Article Text

Abstract
Little literature exists on storage and preparation of an amputated limb prior to transfer to a reconstructive plastic surgical unit for possible macroreplantation. This paper describes practical measures used to prolong ischaemia time allowing macroreplantation, tissue harvesting, or fashioning of a useful stump. A simple protocol is used to summarise these points.
- macroreplantation
- tissue preservation fluid
- hypothermia
Statistics from Altmetric.com
The earliest successful major replantations of an extremity were reported by Malt and Mckhann1 and Chen et al2 in the early 1960s. Microsurgical techniques now allow routine successful replantation in plastic surgical units with numerous authors testifying the technical ability to replant and achieve viability of the limb (fig 1). However, the risks of post-ischaemic syndrome and functional recovery of the limb depends very much on the speed of revascularisation.
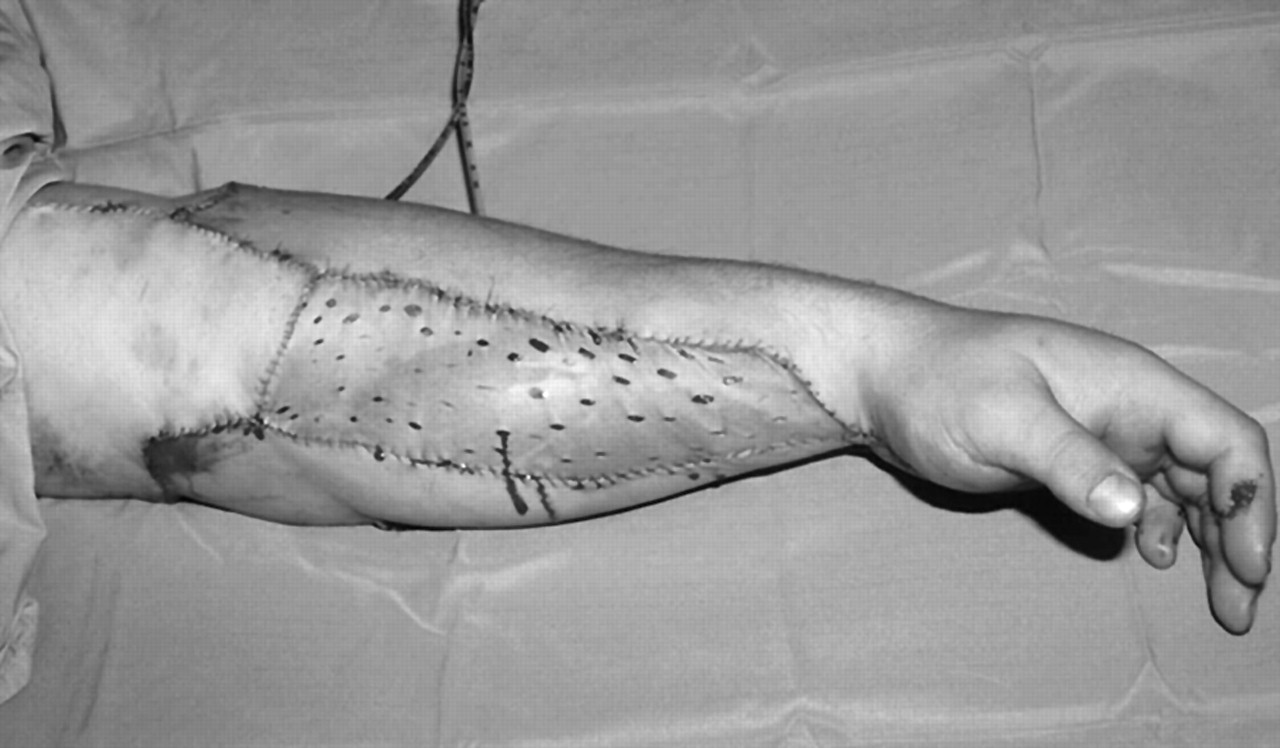
A successfully replanted upper limb.
Ischaemic contractures, muscle loss, and nerve injury affect the eventual functional status of these replanted limbs. The duration of ischaemia in the amputated tissue depends on the availability of first aid support, transportation time, distance, manpower, and preoperative preparation. Recent advances in preservation of ischaemic-sensitive solid organs such as the heart, liver, and kidney with tissue perfusion fluids have extended the time for performance of transplantation surgery.3
This article addresses how an amputated limb may be managed prior to replantation or tissue harvesting for reconstruction. We provide a simple protocol that may be placed in an accident and emergency unit.
AMPUTATED LIMB: PREOPERATIVE MANAGEMENT
The mechanism of injury leading to a completely avulsed or amputated limb is sufficiently violent to warrant strict adherence to advanced life support and trauma guidelines. The first priority is resuscitation of the patient with maintenance of the airway and ventilation with circulatory support using intravenous fluids. Life threatening injuries take precedence over limb loss. Once the patient has been stabilised and tetanus status determined, cultures should be obtained from the injured area and intravenous antibiotics covering Streptococcus, Staphylococcus aureus, and Clostridium perfringens started. Baseline haematological, biochemical studies, and four units of cross-matched blood should be requested. A meticulous history from witnesses should be obtained.4
The limb should be handled as gently as possible. Ideally only one doctor should touch the limb to avoid crushing or contamination of any tissue. The limb should be laid on a sterile towel and photographed. Photographs allow the limb to be seen by other doctors without removing it from its storage media and thus avoiding compromising tissue viability.
Any fragments of tissue, even if thought to be insignificant, should be retained since they may provide tissue for skin, bone, or nerve grafting. The amputated limb should be examined with the same meticulous care despite separation from the patient. Deformities of the limb often suggest underlying fractures of the bone (fig 2). Lacerations on the fingers, palms, or wrist may reveal divided vessels, nerves, and tendons further distally, even though the limb is amputated proximally. The skin should be palpated for foreign bodies.

Telemedicine referral of the x rays revealing an underlying fracture of the radius and ulna in the amputated limb.
The limb should then be x rayed on a sterile towel on a large x ray plate. Standard antero–posterior and lateral views should obtained. Once developed, they can be placed on a standard light box and photographed with a digital camera for telemedicine referrals.
The limb should then be wrapped in sterile gauze moistened in normal saline and placed within an insulating chest containing crushed ice and water.5,6 Ice in direct contact with the tissue will irreversibly damage cells and hinder replantation by causing frostbite damage.7,8 An attempt should be made to locate the main artery and if found tissue preservation fluid can be instilled throughout (fig 3). However, excessive dissection into the amputated stump should be avoided to prevent valuable time being lost and further compromise to any replantation procedure.

Cannulation of the brachial artery for infusion of tissue perfusion fluid.
We recommend that a tissue perfusion fluid, such as the University of Wisconsin cold storage solution (UW or Via Span, Bristol-Myers Squibb, Pharm (UK) Ltd, UK), to be kept in the fridge of the department should such a scenario arise. The most proximal artery should be found and cannulated using an 18 gauge cannula anchored by a silk suture and 1 l of UW fluid at a temperature of 10 °C and 120 cm hydrostatic pressure should be infused into the cooled limb. This should be left running continuously ensuring a complete vascular washout of the stagnant blood within the amputated vasculature.
The patient should then be referred to the nearest plastic surgical unit. Telemedicine will increasingly facilitate this process. The important details that are required are: age of the patient, the handiness, time of injury, ischaemia time, mechanism of injury (crush or guillotine), smoking, diabetes, any life or other limb threatening injuries including an accurate description of the stump and the amputated limb. In our experience we have found that cervical spine x rays are often difficult since the rotator cuff muscles on the amputated side pull the glenohumeral joint upwards obscuring the C7–T1 junction. If this is the case, we recommend that the hard collar remain in situ so that a computed tomography (CT)/magnetic resonance imaging (MRI) scan of the neck can be done at later stage. Only when the patient is haemodynamically stable with no other significant life threatening injures should transfer for definitive treatment be considered.
DISCUSSION
The potential for successful replantation is critically related to the ischaemia time. Unlike minor or distal replantations, life threatening complications may arise following macroreplantation surgery.1,4,9,10 Prolonged ischaemia time may lead to increasing biochemical and structural derangement, which will eventually be irreversible. Complex biochemical changes include loss of cellular ion homoeostasis such as Na+, K+, Ca+, and H+, and changes in oxygen metabolism. These prime the tissues for a burst of free radical production at the time of vascular reperfusion. Tissue damage incurred at the time of ischaemia is further compounded at the time of vascular reflow due to further biochemical and structural changes at reoxygenation. Irreversible ischaemic injury manifests itself as failure of re-flow in the microcirculation despite adequate arterial inflow—termed “no-reflow” phenomenon.11
Of all tissue extremities, muscle is the least tolerant of ischaemia. Hypothermia has been considered beneficial for maintenance of muscle viability before surgical replantation. The optimum level of hypothermia for minimising metabolic derangement in ischaemic muscle has been studied and found to be between 10 and 15 °C with cooling as rapidly as possible and then maintenance of the temperature at 10 °C.
A typical preservation method during transport is to wrap the amputated part in moistened gauze and immerse it within a plastic bag in crushed ice and water. However simple this may seem, it is common for potentially replantable limbs and digits to arrive at a plastic surgical unit inadequately cooled or further damaged and hence unsalvageable. Tissues may arrive macerated because they have been soaked or partially frozen as a result of direct contact with ice. Specimens have even been transported in formalin.
Evidence continues to incriminate blood products as potential mediators of ischaemia induced necrosis. Stagnant blood in the extravascular and intravascular spaces promotes ischaemic necrosis. Stagnant blood or the products of haemolysis play a major role in the development of a hyperpermeable microcirculation with subsequent interstitial oedema, elevated extrinsic hydrostatic pressure and eventual vascular compromise.6
The beneficial effects of perfusion washout can be attributed to the “benign evacuation” of stagnant blood and its haemolytic products from the microcirculation thus reducing ischaemic insult. Perfusion fluid was found to be successful in rats in normothermic conditions and when it was started as soon as amputation had occurred.6,7
University of Wisconsin cold storage solution is a cocktail of pharmacological agents with independent physiological functions. It has a pH of 7.45 with the phosphate acting as a buffer. Magnesium sulphate acts as a cell membrane stabiliser together with high molecular weight impermeable macromolecules; lactobionate and raffinose act to prevent cellular swelling. The reduced glutathione is an antioxidant and allopurinol acts as a free radical scavenger. Adenosine is used for the formation of adenosine nucleotides for cellular metabolism. The high levels of potassium ions protect the cellular structures acting on the sodium potassium pump. The UW cold storage solution is used to washout the stagnant blood from the intravascular tree and provides rapid cooling of the entire limb. The component pharmacological agents then act to preserve the tissues. UW solution also improves the quality of the tissues being preserved. Studies have also shown that serum potassium from the amputated segment when higher than 6.5 mmol/l may indicate poor outcome after replantation.8
CONCLUSION
Efficient management with the methods described above may improve the functional outcome of macroreplantation.10,11 The protocol recommended by the Queen Victoria Hospital, East Grinstead, Hampshire, UK, is shown in fig 4.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Protocol followed for preoperative management of amputated limb at the Queen Victoria Hospital, East Grinstead, Hampshire, UK.
Footnotes
-
Competing interests: none declared