Article Text

Abstract
Background Periprocedural myocardial infarction (PMI; ESC/ACC type 4a) is diagnosed on the basis of elevation of cardiac enzymes more than three times the 99th centile upper reference limit. Recent guidelines recommend the use of troponin instead of creatine kinase (CK) to diagnose PMI, but this assay increases diagnostic sensitivity, while the clinical significance of small increases in troponin remains undetermined. We examined the effects of using the new definition on the incidence of a composite endpoint (previously defined by CK) in a contemporary clinical randomised trial—the British Bifurcation Coronary Study (BBC ONE).
Methods The BBC ONE trial randomly allocated 500 patients with coronary bifurcation lesions to either a simple or complex stenting strategy. The composite primary endpoint (CPEP) included death, myocardial infarction (MI) (PMI plus subsequent MI) and target vessel failure, at 9 months.
Results In BBC ONE the CPEP occurred in 8% versus 15.2% in the simple and complex groups, respectively (HR 2.02, 95% CI 1.17 to 3.47, p=0.009). This difference was largely driven by PMI, which occurred in nine (3.6%) versus 28 (11.2%) patients (HR 3.24, 95% CI 1.53 to 6.86, p=0.001). Using troponin, PMI would have occurred in 71 (28.4%) versus 114 (45.6%) patients, respectively (HR 1.61, 95% CI 1.27 to 2.05, p=0.001), and the CPEP in 32% versus 48% of patients (HR 1.50, 95% CI 1.2 to 1.87, p=0.001). Use of troponin increased MI detection fivefold, from 7.4% to 37.0% overall.
Conclusions Use of troponin would have led to a fivefold increase in diagnosis of PMI in the BBC ONE trial. Incorporation of PMI into a composite endpoint may no longer be justified in many interventional trials.
- Acute coronary syndrome
- angina–unstable
- angiography
- angioplasty offsite
- aortic valve disease
- BBC ONE trial
- cardiac catheterisation
- cardiomyopathy dilated
- clinical trials
- congenital heart disease
- coronary syndromes
- ESC/ACC universal definition
- interventional cardiology
- ischaemic heart disease
- myocardial ischaemia and infarction (IHD)
- non-coronary intervention
- percutaneous valve therapy
- periprocedural myocardial infarction
- platelet and angioplasty
- quality of care and outcomes
- valvular disease
- valvuloplasty
Statistics from Altmetric.com
- Acute coronary syndrome
- angina–unstable
- angiography
- angioplasty offsite
- aortic valve disease
- BBC ONE trial
- cardiac catheterisation
- cardiomyopathy dilated
- clinical trials
- congenital heart disease
- coronary syndromes
- ESC/ACC universal definition
- interventional cardiology
- ischaemic heart disease
- myocardial ischaemia and infarction (IHD)
- non-coronary intervention
- percutaneous valve therapy
- periprocedural myocardial infarction
- platelet and angioplasty
- quality of care and outcomes
- valvular disease
- valvuloplasty
Introduction
Percutaneous coronary intervention (PCI) is associated with a number of potential complications. Of these, periprocedural myocardial infarction (PMI) is one of the most common,1 with a reported incidence of 5–30%.2 The cause of PMI is likely to relate to either occlusive dissection, disruption of coronary collateral blood flow, side-branch occlusion or distal embolisation.3
PMI can be diagnosed on elevation of cardiac enzyme levels with no other additional diagnostic criteria required (such as the presence of ECG changes or chest pain). It is often diagnosed in asymptomatic individuals, after an apparently uncomplicated procedure.
The clinical significance of PMI has been debated but large prospective trials have proved that higher degrees of elevation of myocardial necrosis markers after PCI are clinically relevant,4–6 so that substantially increased periprocedural creatine kinase myocardial type (CK-MB) levels (over five or eight times the upper limit of normal) have prognostic implications similar to those of a spontaneous acute myocardial infarction (MI; type 1).7 ,8
Historically, creatine kinase (CK) or CK-MB have been the cardiac biomarkers used to define PMI. However, the consensus guidelines from the European Society of Cardiology (ESC) and American College of Cardiology (ACC) released in 2000 recommended the use of the cardiac marker troponin, rather than CK-MB, and in the updated guidelines of 2007, this recommendation became absolute.9 ,10 Consequently, periprocedural myocardial necrosis (PMN) is now defined as an elevation of the troponin cardiac biomarker above the 99th centile upper reference limit (URL) of the normal population, if a normal baseline troponin value can be assumed, and a PCI-related MI (MI type 4a) or PMI is an elevation of more than three times the 99th centile URL (table 1).
Clinical classification of different types of MI, ESC/ACC guidelines, 2007
There is concern that use of a troponin-based PMI definition leads to a high incidence of PMI and a resultant increase in adverse events of unknown clinical significance. We therefore examined the effects of the ESC and ACC definition of PMI on the outcomes of a large cohort of patients from a contemporary interventional trial (the British Bifurcation Coronary Study: old, new and evolving strategies (BBC ONE)).11
Methods
The BBC ONE dataset
The BBC ONE study was a prospective randomised multicentre trial in the UK. It recruited 500 patients with coronary bifurcation lesions and randomly allocated them either to a simple strategy, n=250 (main vessel stenting with or without kissing balloon dilatation/T-stenting), or a complex strategy, n=250 (complete lesion coverage with crush or culotte stenting plus mandatory kissing balloon dilatation). Clinical follow-up of these two groups was to 9 months.
BBC ONE endpoints
The primary endpoint of the study was a composite of all-cause death, MI (PMI and subsequent MI) and target vessel failure by 9 months and the secondary endpoints were the individual components of the primary endpoint.
Definitions
In BBC ONE pre and post-procedural CK and troponin levels (troponin I/T) were collected on all patients, but only the CK data were used in the original paper.11 In the first 24 h after PCI, PMI (type 4a) was defined using biomarkers alone, specifically a CK of three or more times upper limit of normal, and for patients who already had a diagnosis of MI on their current admission, a CK rise to over 50% of the previous value, was used to confirm PMI.
Subsequent MI was defined as MI occurring over 24 h post procedure but within the 9-month follow-up period, and was diagnosed on the basis of troponin levels as per the updated ESC/ACC guidelines 2007.10
For this retrospective analysis using troponin as the biochemical marker, the same definitions were used as in the original paper.
CK and troponin biomarker data was obtained in 94% and 94% (simple strategy cases) and 93% and 90% (complex strategy cases), respectively.
Statistics
In line with the original study, normally distributed variables were presented as means±SD. The primary composite endpoint of death, MI and target vessel failure by 9 months was compared using a HR and 95% CI from a Cox regression model with treatment group as the only covariate. Treatments were compared with a log rank test and Kaplan–Meier survival curve. Analyses were done on an intention-to-treat basis using Stata V.10.1 software. A p value of less than 0.05 was considered significant.
Results
Patient demographics for the two groups in the BBC ONE trial are shown in table 2. The primary and secondary endpoints of the original study and how they would have been affected using troponin to define MI are shown in table 3.
Patient demographics
Primary and secondary endpoints
In the original study the incidence of death, MI or target vessel failure at 9 months was 8% in the simple group and 15.2% in the complex group (HR 2.02, 95% CI 1.17 to 3.47, p=0.009, figure 1). The difference between the two groups was largely driven by PMI, defined by CK. Using troponin, this significantly increased composite endpoint events in both groups, rising to 32% in the simple group and 48% in the complex group (HR 1.50, 95% CI 1.2 to 1.87, p=0.001, figure 2).
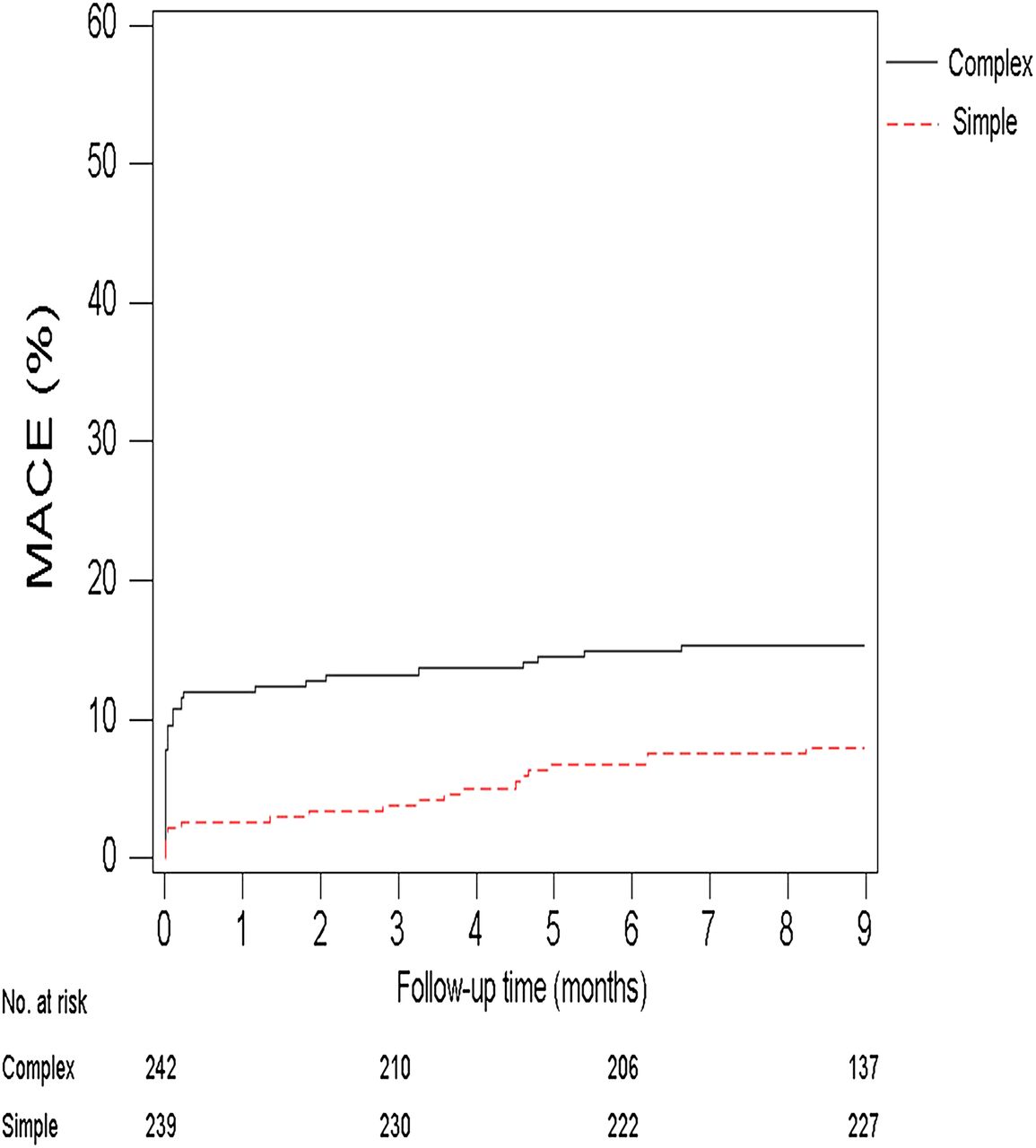
Cumulative risk of primary endpoint (creatine kinase data) MACE, major adverse cardiac event.

Cumulative risk of primary endpoint (troponin data). MACE, major adverse cardiac event.
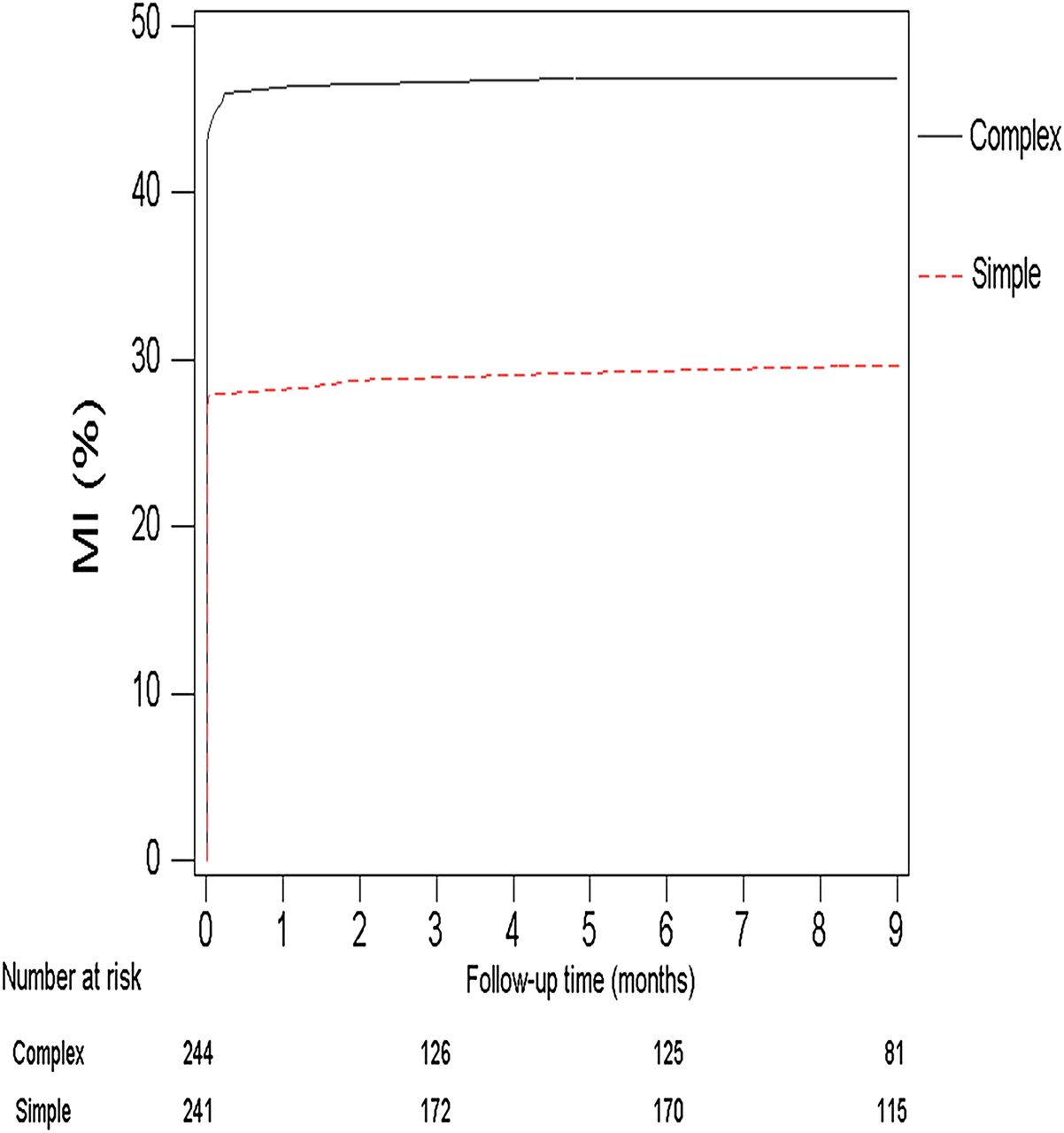
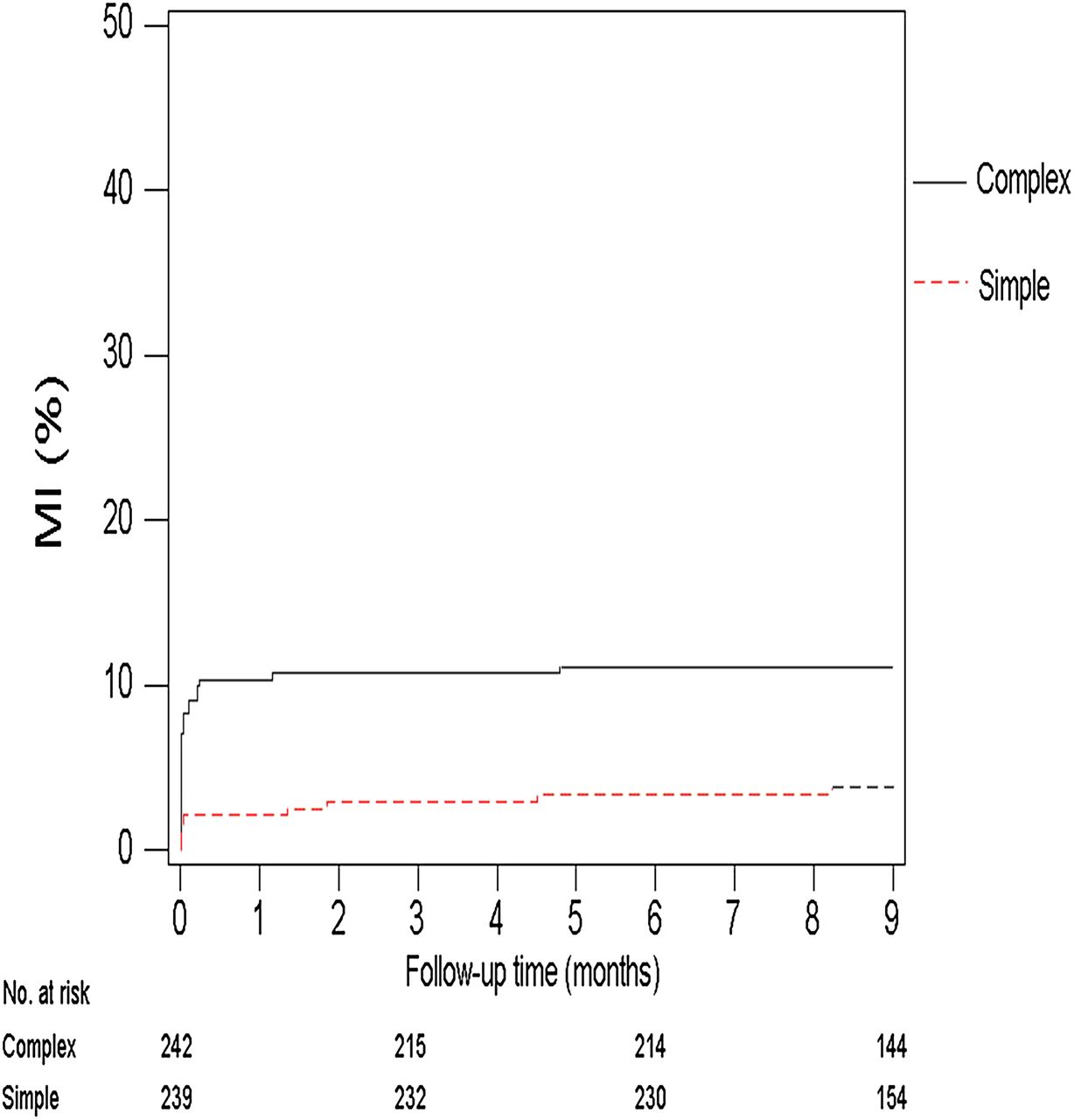
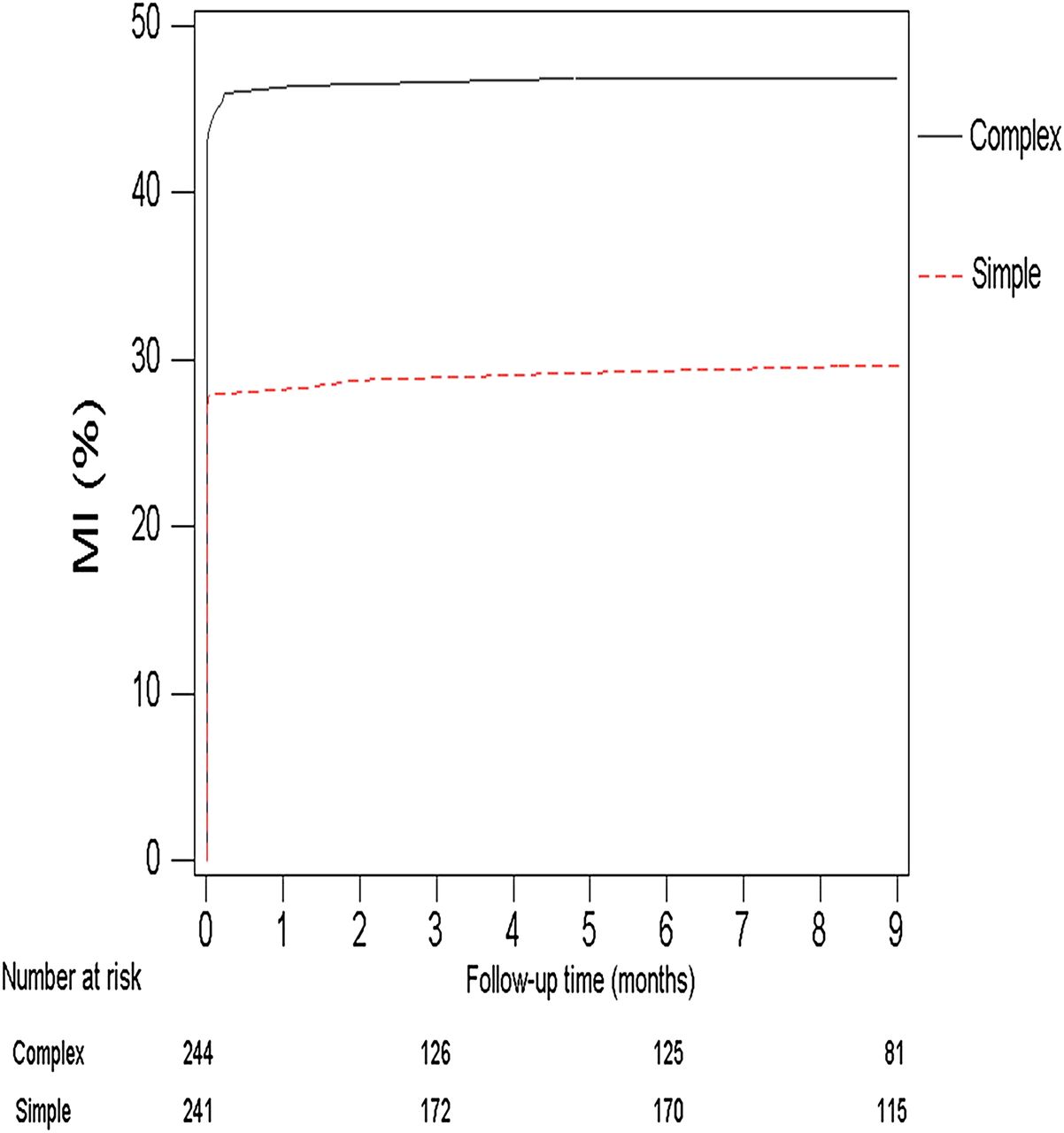
In the original study MI defined by CK occurred in nine (3.6%) patients in the simple group and 28 (11.2%) patients in the complex group (HR 3.24, 95% CI 1.53 to 6.86, p=0.001, figure 3). Again, using troponin this significantly increased MI events in both groups. MI defined by troponin occurred in 71 (28.4%) and 114 (45.6%), respectively (HR 1.61, 95% CI 1.27 to 2.05, p=0.001, figure 4).

Cumulative risk of myocardial infarction (MI) (creatine kinase data).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cumulative risk of myocardial infarction (MI) (troponin data).
The cumulative risk of the primary endpoint and MI, event-free survival and freedom from MI alone were all greater in the simple group versus the complex group, irrespective of which biomarker was used to define MI.
Discussion
From this study we see the comparative effect of using troponin rather than CK to diagnose PMI. The result is a fivefold increase in the diagnosis of PMI, and an increase in the contribution of MI to the total composite endpoint, with an associated skewed increase in total primary endpoint events.
This adds to the debate on the use of composite primary endpoints (CPEP) in interventional trials.12–14 It is wholly justified to use a composite endpoint when it is likely that the event rate of each component is going to be low, and when the assumption can be made that the relative seriousness of each individual component is broadly similar. However, in the BBC ONE trial, the CPEP was already largely driven by PMI, despite use of the less sensitive CK as the biomarker. If troponin had been used, the incidence of PMI would have dwarfed the other components of the CPEP. This would have made the trial more difficult to interpret and would also have made the use of a composite endpoint unjustified. Indeed, the new definition of MI means that there are few interventional trials now in which PMI could reasonably be incorporated into a CPEP. Moreover, the power of smaller studies utilising PMI as an endpoint would be reduced considerably, because of this increased event rate.
These concerns over impact on analysis and reporting of safety and efficacy data have led a number of investigators to consider avoiding the universal definition of PMI using troponin in favour of CK-MB.15 ,16 Indeed, the Academic Research Council have advised collecting CK-MB data whenever possible until more experience has been acquired with the evaluation of outcomes on the basis of troponin.15 It has been clearly shown that there is a dose–response relationship of progressively higher mortality for increasing levels of CK-MB related to PCI.17 There is no doubt that troponin as a biomarker has a higher sensitivity and specificity for myocardial ischaemia than CK-MB.18 However, as shown by Lim et al,19 its biggest weakness remains its inability to differentiate between PMN and true periprocedural infarction. This elegant but small study compared both CK-MB and troponin levels post complex PCI with the presence or absence of late gadolinium enhancement on cardiovascular magnetic resonance (CMR). In the CK group the patients who met the definition of a type 4a event correlated well with CMR evidence of infarction, whereas in the troponin group, while there was an increased number of events that met the definition of type 4a MI, there was very poor correlation with the presence of significant abnormality on CMR.
A recent meta-analysis including 15 studies totalling 7578 patients found elevation of troponin occurred in 28.7% of the procedures, and the incidence of PCI-related MI according to the new definition was 14.5%. However, any level of raised troponin was associated with an increased risk of major adverse cardiac events (OR 11.29, 95% CI 3.00 to 42.48, number needed to harm 5), at the time of hospitalisation and at follow-up out to 18 months (OR 1.48, 95% CI 1.12 to 1.96, number needed to harm 20), suggesting that PMN may not be a benign condition.20
Apart from its potential effects on research, the use of troponin to diagnose PMI will have practical implications. Low thresholds will increase the epidemiological incidence of MI, and will have economic, social and psychological implications for patients.
Moreover, it would be interesting to see what the effects would be if ‘high-sensitivity troponin assays’, now used in many centres, were to be adopted by the ESC and ACC to define PMI. Some studies suggest that approximately 30–50% of patients might have an elevated troponin level after elective PCI under these circumstances,21–24 and this will further complicate differentiating PMN from infarction.
If troponin is still to be used to determine PMI in interventional trials, it will probably need to be used as an isolated endpoint, rather than as part of a composite. Moreover, a recent review by Prasad and Herrmann25 cautioned against including MI as a component of CPEP in future interventional clinical trials, or using it as a surrogate for long-term outcomes, as well as a secondary efficacy or safety endpoint.
Troponin thresholds may also need to be adjusted to differentiate infarction from periprocedural necrosis. As yet, despite a level of 2.4–3.0 ng/ml being suggested as a new threshold level to define PMI using troponin,19 no studies have been performed to validate this level in larger cohorts of patients with associated outcome data.
At present there remains no established cut-off value for troponin that accurately defines PMI, and until such a value is determined (especially if the baseline troponin is elevated), then it would appear that a CK-MB level five times the URL, and /or the presence of new Q waves would appear to be the most appropriate criteria for defining PMI to date.25
Limitations
Although the troponin data were collected prospectively at the time of the indexed procedure, the precision of retrospective analysis is dependent on the availability and accuracy of the medical record. In this study cardiac biomarker data (CK or troponin) were obtained in 98% of simple and 97% of complex patients, respectively.
As the study was multicentre, different assays to measure CK and troponin were used at different sites. Consequently, therefore, we cannot exclude a degree of observer bias.
Conclusions
Biomarker assessment of PMI is important for quality, governance and research. However, troponin, using the current definition for PMI, appears highly sensitive, leading to frequent diagnosis of PMI in interventional trials, with as yet undetermined clinical significance. In the BBC ONE clinical trial, the use of troponin would have increased the PMI rate fivefold. Further studies are required to assess the troponin threshold at which clinical outcomes are affected.
References
Footnotes
See Editorial, p 1397
Competing interests Research Grant (Boston Scientific) Hildick-Smith. Advisory Board (Boston Scientific) Hildick-Smith, Thomas, Curzen, MacCarthy, Baumbach, Stables.
Provenance and peer review Not commissioned; internally peer reviewed.