Article Text

Abstract
Objectives To investigate if use of antibiotics was associated with bacterial complications following upper respiratory tract infections (URTIs).
Design Ecological time-trend analysis and a prospective cohort study.
Setting Primary, outpatient specialist and inpatient care in Stockholm County, Sweden. All analyses were based on administrative healthcare data on consultations, diagnoses and dispensed antibiotics from January 2006 to January 2016.
Main outcome measures Ecological time-trend analysis: 10-year trend analyses of the incidence of URTIs, bacterial infections/complications and respiratory antibiotic use. Prospective cohort study: Incidence of bacterial complications following URTIs in antibiotic-exposed and non-exposed patients.
Results The utilisation of respiratory tract antibiotics decreased by 22% from 2006 to 2015, but no increased trend for mastoiditis (p=0.0933), peritonsillar abscess (p=0.0544), invasive group A streptococcal disease (p=0.3991), orbital abscess (p=0.9637), extradural and subdural abscesses (p=0.4790) and pansinusitis (p=0.3971) was observed. For meningitis and acute ethmoidal sinusitis, a decrease in the numbers of infections from 2006 to 2015 was observed (p=0.0038 and p=0.0003, respectively), and for retropharyngeal and parapharyngeal abscesses, an increase was observed (p=0.0214). Bacterial complications following URTIs were uncommon in both antibiotic-exposed (less than 1.5 per 10 000 episodes) and non-exposed patients (less than 1.3 per 10 000 episodes) with the exception of peritonsillar abscess after tonsillitis (risk per 10 000 tonsillitis episodes: 32.4 and 41.1 in patients with no antibiotic treatment and patients treated with antibiotics, respectively).
Conclusions Bacterial complications following URTIs are rare, and antibiotics may lack protective effect in preventing bacterial complications. Analyses of routinely collected administrative healthcare data can provide valuable information on the number of URTIs, antibiotic use and bacterial complications to patients, prescribers and policy-makers.
- epidemiology
- epidemiology
- infection control
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
Data used in this study are population-based and include information from primary, outpatient specialist and inpatient care as well as data on all drugs dispensed in ambulatory care.
Data are continuously updated, and loss to follow-up is minimal (only when an individual moves out of the region).
Antibiotic exposure assessment is based on the information from a drug dispensation database; no data on antibiotics administered in hospitals were available for these analyses.
Outcome definitions are based on recorded diagnoses. Thus, this study relies on the accuracy and completeness of diagnoses data.
It is unknown whether the individual completed the prescribed course of antibiotic treatment.
Introduction
The use of antibiotics contributes to the emergence and spread of drug-resistant bacteria.1–3 Curbing antibiotic resistance requires coordinated action at the global, national and regional level.4 In Sweden, a comparatively low level of antibiotic utilisation has been achieved through years of strategic work at the national and regional level that have included surveillance of antibiotic utilisation5 6 and resistance trends, development and implementation of treatment guidelines as well as educational activities targeted at healthcare professionals, patients and the general public.7
Most antibiotics prescribed in the Swedish primary care are used for treatment of respiratory tract infections.8 Over the past 20 years, such use in Sweden has gradually declined.9 Most of this decline has been attributed to limiting the inappropriate antibiotic use in viral respiratory tract infections or mild self-healing bacterial infections10 by the implementation of stricter guidelines, for example, for pharyngotonsillitis and acute otitis media (AOM).11–13 However, we know that a substantial number of antibiotic prescriptions are still issued by doctors ‘just in case’ in fear of complications.14 15 There is therefore a need for large studies on rare complications of upper respiratory tract infections (URTIs) in order to quantify these risks and hopefully to reduce some of the uncertainty for primary care physicians and their patients.
The objective of this study was to investigate if use of antibiotics was associated with bacterial complications following URTIs. First, we present results from an ecological time-trend analysis assessing whether the reduction in antibiotic use in URTIs was associated with a change in the incidence of bacterial complications in a large geographically defined population. Second, we present findings from a prospective cohort study based on individual patient level data describing the incidence of bacterial complications in antibiotic-exposed and non-exposed patients with URTIs.
Methods
Setting
We conducted both an ecological time-trend analysis and a prospective cohort study in Stockholm County, Sweden, using administrative healthcare data from 1 January 2006 to 31 January 2016. Since this study used only anonymised administrative healthcare data, informed consent was not required. The study was approved by the regional ethics committee in Stockholm, Sweden (ref. no 2015/158-31).
Data sources
We used data from the regional healthcare data warehouse of Stockholm County (VAL)16 and the Swedish Prescribed Drug Register.17 VAL contains comprehensive administrative healthcare data for all Stockholm County residents (around 2.3 million people, approximately 23% of the population of Sweden). Virtually all healthcare contacts financed by the Stockholm County Council are documented in VAL. From VAL, we obtained the following information: demographic data (patient age and sex), diagnoses in primary care, outpatient specialist and inpatient care (diagnoses are coded using the International Classification of Diseases, 10th Revision (ICD-10) codes), consultation dates (for both in-person and phone consultations), hospital admission and discharge dates, as well as migration and death records. From the Swedish Prescribed Drug Register, we obtained data on dispensed antibiotics (drugs are coded using the Anatomical Therapeutic Chemical codes).
Ecological time-trend analysis
For the ecological time-trend analysis, we used aggregate level antibiotic utilisation data (exposure) and data on the incidence of bacterial complications (outcome) between 1 January 2006 and 31 December 2015. We also assessed data on the incidence of URTIs during this period. We matched the exposure and outcome data based on the year in which they were recorded. The list of antibiotics classified as those used to treat URTIs is provided in online supplement 1. The utilisation of antibiotics was expressed as the defined daily dose (DDD) per 1000 inhabitants per day (DID).18
Supplementary file 1
We studied the following bacterial complications: mastoiditis, meningitis, retropharyngeal and parapharyngeal abscesses, invasive group A streptococcal disease, acute pansinusitis, acute ethmoidal sinusitis, orbital abscess, extradural abscess and subdural abscess documented in inpatient care. For peritonsillar abscess, diagnoses recorded both in outpatient and in inpatient care were included. The lists of ICD-10 codes used to define bacterial complications and primary URTIs are provided in online supplements 2 and 3, respectively.
Prospective cohort study
Inclusion and exclusion criteria
In the prospective cohort study, we included all patients with a diagnosis of AOM, tonsillitis, sinusitis or acute URTIs of multiple and unspecified sites diagnosed in the outpatient care (primary or outpatient specialist care) from 1 January 2006 to 31 December 2015 (see online supplement 3 for ICD-10 codes used to define the cohorts). The selected population was stratified into four subcohorts to study the incidence of bacterial complications in the antibiotic-exposed and non-exposed individuals: (1) AOM cohort to study the incidence of mastoiditis and meningitis, (2) tonsillitis cohort to study the incidence of peritonsillar abscess, retropharyngeal and parapharyngeal abscesses and invasive group A streptococcal disease, (3) acute sinusitis cohort to study the incidence of acute pansinusitis, orbital abscess and extradural and subdural abscesses and (4) a combined cohort of patients with sinusitis and acute URTIs (corresponding to the ICD-10 code: J06) to study the incidence of orbital cellulitis (without formation of abscess). This last combination cohort allowed to identify complications to acute rhinosinusitis, mainly of ethmoidal origin not included in the acute sinusitis cohort (the majority of this combination cohort is composed of children). In the widespread Swedish clinical practice, children displaying symptoms and signs of an orbital complication in relation to URTI (often of viral origin) are designated as cases of acute ethmoidal sinusitis (or other types of acute sinusitis) based on the clinical findings.19 In this paper and internationally, these complications are referred to as orbital cellulitis. The cohort selection flow chart can be found in online supplement 4.
Episode definition
As more than one diagnosis of URTI can be recorded for the same patient, an episode was created to combine data on diagnoses and treatment attributed to the same URTI, and the start and the end dates were defined for each episode (figure 1).

Definition of an episode of upper respiratory tract infection (here exemplified with acute otitis media (AOM)).
The episode start date (index date) was defined as the date of the first recorded diagnosis within the episode. If there was more than a month (30-day period used in all calculations) between diagnoses, the later diagnosis was attributed to a new URTI episode. The 30-day period was based on the Swedish guidelines on URTIs (sinusitis, AOM and tonsillitis) stating that new symptoms within 30 days are a relapse and not a new episode. If a dispensation of antibiotic occurred within 3 days after the latest recorded diagnosis attributed to an episode (reflecting the strategy of watchful waiting), the date of antibiotic dispensation constituted the episode end date. If a bacterial complication occurred, the date of complication diagnosis constituted the episode end date.
If a bacterial complication occurred on the same date as the episode start date, this episode was excluded from our analyses. Furthermore, episodes with less than 1 month of follow-up were also excluded.
For all bacterial complications, if more than 6 months passed between recorded diagnoses, it was defined as an incident bacterial complication. The 6-month period was chosen in order to not miss any late bacterial complications.
Exposure groups
Patients were considered exposed to respiratory tract antibiotics if a prescription was dispensed within the episode. An episode was not considered exposed to antibiotic if the first antibiotic prescription was dispensed on the same day as the bacterial complication.
Outcomes
The follow-up of patients for study outcomes started at the episode start date and continued for a 1-month period (30 days) after the episode end date.
The study outcomes included: (1) mastoiditis and meningitis diagnosed in inpatient care (AOM cohort); (2) peritonsillar abscess diagnosed in either outpatient or inpatient care, retropharyngeal and parapharyngeal abscesses and invasive group A streptococcal disease diagnosed in inpatient care (tonsillitis cohort); (3) pansinusitis, orbital abscess and extradural and subdural abscesses diagnosed in inpatient care (sinusitis cohort) and (4) orbital cellulitis diagnosed in inpatient care (sinusitis and acute URTIs (corresponding to the ICD-10 code: J06) in combination cohort). ICD-10 codes used to define bacterial complications are provided in online supplement 2. We included as outcomes in the study those bacterial complications that have an established or plausible association with URTIs.
Statistical analyses
For the time-trend analysis, aggregate level of respiratory antibiotic utilisation data (DDD per 1000 DID), number of bacterial complications per year as well as number of primary URTI episodes per year were plotted over time.
Trends for bacterial complications and respiratory antibiotic utilisation (using DDD as the measure of utilisation) were investigated using negative binomial regression models with annual Stockholm County population counts (as of 31 December each year) as the offset variable.
For the prospective cohort study, we calculated the number of patients experiencing episodes of URTIs and stratified these patients by age and antibiotic treatment (no antibiotic treatment group and treated with antibiotics group). We then calculated the number of bacterial complications occurring in these patients and risk of bacterial complications per 10 000 episodes.
Data management and analyses were carried out using SAS 9.4 (SAS Institute, Cary, North Carolina, USA).
Results
The volumes of dispensed respiratory tract antibiotics in Stockholm County declined by 22% from 2006 to 2015 (figure 2). The number of AOM and sinusitis episodes declined, and the number of tonsillitis episodes was increasing from 2006 to 2012 and then sharply declined and remained stable from 2013 to 2015 (table 1). The proportion of patients treated with antibiotics declined in the cohorts of AOM (from 88% in 2006 to 81% in 2015), sinusitis (from 86% in 2006 to 71% in 2015) and sinusitis/acute URTI unspecified (from 36% in 2006 to 18% in 2015) and remained stable for tonsillitis (73% in 2006 and 73% in 2015).
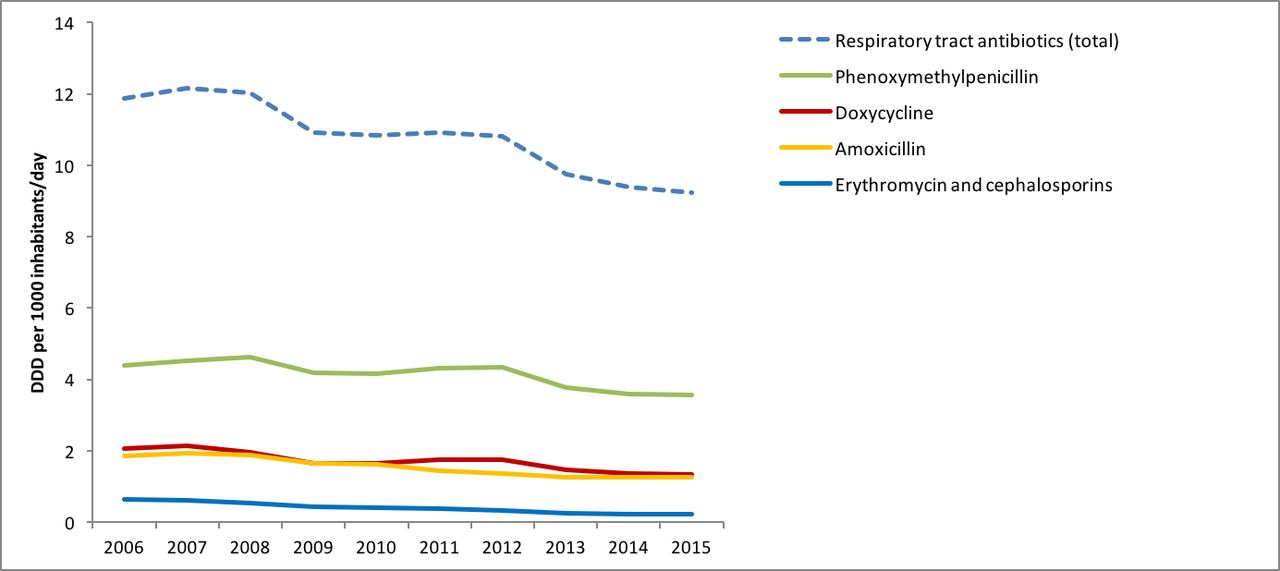
Trend for respiratory tract antibiotic utilisation in Stockholm County from 2006 to 2015. DDD, defined daily dose.
Number of episodes and antibiotic treatment for AOM (cohort 1), tonsillitis (cohort 2), sinusitis (cohort 3) and sinusitis/acute URTIs of multiple and unspecified sites in combination (cohort 4) in Stockholm County from 2006 to 2015
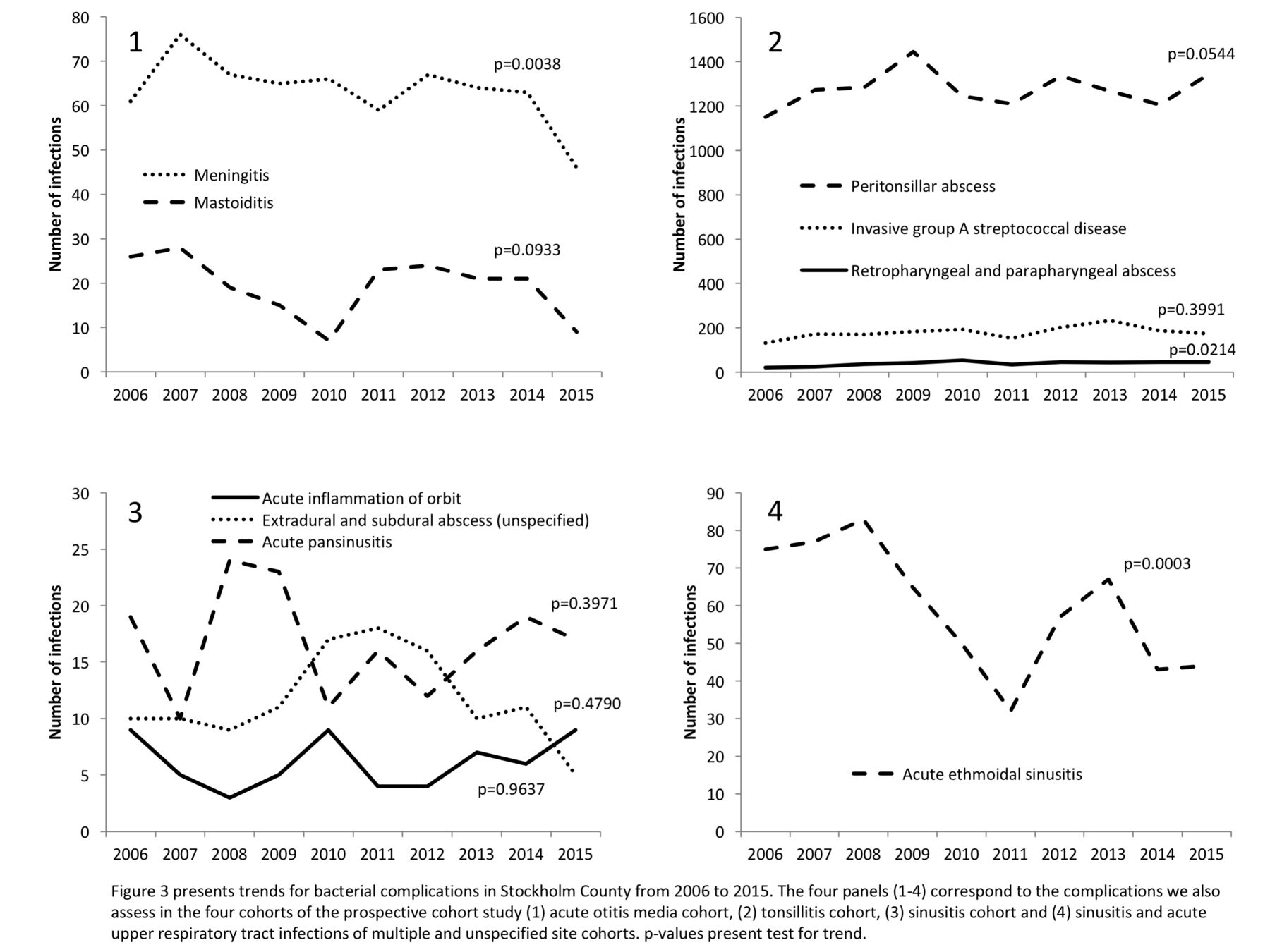
In the ecological time-trend analysis, we observed a significant decrease in the volumes of dispensed antibiotics from 2006 to 2015 (p<0.0001). During the same time period, there was no significant trend in the number of the following bacterial complications: mastoiditis (p=0.0933), peritonsillar abscess (p=0.0544), invasive group A streptococcal disease (p=0.3991), orbital abscess (p=0.9637), extradural and subdural abscesses (p=0.4790) and pansinusitis (p=0.3971). For meningitis and acute ethmoidal sinusitis, a decrease in the numbers of infections from 2006 to 2015 was observed (p=0.0038 and p=0.0003, respectively), and for retropharyngeal and parapharyngeal abscesses, an increase was observed (p=0.0214). Data are presented in figure 3.

{kind=link}
{kind=link}
{kind=link}
Trend for bacterial complications in Stockholm County from 2006 to 2015.
Using individual patient level data, we identified 515 156 AOM, 866 378 tonsillitis, 269 215 sinusitis and 2 015 595 sinusitis/acute URTIs of multiple and unspecified site episodes (see online supplement 4 for cohort selection flow charts). Table 2 provides information on the number of bacterial complications, stratified by age and antibiotic treatment. Our data showed that all bacterial complications in URTI patients were infrequent (less than 1.5 per 10 000 episodes) with the exception of peritonsillar abscess after tonsillitis (risk per 10 000 tonsillitis episodes: 32.4 and 41.1 in patients with no antibiotic treatment and patients treated with antibiotics, respectively). Peritonsillar abscess was most common in adults aged 15 to 64 years (risk per 10 000 tonsillitis episodes: : 42.2 and 67.4 in patients with no antibiotic treatment and patients treated with antibiotics, respectively).
Risk of bacterial complications in the month after diagnosis of URTIs
Discussion
The volumes of dispensed URTI antibiotics in Stockholm County decreased by 22% over a 10-year period from 2006 to 2015. Our ecological time-trend analysis covering the entire population in a large region showed that restricted use of antibiotics was not associated with an increase in bacterial complications of mastoiditis, meningitis, peritonsillar abscess, invasive group A streptococcal disease, acute pansinusitis, acute ethmoidal sinusitis, orbital abscess and extradural abscess and subdural abscess. Moreover, the number of meningitis and acute ethmoidal sinusitis complications decreased over the study period. For retropharyngeal and parapharyngeal abscesses, an increase was observed.
The analyses of individual patient level data revealed that the incidence of bacterial complications following primary URTIs was very low: the risk per 10 000 URTI episodes was less than 1.5 (average for all age groups) for all analysed bacterial complications (with the exception of peritonsillar abscess) for both patients with no antibiotic treatment and patients treated with antibiotics. We observed a slightly higher risk of bacterial complications in the antibiotic treated group in 3 out of 9 bacterial complications studied. This can possibly be explained by the presence of confounding by indication: patients prescribed antibiotics likely had a more severe primary URTI, thus were at a higher risk of both being prescribed an antibiotic and progressing to bacterial complications.
Our findings of no association between more restricted antibiotic use and the incidence of bacterial complications are in line with previous studies.10 20–22 A previous Swedish study23 showed that there was no increase in acute mastoiditis since 2000, when new guidelines recommending restrictive use of antibiotics for AOM were introduced. In 2010, new revised guidelines with an even more restrictive recommendation were issued.24 Our study includes data on mastoiditis in Stockholm County before and after these most restrictive recommendations, thus providing a first update on the impact of further restriction of antibiotic use in the treatment of AOM. Of interest also is that while the proportion of patients with tonsillitis, sinusitis and other URTI receiving antibiotics in our study was comparable with that of Norway25 the doctors in Stockholm prescribed antibiotics to a larger proportion of AOM patients than the doctors in Norway did. This may possibly be explained by different frameworks for coding AOM (ICD-10 vs International Classification of Primary Care) and different definitions for exposure to antibiotic. Our definition of the antibiotic-exposed group included patients receiving an antibiotic anytime during their URTI episode, thus likely resulting in a more complete capture of patients treated with antibiotics. Differences in definitions used can also explain discrepancies with other observational studies.20 26 For example, our definition of bacterial complication only included bacterial complications recorded in inpatient care (except for peritonsillar abscess) and, therefore, was stricter than those used in other studies (eg, in comparison to analyses by Petersen et al).
We found that a large proportion of diagnosed bacterial complications analysed in this study were not preceded by patients seeking care for URTIs. A short duration from the onset of primary URTI to progression to bacterial complication could be an explanation for this as patient would have already developed a bacterial complication by the time of the first contact with healthcare professionals. In children, for example, the onset of symptoms and signs of mastoiditis is often very quick (within 24 hours). In this case, a rapid progress of the disease is likely related to the virulence of pathogenic airway bacteria. It has also been noted that peritonsillar abscess, the most common bacterial complication among adults in our study, often occurs without a preceding typical tonsillitis.27 Alternate routes of infection, for example, oral pathogenic bacteria, may play a role in the aetiology of peritonsillar abscess.
The decline in meningitis and acute ethmoidal sinusitis observed in our analyses is in line with previous studies demonstrating a similar decrease in these infections after the introduction of conjugated antipneumococcal vaccine in the general vaccine schedule in Stockholm in 2007.28 Retropharyngeal and parapharyngeal abscesses are uncommon diseases, and it was outside of the scope of this study to investigate what may have contributed to the discreet increase in these complications observed during the study period. Among risk factors for these heterogeneous infections are local trauma, immunosuppression and dental infections.29
All data used in our study are population-based and include information on diagnoses in primary, outpatient specialist and inpatient care as long as they were recorded by healthcare professionals, as well as on all dispensations of antibiotics in ambulatory care. These data are updated on a monthly basis, thus enabling a real-time patient follow-up. We based our selection of bacterial complications on those that we perceived have an established association with URTIs. There could be other bacterial complications such as pneumonia that we have missed by narrowing the number of complications we looked for. Furthermore, using administrative data in general carries a number of known limitations, including reliance on the accuracy and completeness of recorded diagnoses, lack of information on antibiotics administered in hospitals and inability to assert whether the patient completed the prescribed course of antibiotic treatment.
To summarise, our study demonstrated that routinely collected administrative healthcare data can provide valuable information on the number of URTIs, antibiotic use and bacterial complications to patients, prescribers and policy-makers. We found that bacterial complications were rare both in patients with no antibiotic treatment and in patients treated with antibiotics. While the utilisation of respiratory tract antibiotics decreased, bacterial complications following URTIs remained uncommon.
Acknowledgments
Ahmed Farah at the Public Health Agency of Sweden is acknowledged for statistical support
References
Footnotes
Contributors TC, IE, AG, BW, JH, CN and AT contributed to the design of the study. TC extracted the data, wrote statistical programs and led statistical analyses. TC, IE, AG, BW, JH, CN and AT participated in the interpretation of data. TC had full access to all of the data in the study and can take responsibility for the integrity of the data and the accuracy of the data analysis. TC and IE drafted the paper. TC, IE, AG, BW, JH, CN and AT critically revised the paper for important intellectual content and approved the final version to be published.
Funding This study was funded by the Stockholm County Council and the Public Health Agency of Sweden.
Competing interests None declared.
Ethics approval The study was approved by the regional ethics committee at Karolinska Institutet, Sweden (ref. no 2015/158-31).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Additional data are available by emailing the corresponding author.