish Intercollegiate Guidelines Network.4 5
The benefits of cardiac rehabilitation (CR) participation for those with coronary heart disease (CHD) and heart failure (HF) are well established and include reduced cardiovascular mortality, reduced risk of hospital admissions, improved exercise capacity and health-related quality of life.6 7 A key aim of CR is to increase total daily energy expenditure in addition to exercise capacity.2 However, previous observational studies demonstrated that many patients with heart disease (pre-CR and post-CR) are failing to meet recommended daily PA levels8 9 and the extent that CR impacts on PA levels of patients remains unclear.
While two systematic reviews to date have indicated inadequate evidence of an impact of CR participation on PA levels of patients with CHD,10 11 these studies have limitations. Neither included studies involving patients with HF nor attempted meta-analysis due to the heterogeneity of CR interventions. Therefore, an updated systematic review with an improved search strategy and broader population inclusion criteria is justified.
The aim of this systematic review and meta-analysis of randomised controlled trials (RCTs) was twofold. First, to clarify the impact of CR participation on PA levels of patients with CHD and HF. Second, to review the methodological quality of PA outcomes reported in these trials.
Methods
The protocol was registered on PROSPERO (CRD42017055137). We conducted and report this systematic review in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyse statement.12
Search strategy and inclusion criteria
Details of the search strategy and inclusion criteria are provided in the online Supplementary file 1. The full search strategy is provided in the online Supplementary file 2.
Supplementary file 1
Supplementary file 2
Data extraction and risk of bias assessment
A standardised data extraction form was used to extract study characteristics, patient characteristics, intervention and control details, PA measurement method and outcome data at all follow-up time points. Multiple publications of the same study were assessed for additional data and presented as a single RCT (see online Supplementary file 3).
Supplementary file 3
The Cochrane Collaboration’s tool for assessing risk of bias was used to assess the quality of included studies.13 Data extraction and risk of bias assessment were initially completed by a single reviewer (GD) and then checked for accuracy by one other reviewer (MH, HD or RST). Disagreement was resolved by discussion.
Data synthesis and meta-analysis
Due to the wide range of PA metrics reported across studies, we first summarised the direction of PA results using a vote counting approach13 (quantifying studies on the basis of their positive, negative or non-significant results). Given the wide range of PA measures, we decided against using standardised effect size for meta-analysis and instead conducted meta-analysis where two or more studies reported the same units of PA measurement. Meta-analysis was completed on all follow-up time points apart from one outcome measure (proportion of patients categorised as physically active) where there was sufficient data to separate into short-term (≤12 months post-CR) and long-term (>12 months post-CR) follow-up.
Given the clinical heterogeneity of the included studies, random-effects models were used to pool data. Statistical heterogeneity was assessed using the I2 statistic. Binary outcomes for each study were pooled as relative risks (RR) and continuous outcomes as mean differences (MD). Meta-analysis results were reported as means and 95% CIs. A two-tailed p value of ≤0.05 was considered statistically significant. Analyses were performed in Review Manager (RevMan V.5.3, The Cochrane Collaboration) or Stata V.14.
We explored the effect of various potential treatment effect modifiers by stratifying the vote counting results, that is, setting of CR (centre vs home based), patient group (CHD vs HF), publication date (pre-1990, representing the time of major changes in drug and device management of CHD and HF), dose of exercise intervention (dose=number of weeks of exercise training×average sessions/week×average duration of session in minutes. Dose ≥2000 units (median) vs dose <2000 units); objective versus subjective PA measures and method of PA statistical analysis. Studies lacking enough information to calculate dose were omitted from the analysis.
Results
Study selection
Figure 1 summarises the screening process resulting in 47 publications across 40 RCTs included in the review.

Preferred Reporting Items for Systematic Reviews and Meta-analyses flow chart of search process. CR, cardiac rehabilitation; PA, physical activity; RCT, randomised controlled trial.
Characteristics of included studies
The 40 RCTs, all published in English, included a total of 6480 patients with cardiac disease (5825 CHD, 655 HF). A summary of study characteristics is shown in table 1. Individual study characteristics are detailed in the online Supplementary file 4.
Supplementary file 4
Summary of study characteristics
PA measures reported
In total, 28 studies measured PA using subjective approaches, 10 studies used objective methods and two studies used a combination of both. Across all studies, 45 different PA metrics were used (median 1.5, range 1–10). Details of individual study PA measurement methods including a summary is presented in the online Supplementary file 5.
Supplementary file 5
Risk of bias assessment
Risk of bias assessments for each study are summarised in figure 2. All studies were assigned high risk in blinding of participants and personnel due to the nature of CR. The most prevalent methodological issues were non-adequate description of randomisation (25/40, 62.5%), allocation concealment (27/40, 67.5%) and blinding of PA outcome assessment (26/40, 65%). There was high risk of bias in 50% (20/40) trials for incomplete outcome data. Most trials were low risk for selective reporting (33/40, 82.5%), balanced groups at baseline (34/40, 85%) and were free of cointerventions (35/40, 87.5%).

Quality appraisal. + (green), low risk of bias; ? (yellow), unclear risk of bias; − (red), high risk of bias.40–59
Impact of CR participation on PA levels
Vote counting
A total of 145 CR versus control PA comparisons were reported across all studies (online Supplementary file 6). Overall, 26% of results showed a statistically significant improvement in PA with CR (table 2).
Supplementary file 6
Vote counting
Stratified analysis
The pattern of results was similar whether PA measurement was objective or subjective (online Supplementary file 7). The statistical methods used across the studies were varied. The majority reported a p value for between-group differences. Comparing the direction of results by statistical method showed a greater number of positive results reported when the p value for interaction time×group was used (online Supplementary file 8). As numbers were small, this is unlikely to be of significance.
Supplementary file 7
Supplementary file 8
There was a higher proportion of non-significant results (86% vs 63%) and fewer positive results (10% vs 32%) in studies including patients with HF compared with studies with CHD (online Supplementary file 9). Removing the results from studies conducted prior to 1990 or those based on exercise frequency did not affect the direction of results (online Supplementary file 10).
Supplementary file 9
Supplementary file 10
CR intervention
Table 3 shows an increased number of positive results with home-based CR interventions compared with centre-based interventions. Studies with a higher exercise dose also produced a slightly increased number of positive results compared with studies with a lower exercise dose (online Supplementary file 11). The pattern of results was similar when comparing studies of comprehensive CR to exercise-only CR studies (online Supplementary file 12).
Supplementary file 11
Supplementary file 12
Vote counting—comparing centre-based CR to home-based CR and combined RCTs
Meta-analyses
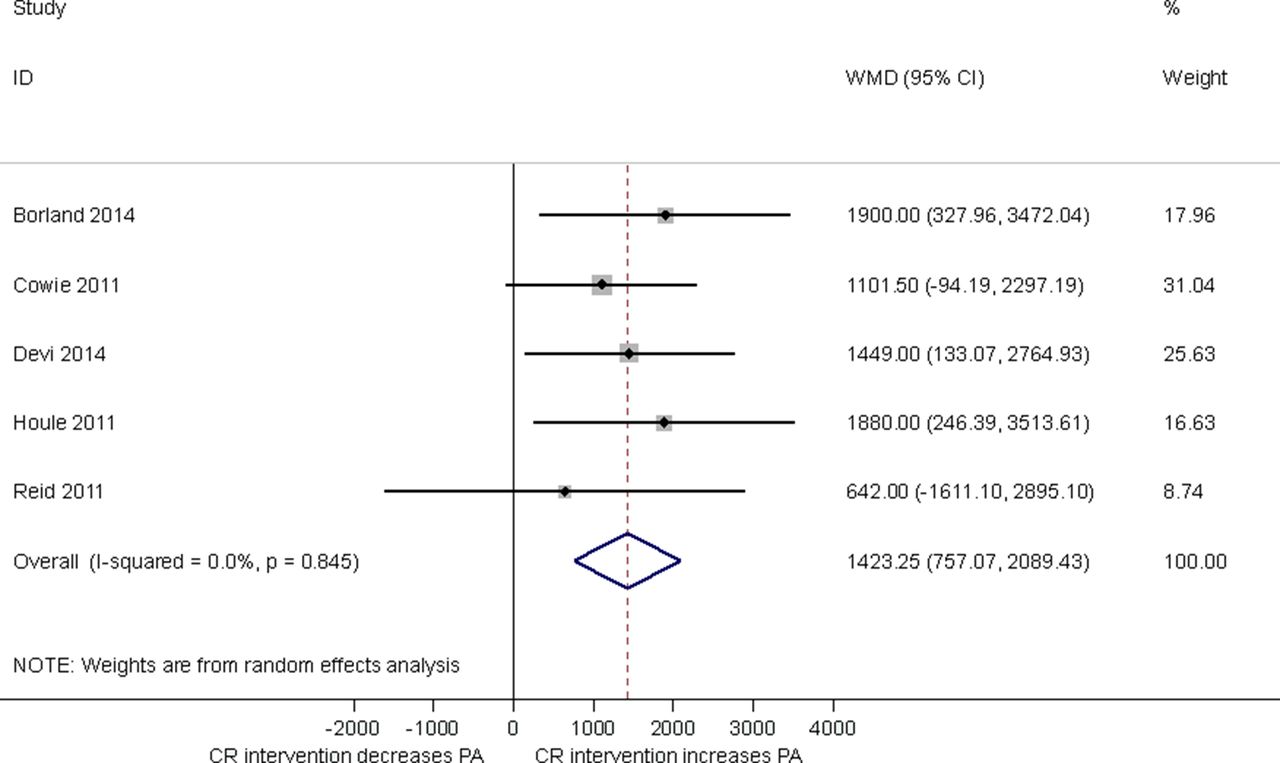
Steps/day
Five studies used mean steps/day as a measure of PA assessed by either pedometer 14–16 or accelerometer.17 18 Pooling results across studies showed compared with control, CR participation was associated with an increase in mean steps/day (1423, 95% CI 757.07 to 2089.43, p<0.0001; figure 3) at short-term follow-up (median 3, range 1.5–12 months). With no evidence of statistical heterogeneity (I2=0%, p=0.845).

Impact of cardiac rehabilitation on mean steps/day at short-term follow-up (median 3 months, range 1.5–12 months). CR, cardiac rehabilitation, PA, physical activity; WMD, weighted mean difference.
Energy expenditure
Energy expenditure (kcal/week) was estimated via questionnaire in three studies (median follow-up time 12 months, range 32 weeks–72 months).19–21 Meta-analysis showed that CR participation was associated with an increase in energy expenditure compared with control (878.4, 95% CI 433.83 to 1323.01, p=0.0001). Test for statistical heterogeneity was significant (I2=70%, p=0.04).
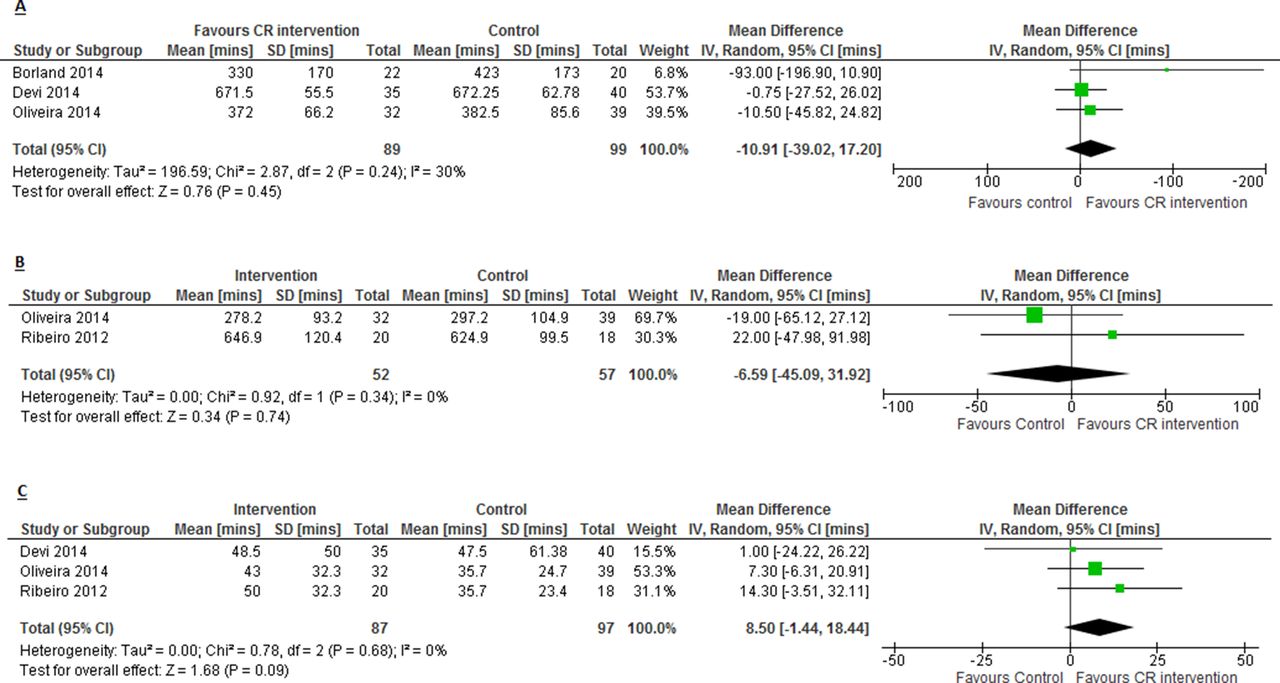
Sedentary time, light PA and moderate–vigorous PA (min/day)
There was no impact on mean min/day spent sedentary or sitting between CR and control (−10.9, 95% CI −39.02 to 17.20, p=0.45; figure 4A) based on two studies estimating this objectively via accelerometer14 18 and subjectively via International Physical Activity Questionnaire (IPAQ),22 at 9 weeks follow-up (median, range 6–12 weeks). There was no evidence of a difference in mean min/day spent in light intensity PA in CR compared with control (−6.6, 95% CI −45.09 to 31.92, p=0.74; figure 4B) based on two studies reporting this outcome via accelerometer23 and IPAQ,22 at 9.5 weeks follow-up (median, range 9–10 weeks). There was no difference in mean min/day spent in moderate–vigorous PA in CR compared with control (8.5, 95% CI −1.44 to 18.44, p=0.09; figure 4C), measured via accelerometer18 23 and IPAQ,22 at 9 weeks follow-up (median, range 6–10 weeks).

Impact of cardiac rehabilitation on (A) min/day spent sedentary or sitting; (B) min/day spent in light intensity PA and (C) min/day spent in moderate–vigorous PA. CR, cardiac rehabilitation.
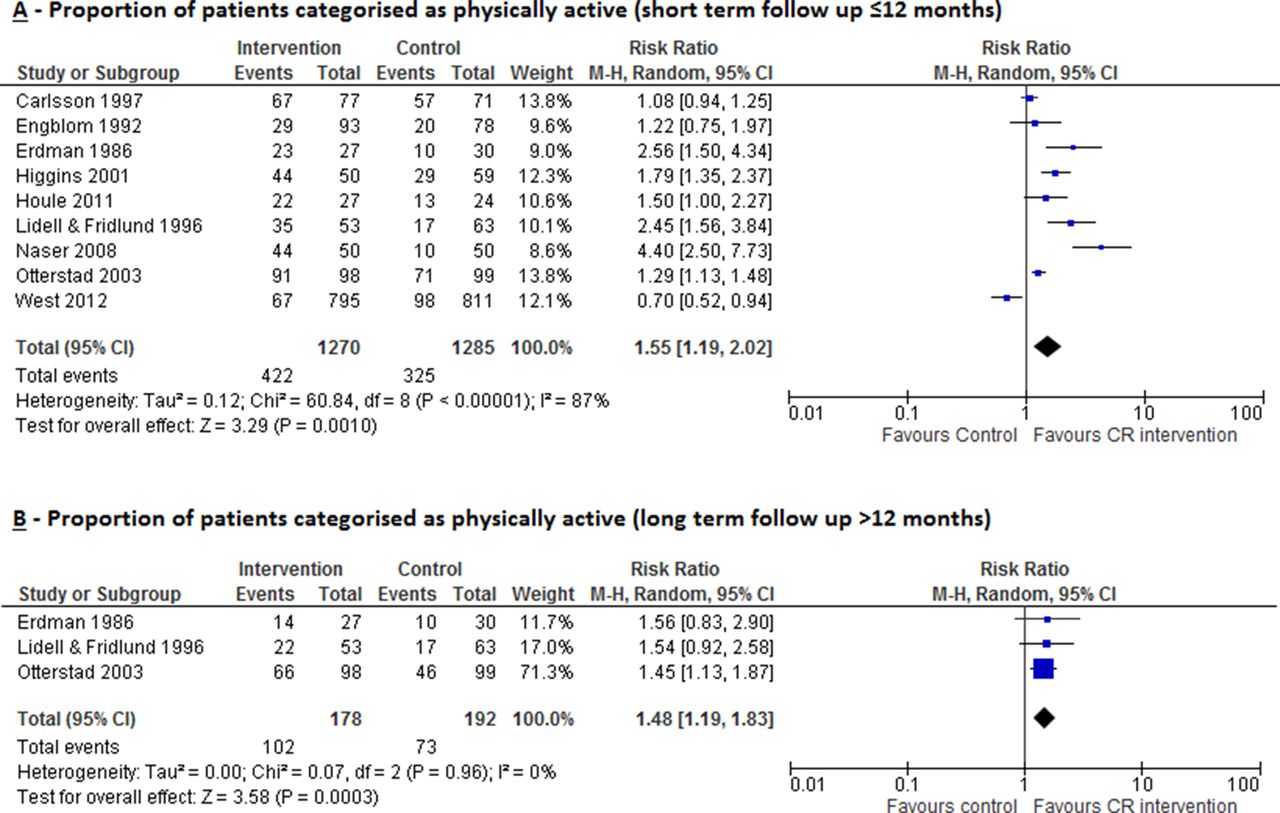
Proportion of patients categorised as physically active (short-term follow-up ≤12 months)
CR increased the proportion of patients categorised as ‘physically active’, measured at short-term follow-up (median 6 months, range 0–12 months) across nine studies (RR 1.55, 95% CI 1.19 to 2.02, p=0.001; figure 5A). There was evidence of substantial statistical heterogeneity (I2=87%, p<0.00001). The definition of ‘physically active’ varied across studies: that is, exercise frequency ≥3×/week,24 exercising ≥3×/week for 20 min,25 26 exercising >100 kcal/day,27 average daily steps >7500,15 exercising for >1 hour/week,28 regularly training (defined as either walking or cycling ≥30 min daily, sport activities once weekly or vigorous physical training)29 and two studies did not provide any definition.30 31

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Impact of cardiac rehabilitation on proportion of patients categorised as physically active measured at (A) short-term follow-up (≤12 months) and (B) long-term follow-up (>12 months). CR, cardiac rehabilitation.
Proportion of patients categorised as physically active(long-term follow-up >12 months)
CR increased the proportion of patients considered physically active, measured at long-term follow-up (median 5 years, range 2–5 years) in three studies28 30 31 (RR 1.48, 95% CI 1.19 to 1.83, p=0.0003; figure 5B) with no evidence of statistical heterogeneity (I2=0.0%, p=0.96).
Proportion of patients categorised as sedentary or not physically active
Five studies reported the proportion of patients considered sedentary,29 exercising <4 hours per week32 or undertaking no exercise,24 28 33 at 12 months (median, range 12–24 months) follow-up. There was a reduction in CR participants categorised as sedentary or not physically active(RR 0.76, 95% CI 0.61 to 0.95, p=0.02), with no evidence of statistical heterogeneity (I2=36%, p=0.18).
Discussion
This systematic review of RCTs shows moderate evidence of an increase in PA with CR participation with 26% (38/145) of comparisons reporting a statistically significant result in favour of CR compared with control. This pattern of results appear consistent regardless of whether studies assessed PA using subjective or objective methods, or the CR intervention was comprehensive or exercise only. Studies involving patients with HF appeared less likely to have positive results in favour of CR. There was an increased proportion of positive results with higher doses of CR suggesting that higher doses of exercise training may be more effective in improving PA levels. Similarly, results suggest that home-based interventions may be more effective in improving PA levels.
Meta-analyses showed that CR participation compared with control is associated with an increase in some PA outcomes: steps/day at short-term follow-up, energy expenditure (kcal/week) at short-term follow-up, proportion of patients categorised as physically active both at short-term and long-term follow-up and reduced proportion of patients categorised sedentary or not physically active at short-term follow-up. CR was not shown to have a significant impact on minutes/day spent sedentary or in light or moderate-vigorous PA at short-term follow-up.
It remains uncertain if the mean increase of 1423 steps/day that we observed with CR is clinically meaningful. In patients with chronic obstructive pulmonary disease undergoing rehabilitation, the minimal clinically important difference (MCID) was calculated to lie between 600 and 1100 steps/day and resulted in a reduction in hospital admissions.34 However, we know of no published MCID for patients with CHD or HF.
We believe there are two potential reasons why we saw improvements in some outcomes, but not others. First, categorising continuous PA data to PA categories (eg, sedentary, light moderate or vigorous) may have resulted in a loss of sensitivity to change. Second, some studies may have been susceptible to measurement bias as they used subjective PA measures.
Comparison of findings to previous studies
Our results build on previous systematic reviews10 11 that found some evidence to indicate that CR positively impacts on PA in patients with CHD, but little evidence in long term and recommended CR programmes place more emphasis on improving the long-term PA levels of patients.10 Ter Hoeve et al concluded that centre-based CR was not sufficient to improve and maintain PA levels and suggested home-based CR programmes may be more successful; however, literature is limited in this area.11 In accord with recent Cochrane systematic reviews of CR,9 10 the participating patients were relatively young (<60 years), predominantly male, with large differences in the programme location, duration, intensity, modality and length of follow-up.
Strengths and limitations
We believe this to be the first meta-analysis to assess the impact of CR on PA levels of patients with both CHD and HF . Strengths of this review include extensive literature searches, use of RCTs and inclusion of both subjective and objective PA assessment. Compared with the previous systematic reviews, we identified an additional 23 RCTs (2432 additional patients), 10 of which specifically involved patients with HF (655 patients).
However, this review has limitations. With the wide range of PA outcomes reported across the studies, at various follow-up time points, we were limited in the extent of meta-analysis we were able to complete. That only small numbers of studies were suitable for inclusion in the meta-analysis, limits our ability to draw firm conclusions from these pooled results. Vote counting was done to give a quantitative overview of the results. However, this method has limitations: (1) large and small studies carry the same weight, (2) studies reporting multiple PA outcome results contribute more weight and (3) results from multiple outcomes within study may not be independent. Furthermore, judgements by the authors on levels of PA were not based on national recommendations, leading to uncertainty about the clinical meaningfulness of PA improvements.
Key issues raised in risk of bias assessments were insufficiently described randomisation and allocation concealment procedures, leading to difficulty rating the quality of the RCTs. Additionally, 65% of studies had unclear risk of bias with regard to blinding of outcome assessment. This is particularly important in PA measurement since awareness of being assessed may cause both the intervention and control group patients to alter their behaviour and increase their PA on assessment days, potentially introducing bias to results.
There were numerous limitations in approaches studies took to assessing PA. Where questionnaires were used, few had been evidently validated for use in cardiac populations. Self-report commonly considered the frequency of exercise sessions undertaken as opposed to overall PA per se. Self-reported measures of PA are less valid and reliable than direct measures in patients with CR, generally overestimating PA and relying on patient recall.35 Despite accelerometers being the most commonly used objective PA measurement method, a variety of devices were used, with sensors placed at different body sites, and a wide range of outcome metrics reported across studies, limiting the ability to meta-analyse these data. Additionally, data handling methods were poorly reported; no studies adequately explained the minimum wear time requirement for inclusion in data analysis or data reduction techniques. Where accelerometer thresholds were used to estimate intensity, they were derived from studies in young, healthy adults which may mean the PA level is underestimated in patients with cardiac disease.36 Resting metabolic rate in patients with cardiac disease has been previously demonstrated to be significantly lower (23%–36%) than the typically utilised value of 3.5 mL/kg/min,37 which may have implications in underestimating energy expenditure during higher intensity activities. Therefore, researchers should consider using thresholds specifically established for patients with cardiac disease.
There was inconsistency in statistical methods used across the studies. Baseline adjusted regression methods are recommended for analysis of RCTs.38 However, only 35% reported a p value that took the baseline PA level into account. Although many studies showed between group differences in fitness outcomes, 26% of results demonstrated a statistically significant difference in PA outcomes. This is likely because individual studies were often small and underpowered to detect small differences in PA. Only 13 (32%) of the included studies included formal sample size calculations and of these only 4 (31%) were based on PA outcomes.
Implications for clinical practice and future research
That our results showed no difference in PA outcomes in studies that employed comprehensive CR compared with exercise-only CR suggest that improvements in PA with CR are the result of exercise training rather than components of education and psychosocial interventions. Additionally, improvement in exercise capacity may not be directly related to increases in PA levels. CR programmes should consider supplementing their existing exercise-training intervention with interventions that specifically aim to increase PA level. For example, the ongoing PATHway I trial, where the basis of the CR intervention is PA promotion and the primary outcome is objectively measured PA level.39
Further research is required to validate interventions that promote PA in cardiac populations. Furthermore, objective measurement of PA requires population-specific calibration studies to establish intensity thresholds. The use of inconsistent PA measures and units made formal pooling of data problematic. We therefore recommend that future studies use objective measures of PA such as accelerometers, be statistically powered to detect small differences in PA, use appropriate data handling and analysis methods, and PA outcomes are reported in relation to national PA recommendations. Studies should assess PA outcomes over the long term.
Conclusions
This systematic review and meta-analysis provides moderate evidence of an increase in PA with CR participation compared with control. However, the included trials were at risk of bias, and the quality of PA assessment and reporting was relatively poor. It is unclear whether increases in PA with CR are clinically meaningful. Further high-quality trials are required to assess if CR leads to important improvements in PA, such as the UK recommended target of 150 min of moderate intensity PA per week, especially in long term.
Acknowledgments
We would like to thank Catriona Organ, librarian at the Royal Cornwall Hospital Library, Knowledge Spa, Truro, and the PenCLARHC Evidence Synthesis Team at University of Exeter Medical School for their assistance throughout the process of this review. We also thank Dr Joe Mills (immediate past president of BACPR) for encouraging us to write this review and facilitating its submission.
References
Footnotes
Contributors GOD, HMD, RST and MH contributed to the conception, design, planning, conduct and reporting of the work described in this article. All authors contributed to the critical revision of the manuscript.
Funding This study was supported by a University of Exeter Postgraduate Studentship Grant.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.