Article Text

Statistics from Altmetric.com
Managed care and disability management of sicklisted patients is a topic for discussion.1 It is stated frequently that ineffective medical care of patients may result in a serious risk of unnecessarily (long) absenteeism, iatrogenesis, and even permanent disability. According to Bruckman and Harris, barriers for return-to-work or even iatrogenesis can originate from the treating physician; they described several ineffective medical practises that may delay functional recovery.2
Unnecessary long absenteeism or iatrogenesis can also be caused by fragmented and poorly coordinated medical care of sicklisted workers.3,4 A common reason for unnecessary lost days is that treating physicians have too little information about the physical demands of the job to make an appropriate decision as to when and how the worker can return to work.5 In addition, many treating physicians do not recognise the work relatedness of diseases, because they have no training in occupational medicine.5–7 For these reasons cooperation between general practitioners (GPs) and occupational physicians (OPs) is recommended in recently published occupational health guidelines for the management of low back pain.8 Opinion surveys in both the UK and the Netherlands indicate, however, that cooperation between GPs and OPs in disability management is poor.9,10
Although it is often stated that medical practises of treating physicians can be obstacles for return-to-work, and that cooperation in disability management between OPs and treating physicians is poor, there appears to be no systematic study regarding these issues. Consequently, the objectives of this study are to investigate: (1) obstacles for return-to-work in general and in medical management; and (2) occurrence and content of communication in disability management between OPs and treating physicians regarding low back pain patients. In order to obtain an accurate picture of the obstacles for return-to-work and communication in disability management, we investigated data on the medical management of 300 low back pain patients who were sicklisted for 3–4 months.
STUDY DESIGN AND METHODS
This Dutch research project formed part of the international comparative study “Work Incapacity and Reintegration”.11 This was a prospective cohort study in which patients who were sicklisted for 3–4 months because of low back pain were followed up for two years in six countries. For this international comparative study, a cohort of patients was selected on the basis of the following inclusion criteria12:
-
Being sicklisted and receiving full or partial compensation for at least three months because of low back pain (ICD-9 codes 721, 722, 724). Patients with low back pain caused by fracture, inflammation, or malignancy of the spine and patients with spinal surgery in the past year were excluded.
-
Having a paid job and an employer who has contracted an Occupational Health and Safety Service (OHS).
-
Age between 18 and 60 years.
The recruitment of the Dutch cohort was performed in cooperation with the Social Security administration. A consecutive series of 1890 patients with back pain was selected in the period November 1994 to February 1995. These patients were asked by mail to participate in the study. A total of 1087 (58%) patients agreed to participate and signed a letter of authorisation, drawn up according to the guidelines of the Royal Dutch Medical Association, permitting their OP to make available the data to be used for this study. Non-response analysis showed that there was hardly any difference between the response group and the non-response group with regard to demographic characteristics.12 The inclusion criteria were checked by an answer form, filled in by the patients themselves. A total of 620 patients did not meet the inclusion criteria, finally resulting in a cohort of 467 patients.
Between January and June 1995 (after three months of absenteeism because of back pain), a questionnaire was sent to the OP of every patient that was included in the cohort. In this questionnaire questions were asked regarding the medical management of the patient concerning the diagnosis (ICD-9 codes), treatment, functional disabilities, factors influencing return-to-work (on a three point scale: a factor has an inhibiting, promoting, or no role in return-to work), communication with the treating physicians, and the content of this communication (on a two point scale: a subject was discussed between the OP and treating physician, or not discussed). When included in the cohort at three months of sickleave, every patient was asked about low back pain related and work related characteristics such as pain intensity (Von Korff), back pain history, working hours, and working status.
Statistical methods
All presented proportions have been calculated after excluding missing data. Factors influencing return-to-work, according to the OP, were dichotomised: (1) factors inhibiting return-to-work; (2) factors promoting return-to-work, or factors which played no role in return-to-work. Results of univariate analysis are presented as odds ratios (odds of a communication regarding participants identified by a factor inhibiting return-to-work, compared with the odds of a communication regarding participants without that inhibiting factor). The corresponding 95% confidence intervals (95% CI) for the odds ratios (OR) are calculated.
Multiple logistic regression analysis was used to identify independent predictor variables (significant at p < 0.05). Potential predictor variables were those listed in table 3. Additional variables examined were age, gender, and working status when the patient was included in the cohort. Results of multiple logistic regression analysis are presented as odds ratios, adjusted for the other variables—that is, all other inhibitory factors, age, gender, and working status. Analysis was carried out using SPSS for Windows, release 7.5, 1997.
RESULTS
The OPs of 300 (64%) of the 467 patients in the cohort participated in the study. They completed the questionnaires at an average of 4.5 months after the first day of absence from work. Non-response analysis showed that there was no difference between the subgroup of patients for whom the OP had returned the questionnaire and the total cohort, with regard to either the demographic characteristics or the patient reported aspects of the medical treatment. Table 1 presents the characteristics of the 300 patients sicklisted for 3–4 months with low back pain. OPs who had not returned the questionnaire were questioned by telephone in order to gain insight into reasons for their non-response. The main reasons for not responding were lack of time or the absence of the patient’s medical file (due, for example, to reorganisation of the OHS or a switch of the patient’s company to another OHS).
Baseline characteristics of the cohort of patients sicklisted for 3–4 months
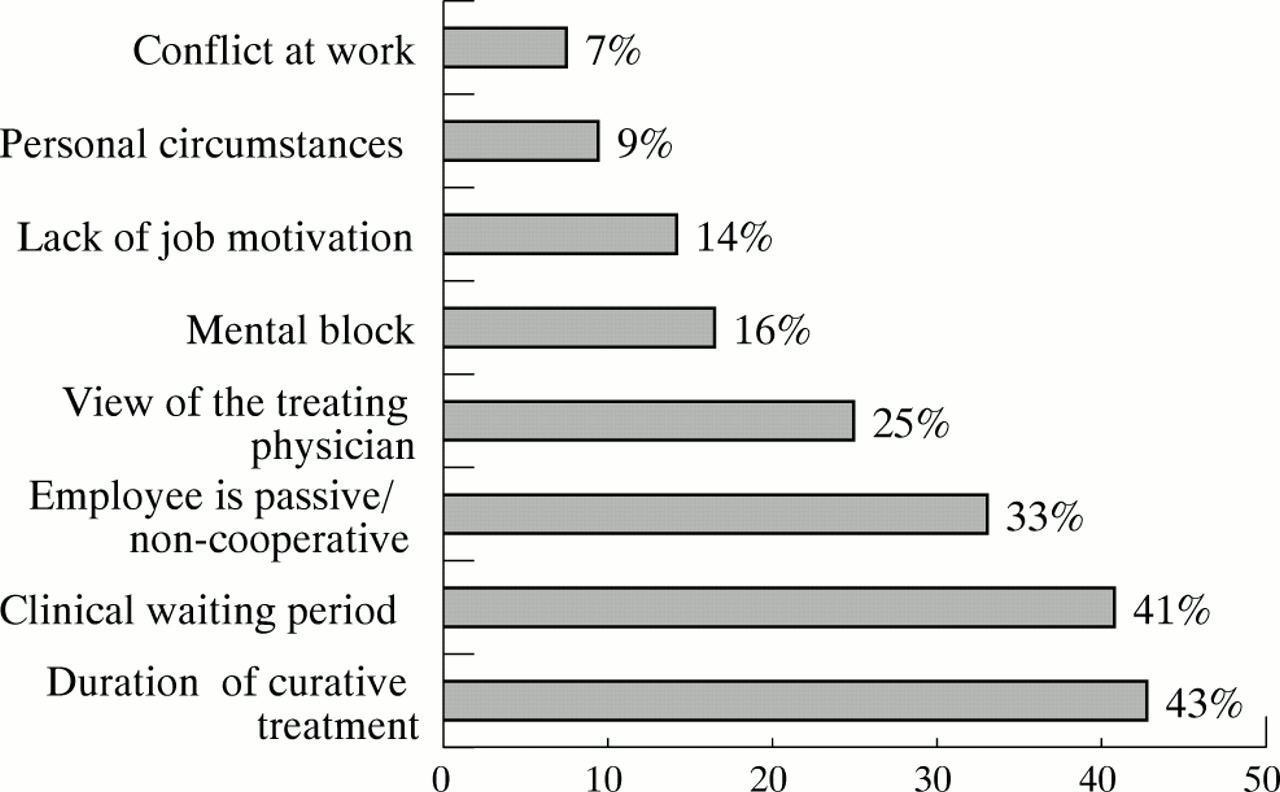
The OPs reported a number of obstacles for return-to-work in the 300 patients sicklisted for low back pain (see fig 1). The OPs felt that the duration of treatment and the waiting time before treatment had had an inhibitory effect on the return-to-work, in 43% and 41% of the cases, respectively. According to the OPs, the view of the treating physicians regarding return-to-work of the patient was an inhibitory factor in 25% of cases. In the opinion of the OPs, 33% of cases showed a passive attitude with regard to return-to-work. Psychosocial factors such as mental blocks (16%), lack of job motivation (14%), personal circumstances (9%), and conflict at work (7%) were less frequent obstacles to return-to-work, in the opinion of the OP.

{kind=link}
Factors inhibiting return-to-work in low back pain patients (n = 300) sicklisted for 3–4 months, in the opinion of their occupational physicians.
In 56 (19%) cases there was communication between OP and treating physician; in another 14 cases the OP was planning to contact the treating physician in the immediate future. There was thus either actual or intended communication between OP and treating physician in a total of 70 cases (24%). In 43 of these cases the communication consisted of consultation with the general practitioner, in 23 cases with a specialist, and in 20 cases with a physiotherapist. The OPs indicated that communication with a treating physician was almost always for the purpose of requesting and exchanging information on diagnosis, treatment, and prognosis. Other subjects, such as an attempt to reach a common policy on case management, were less often the subject of communication between the OP and the treating physician (see table 2).
Reasons for consultation by the OP of the treating physician in 70 low back pain patients sicklisted for 3–4 months (n=300)
Finally, we investigated whether there was more communication between the OP and the treating physicians in the presence of obstacles for return-to-work (see table 3). Such communication was limited in general, but occurred most frequently in the presence of psychosocial obstacles: mental blocks (36%), a lack of job motivation (40%), and passivity with regard to return-to-work (39%). Communication was even more limited when OPs felt that the waiting period (32%), duration of treatment (30%), and view (28%) of treating physicians inhibited return-to-work. We used multiple logistic regression analysis to identify independent predictor variables for the occurrence of communication. Communication between OPs and treating physicians was significantly associated with the following obstacles for return-to-work: passivity with regard to return-to-work and clinical waiting period; adjusted OR were 3.35 (95% CI: 1.64 to 6.82) and 2.23 (95% CI: 1.04 to 4.79) respectively. All other inhibiting factors, gender, age, and working status were not significantly associated with communication.
Proportions of cases leading to communication when the factor was inhibitory in low back pain patients sicklisted for 3-4 months, in the opinion of the occupational physician (n=300)
DISCUSSION
To our knowledge, this is the first study to investigate obstacles for return-to-work by ineffective disability management of treating physicians, based on data concerning the medical management of a cohort of 300 low back pain patients. The literature on this subject has been based principally on opinions of authors.1–7 Surveys have shown that there are differences in the perception of frequency with which communication between OPs and GPs occurred.9,10 There is, however, no systematic study on the communication between treating physicians and occupational physicians in a well described patient population.
Factors inhibiting return-to-work
In our study it was found that OPs considered the inhibitory effect of treating physicians to be of great influence on return-to-work of low back pain patients sicklisted for 3–4 months. In the opinion of the OPs, psychosocial factors only play a secondary role in a delay in return-to-work in these patients.13,14 Treating physicians should pay more attention in the medical management of their patients to the prevention of absenteeism and disability, according to OPs. This finding is supported by many publications about medical practises delaying return-to-work in patients with back pain. For example, treatment with exercise therapy in cases of acute low back pain has been shown to prolong absenteeism.15–17 Diagnostic labelling of patients presenting with back pain can also have detrimental effects on outcome.8,18 Van Wolde showed that in the Netherlands in general, absenteeism from work is prolonged by the long waiting periods for consultation of orthopaedic surgeons and neurologists.19 Finally, it has been shown that in cases of back pain, therapeutic recommendations for (bed) rest or (undesirable) pain related advice may confirm the patient in his pain avoiding behaviour and thus inhibit return-to-work and prolong absenteeism.17,20
Frequency and content of communication
In our study, communication between the OPs and the treating physicians regarding low back pain patients sicklisted for 3–4 months, was limited. Our findings are in agreement with those of two surveys regarding the perception of the frequency of communication between GPs and OPs.9,10 According to both surveys the lack of regular communication can be explained by misunderstandings of treating physicians about the role and responsibilities of OPs.9,10
In our study the content of the communication almost always concerned the informative exchange of factual data; communication in a broader sense, such as harmonisation of the case management policy, occurred much less frequently. Our results regarding the content of communication support the findings of the above mentioned Dutch survey,9 as well as the outcome of an audit on the communication between one OP and GPs carried out in the UK.21 However, a limitation of our and the other studies is that the communication between OPs and treating physicians may also be varied in terms of type and nature. The possible explanation for the mainly informative exchange of factual data may be the legal rules of behaviour concerning the exchange of medical data in work related matters. These rules were constructed for privacy and confidentiality reasons,5 and do not allow a “free” exchange of information. The point of departure for these rules is that treating physicians may provide only factual data to OPs in response to concrete questions, and only with written consent of the patient.22
Lack of communication regarding obstacles for return-to-work
According to their respective clinical guidelines on back pain management, OPs and treating physicians have a common goal: the prevention of dysfunction and prolonged disability.8,23,24 Furthermore, there is moderate evidence that communication and cooperation between OPs and GPs regarding workers with low back pain is fundamental for improvement of clinical and occupational health management and its outcomes.8 According to the Dutch guidelines on the management of low back pain, the OP should contact the treating physicians if, in his opinion, the medical management is inadequate, or is inhibiting return-to-work.24,25 In contrast to what one might expect, our study has shown that only a small proportion of the OPs who reported that treating physicians had an inhibitory effect on return-to-work, actually sought contact. There are two possible explanations for this lack of communication in the presence of obstacles in the medical management for return-to-work: (1) It is not yet common practice of OPs to debate the treatment pursued by their colleagues, although in our opinion by doing so the OP fails to coordinate adequately the disability management of the patient. (2) In practice, the treating physician and the OP still have different goals instead of common goals, when treating the same patient. The latter explanation seems in our opinion the most likely explanation for this phenomenon; while the treating physician concentrates on the diagnosis and treatment of back pain, the OP attempts to limit the level of dysfunctioning resulting from the back pain. In order to prevent obstacles for return-to-work by ineffective disability management of doctors, more education on this issue is needed in the medical course in order to agree on common goals in medical management for treating physicians and OPs and to increase bilateral cooperation.
Conclusions
(1) According to OPs, the clinical waiting period, duration of treatment, and the view of the treating physicians are obstacles for return-to-work of many low back pain patients sicklisted for 3–4 months. (2) Nevertheless the cooperation between OPs and the treating physicians in disability management of these patients is limited and is directed primarily at exchange of information, rather than at harmonisation of management policy.
Main messages
-
According to OPs the clinical waiting period, duration of treatment, and the view of the treating physicians are obstacles for return-to-work in 43%, 41%, and 25% of low back pain patients sicklisted for 3–4 months, respectively.
-
This systematic study confirms that communication between OPs and the treating physicians is very limited, despite the reported obstacles in return-to-work management.
-
Communication between OPs and the treating physicians is directed primarily at exchange of information, rather than at harmonisation of management policy.
Policy implications
-
More cooperation between occupational physicians and treating physicians is needed in return-to-work management of sicklisted patients in order to harmonise management policy and to agree on a common goal—that is, prevention of dysfunction and prolonged disability.
-
The results of this study suggest that more attention to prevention of (prolonged) absenteeism and to bilateral communication is needed in medical courses.
Acknowledgments
This Dutch research project is part of an international comparative study “Work Incapacity and Reintegration” and concerns the results of the Dutch contribution to this research project. It was carried out under contract with the Social Security Supervisory Board, the Netherlands Ministry of Social Affairs and Employment, and the Netherlands Ministry of Health, Welfare and Sports, with a grant from the General Disability Funds. Part of the results of this study was previously published in Dutch.26