Article Text

Abstract
Study objective: To determine if a self help intervention, delivered via written interactive materials (the “Walk in to Work Out” pack), could increase active commuting behaviour (walking and cycling).
Design: Randomised controlled trial. The intervention group received the “Walk in to Work Out” pack, which contained written interactive materials based on the transtheoretical model of behaviour change, local information about distances and routes, and safety information. The control group received the pack six months later. Focus groups were also conducted after six months.
Setting: Three workplaces in the city of Glasgow, Scotland, UK.
Participants: 295 employees who had been identified as thinking about, or doing some irregular, walking or cycling to work.
Main results: The intervention group was almost twice as likely to increase walking to work as the control group at six months (odds ratio of 1.93, 95% confidence intervals 1.06 to 3.52). The intervention was not successful at increasing cycling. There were no distance travelled to work, gender, or age influences on the results. Twenty five per cent (95% confidence intervals 17% to 32%) of the intervention group, who received the pack at baseline, were regularly actively commuting at the 12 month follow up.
Conclusion: The “Walk in to Work Out” pack was successful in increasing walking but not cycling. The environment for cycling must be improved before cycling will become a popular option.
- active commuting
- physical activity
- transport
Statistics from Altmetric.com
Recent UK government white papers on public health 1 and transport 2 established targets to increase participation in regular physical activity and associated improvements in the environment. The physical activity target aims to increase the percentage of the population accumulating 30 minutes of moderate physical activity on five or more days each week. Active commuting (walking or cycling part, or all, of the way to work) could contribute to these targets. Active commuting can improve fitness 3 but there is little information on how to increase this behaviour. This randomised controlled trial aimed to establish if a self help intervention, delivered via written interactive materials, could increase active commuting behaviour in workplaces. The intervention was based on the transtheoretical model of behaviour change, which has four core constructs.4 The constructs are stages of change, processes of change, self efficacy, and decision balance. The stages of change for active commuting can be described as follows:
-
Precontemplation: no intention to become more active in the next six months
-
Contemplation: thinking about becoming more active in commuting in the next six months
-
Preparation: having a plan of action (for example, buying a bicycle) or having attempted some active commuting but not enough to meet the minimum criteria of accumulating 30 minutes on most days of the week.
-
Action: people have become regular active commuters but only in the previous six months
-
Maintenance: achieved regular active commuting for longer than six months.
People make progress at different rates towards maintenance and may fall back from their current stage for a variety of reasons and this is described as relapse and is sometimes listed as a separate stage.
The processes of change are strategies that people use to help themselves to make change. Ten process have been identified and five of these are described as experiential and the other five as behavioural. The five experiential processes are consciousness raising, dramatic relief, self re-evaluation, social liberation, and environmental re-evaluation. The five behavioural processes are self liberation, counter-conditioning, stimulus control, reinforcement management, and helping relationships.
The third of the key constructs in the transtheoretical model is self efficacy. Self efficacy for exercise and physical activity has often referred to a person's confidence that they can overcome typical barriers to exercise. The final construct is decision balance, which refers to the weighing up of the pros and cons of changing a particular behaviour.
The purpose of this study was to determine if a self help intervention, based on the transtheoretical model, could increase active commuting behaviour in a worksite setting. The intervention described in this paper targeted those who were thinking about active commuting (contemplators) and those who were irregular active commuters (preparers), invited participants to undertake a decisional balance process, suggested ways of enhancing self efficacy for active commuting and emphasised processes of change, such as consciousness raising, which have been reported as useful in early behaviour change.
METHODS
Protocol
Advertisements inviting participation in the project were posted electronically, by internal mail, and via paycheques to all employees in three city workplaces. All workplaces were in the same area of the city and served by good public transport links and by marked cycle routes. All three workplaces were large public sector organisations with a spectrum of socioeconomic groups within the workforce. One workplace was an acute hospital trust with a workforce of approximately 4000, one workplace was a university also with a workforce of approximately 4000, while the third workplace was a health board with a smaller workforce of approximately 350. Thus, there was representation from large and medium sized workplaces. Over a three month period, interested participants completed a screening questionnaire to identify their stage of change for active commuting. Participants identified as contemplating or preparing to actively commute (n=333) were sent a baseline questionnaire that measured demographic variables and contained the main outcome measures, which were: stage of change for active commuting (adapted from Marcus et al),5 seven day recall of physical activity,6 and perceived physical and mental functioning measured by the SF-36 scale.7 Other variables measured will be reported elsewhere. Those who returned the baseline questionnaire (n=295) consented to their involvement in the project. A power calculation suggested a minimum of 270 participants given the following assumptions: a minimum important difference between the groups in terms of movement to a higher category of stage of change was defined as 15%; the predicted proportion of subjects in the control group moving to a higher category of stage of change was 10%; a statistical power of 80% at a significance level of 5%; and 25% loss to follow up from each group. The project was approved by the local university ethical committee.
Assignment
The research assistant entered baseline data into the data management system. The system automatically matched respondents on distance travelled to work (under two miles, two to five miles, over five miles) and then randomly assigned them to control or intervention groups. This automatic procedure was not accessible to the research assistant entering the data. The statistician remained blind to group identity. The intervention group received the “Walk in to Work Out” pack immediately and the control group was told that the pack would be forwarded in six months time. The control group was not requested to refrain from beginning active commuting. Thus participants were not blind to treatment.
Participant flow and follow up
Follow up questionnaires, repeating the outcome measures collected at baseline, were sent at 6 and 12 months to both groups. Three attempts were made to contact non-respondents before categorising them as lost to follow up. The flow of participants in the trial is shown in figure 1. Data were analysed on an intention to treat basis in that all respondents were included whether or not they had changed active commuting behaviour.

Flow of participants through the trial.
The intervention
The intervention consisted of a pack entitled “Walk in to Work Out”. The pack had been pre-tested on a local population. It contained a booklet with written interactive materials based on the transtheoretical model of behaviour change, educational, and practical information on: choosing routes, maintaining personal safety, shower and safe cycle storage information, and useful contacts. The pack also included an activity diary in the form of a wall chart, a workplace map, distances from local stations, local cycle retailers and outdoor shops, contacts for relevant organisations, local maps, and reflective safety accessories. The pack was specially designed for use in the research study. The cost of the initial design and print was £10 000 for the printing of 1000 folders and 300 full sets of inserts. Additional pre-testing with target groups cost £2000. Maps showing local cycle and walking routes and reflective safety strips included in the pack were provided by the local authority.
Focus groups
Focus group discussions were conducted, after the six month responses had been received, on subsamples of walkers and cyclists who had progressed or regressed in active commuting stage of change. Five focus groups were conducted and 27 participants contributed. Table 1 shows the participants in each group. All discussions lasted approximately one hour and were tape recorded. Typed verbatim transcripts of the discussion were then analysed using methods described by Miles and Huberman.8 The data obtained from the focus groups were examined for participants motivations and barriers for active commuting.
Focus group participants
Statistical analysis
Those who progressed over the first six months in stage of change for active commuting were compared with those who did not progress or regressed. The comparison was modelled by stepwise logistic regressions on the main effects and interactions of the three potential explanatory variables (age, gender, and distance travelled to work) as well as study group (intervention or control).
The logarithm of the time spent walking to work per week at six months was modelled by means of an analysis of covariance on study group and the logarithm of the time spent walking to work at the start of the study. Taking logarithms of the times was required to meet the assumptions of linearity and conditional normality in the analysis of covariance model. The 95% confidence intervals for the population changes in each of the SF-36 variables and processes of change (from the start of the study to six months) were standard normal two sample t intervals based on the difference of the changes across the six months. The 95% confidence intervals for population proportions (for example, for those who progressed to higher stage of change for active commuting) or differences in such between the study groups are all based on the standard large sample approximations for binomial parameters.
RESULTS
Completed baseline questionnaires were received from 295 participants (intervention group n=145, control group n=150). The mean age was 38 years (range 19 to 69 years), 64% (n=186) were women and 36% (n=109) were men. Most participants were members of social economic class 1 and 2, that is they were in the professional and managerial categories (76%, n=224). The majority of participants travelled between 2 and 10 miles to work (70%, n=207) and travelled by car (73%, n=215).
Stage of change for active commuting
The response rate at six months was 66% (n=194). Over six months, a significantly larger percentage of the intervention group (49%, n=50) progressed to a higher stage of active commuting behaviour change compared with the control group (31%, n=29). The average difference between the two groups was 18% (95% confidence intervals 5% to 32%). A logistic regression of change (progress in stage of change versus no change or regression in stage of change) in active commuting stage of change (six month minus baseline) was carried out to identify any effects of distance travelled to work, gender, and age and all interactions thereof. Analysis showed that none of these variables, or their interactions, significantly influenced the probability of improvement in active commuting stage of change over the first six months.
Walking
Analysis of the seven day recall of physical activity data showed a significantly greater average time per week spent walking to work for those in the intervention group compared with controls, among those who had not walked to work at the start of the study (sample means of 125 minutes per week for the 14 such persons in the intervention group and 61 minutes per week for the 12 in the control group). There was also a significant increase in the average time spent walking to work per week, in favour of the intervention group, among those who already walked to work (a sample mean increase from 52 minutes per week at baseline to 79 minutes per week at six months for the 61 such persons in the intervention group compared with an increase from 50 to 60 minutes per week for the 43 such in the control group). The full analysis here used an analysis of covariance (using logarithms) of the time spent walking to work at six months on the (logged) time walked to work at baseline compared across the two groups. This resulted in an estimated average relative increase in the time spent walking to work at six months, for someone given the intervention, of 1.93 (95% confidence intervals of 1.06 to 3.52) times any increase in walking time for a corresponding control who walked the same amount at baseline.
Cycling
The intervention was not successful in increasing cycling. Only 18 participants reported cycling to work at six months. There was no difference in the reported average weekly minutes of cycling between cyclists in the intervention group (n=9) and control group (n=9).
SF-36
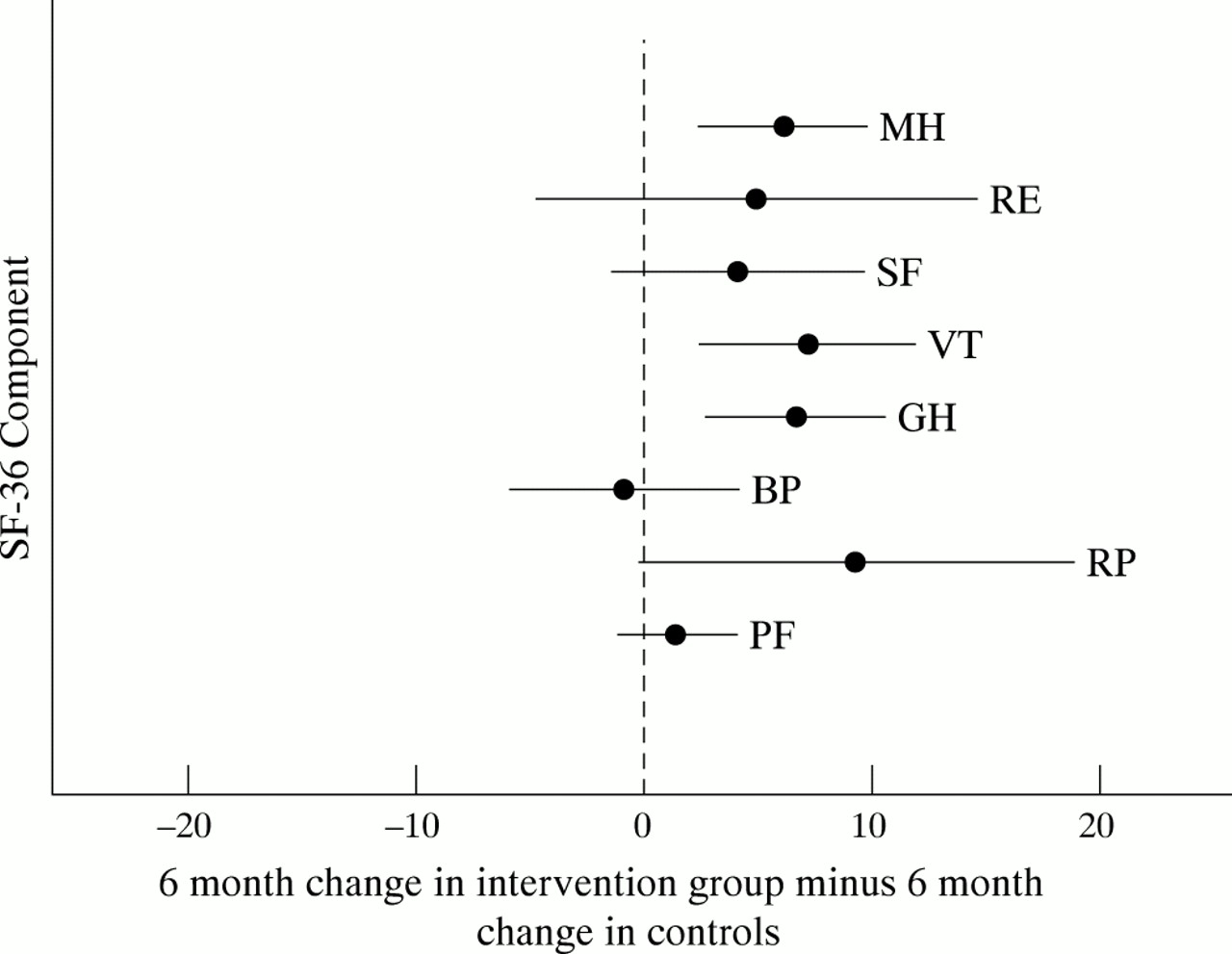
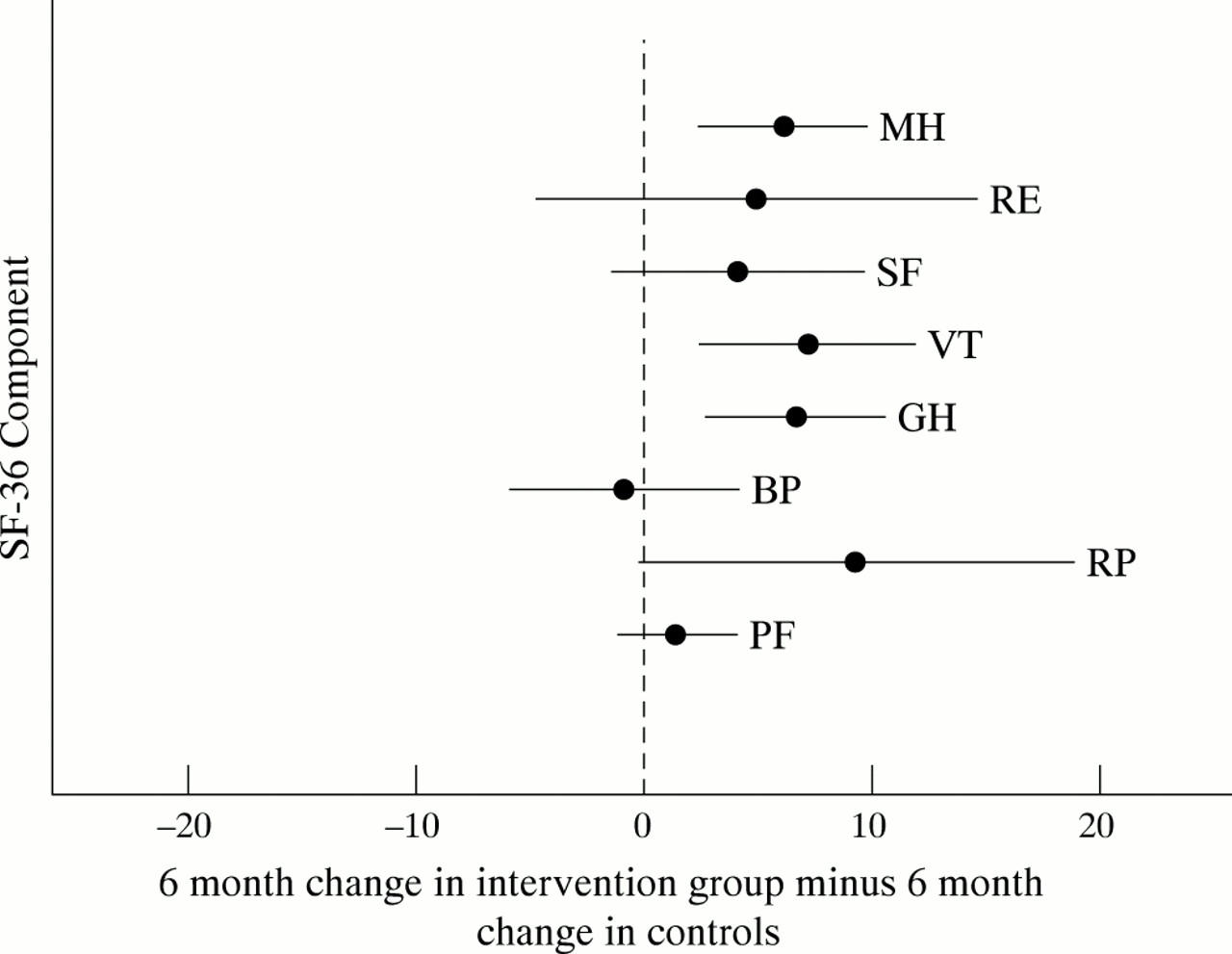
A comparison of the subscales of the SF-36 from baseline to six months showed that individuals in the intervention group improved their scores significantly more than the control group on three of the eight SF-36 subscales. For the Mental Health subscale the intervention group improved in terms of sample mean score from 72 to 76 at six months while the control group sample mean scores over the same time period were 73 and 71. For the Vitality subscale sample mean change for the intervention group was from 57 to 64 while the control group produced a sample mean score of 61 at both time points. Finally, on the General Health subscale, the sample mean scores were 71 at baseline and 76 at six months for the intervention group and 75 and 73 respectively for the control group. These changes indicate enhanced perceptions of physical and mental health functioning for the intervention group. Four of the other five subscales showed greater average increases for the intervention group but they were small and not significant at the 5% level. These results are illustrated in figure 2.
{kind=link}
{kind=link}
The 95% confidence intervals of six month change in SF-36 scores for intervention group minus six month change for control group. MH, mental health; RE, role emotional; SF, social functioning; VT, vitality; GH, general health; BP, bodily pain; RP, role physical; PF, physical functioning.
Processes of behaviour change
There was no difference between intervention group and control group, or between those who had progressed in stage of change versus those who had not progressed, in terms of the utilisation of the 10 processes of change that are associated with the transtheoretical model of behaviour change. The most frequently used processes were self liberation, counter conditioning, and self re-evaluation, with stimulus control and helping relationships being used least.
Focus groups
Focus group discussions were conducted, after the six month responses had been received, on subsamples of walkers who had progressed or regressed in active commuting stage of change. Both groups listed similar barriers to active commuting. What discriminated between the groups was that those participants who managed to maintain walking had developed coping strategies to overcome the barriers. Examples of these strategies were: buying waterproofs and rucksacks, and walking from work rather than to work when time pressure exists. Focus group discussions with cyclists showed that barriers were related to the cycling environment. Examples of these barriers were: pollution, other road users, lack of covered cycle locking facilities, state of repair of cycle paths, and safety. Focus groups reported that their workplaces did little to encourage the active commuter. Suggestions from focus groups of how employers can encourage active commuting are shown in table 2. We also elicited comments on the elements of the pack. Participants reported that the interactive tasks were useful at the beginning and that they found the local maps and distance charts (which showed how long it would take to walk to local train and bus stops from each workplace) very useful.
Suggestions from focus group participants of how employers can promote active commuting
12 month results
The response rate at 12 months was 56% (n=166). The control group was given the intervention materials at the six month point. The percentage of participants in the control group who progressed from the stage of active commuting behaviour change recorded at six months to a higher stage at 12 months (46%, n=31) was similar to the percentage in the intervention group who progressed their stage of change in the first six months (49%, n=50). The 95% confidence intervals for the difference between the two percentages was −16% to 17%.
Twenty five per cent (95% confidence intervals 17% to 32%, n=36) of the intervention group (n=145), who received the intervention at baseline, had changed their active commuting stage of change to action or maintenance (that is, regularly actively commuting) at 12 months.
DISCUSSION
The “Walk in to Work Out” pack was effective in increasing walking part or the entire journey to work over a six month period and the intervention group also reported increased perceptions of physical and mental health functioning. If we assume that average walking pace is 5 km per hour, for those who were in contemplation stage at the beginning of the study, the intervention group were doing 10.4 km per week at six months compared with the controls who were doing 5 km per week. For those who were in the preparation stage at the beginning of the study, the intervention group added 2.3 km per week to what they were doing at the start of the study while the controls added 0.8 km. Thus the intervention group achieved more than double the increase in walking achieved by the control group at six months. People who changed their behaviours reported a variety of methods of creating active journeys. These included: adding walking to bus journeys by getting off the bus early; walking to the next bus stop; declining a regular lift in others peoples' cars; using public transport more; parking further away from normal destinations; taking a bicycle in the car and parking at the end of a cycle route; and in one instance selling the car.
Twenty five per cent of the initial intervention group, who were contemplating or preparing to actively commute at baseline, were regularly actively commuting to work one year after they received the intervention, which compares well with interventions aimed at changing other health behaviours. For example, only 2% of smokers successfully quit and did not relapse after one year following personal advice on how to stop.9
After the study several design alterations were made to the pack to respond to lessons from the research. It was subsequently reprinted by the Health Education Board for Scotland for national use at the cost of £1 per pack. Scottish workplaces can access the amended pack free of charge through their local health promotion department. Continued use of the pack will require only reprint costs supplemented by the use of existing resources (such as local maps and leaflets). Provided internal mailing systems are used the intervention can therefore be repeated at a minimal cost. This suggests that the “Walk in to Work Out” pack is a comparatively cheap and effective way of achieving recently set population targets for physical activity 1 and the environment.2
The intervention was not successful in increasing cycling. This finding is likely to generalise to cities similar to Glasgow, which have cycle routes and maps, but limited separation of cyclists from traffic. The intervention material may be more successful in increasing cycling in rural settings or settings in which there is significant separation of cyclists from traffic and that should be tested in future research. However, Wardman et al10 have suggested that increases in cycling are unlikely to be achieved by provision of cycle routes alone. Recent research suggests that a significant shift to cycling will only happen if coordinated action is taken in three areas: promotion of individual and social behaviour change, promotion of organisational change, and implementation of situational and environmental measures.11 We also recognise that the emphasis on the campaign, as inferred by the title, was walking, although plenty of information for cycling was provided.
Key points
-
Active commuting (walking or cycling some or all of the way to work) is one means of increasing physical activity.
-
There has been little investigation into ways in which active commuting can be encouraged.
-
This randomised controlled trial showed that self help materials can increase walking to and from work.
-
The intervention was not successful in increasing cycling.
Policy implications
-
The 1999 Charter on Transport, Environment and Health14 calls for the public to be informed of, and take individual action to alleviate, the negative health and environmental impacts of transport. This intervention increased individual walking patterns and can contribute to the limited evidence base for encouraging active commuting.
-
Increasingly, statutory agencies are jointly developing local green commuter plans. As well as structural and financial incentives for change, such plans should recommend evidenced based interventions such as “Walk in to Work Out” that will encourage uptake and adherence to active commuting by their employees and service users
-
Given the health and financial burden of coronary heart disease and obesity within Europe and the US, and the importance of physical inactivity as a risk factor for these conditions, there should be a greater research focus on how to initiate and sustain behaviour change through both environmental and mediated individual support.
-
The Health Education Board for Scotland and the UK Department of Transport Local Government and the Regions, has adopted the “Walk in to Work Out” materials to use as part of their efforts to encourage workforces to promote green transport polices and increase physical activity participation to meet national targets.
There were no adverse effects noted from this intervention such as traffic accidents. There were no gender, age, or distance to work effects noted. This suggests that the pack will be useful to a wide variety of employees. However, more women than men responded to the opportunity to be involved in this project, which may suggest this form of activity is more appealing to women.
Surprisingly, the processes of change, which are part of the transtheoretical model of behaviour change, did not explain movement in active commuting behaviour change at six months. Other researchers 5 have been able to describe changes in process use over time but it has been recognised that the measurement of the processes of change for physical activity, which were modelled on those processes that were most frequently used in smoking cessation, does need to be improved.4 It is suggested that the current instrument is not specific enough for active commuting. Further research is needed to comprehend the processes involved in adopting and maintaining active commuting. It may be that there are other processes that influence the adoption of active commuting. These may be family or work constraints or they may be infrastructural factors such as safer routes.
Our results support those of Vuori et al 3 who reported a 7% increase in active commuting from an intervention in a Finnish workforce. However, the study by Vuori et al was not a RCT and the intervention was not only focused on behaviour change but included management support, fitness testing, and environmental change. Moreover, the Finnish workforce reported higher levels of active commuting before the intervention and the environmental conditions are different to those in Glasgow. There is therefore a need to test the “Walk in to Work Out” pack in other settings.
Limitations
The majority of participants in our study were economically advantaged women from medium and large sized workplaces and were car owners. This limits the generalisability of the findings but it is argued that car owners are a key target group for active commuting promotion and that women are a key target group for increasing activity levels. The findings are dependent on self report measures. However, a subsample of 16 participants volunteered for a more objective study of two complete journeys after the six month follow up. We observed the journeys using heart rate monitors and pedometers and performed laboratory tests of maximal oxygen uptake. We found that the average journey time for walkers and cyclists was 25 minutes and the mean MET value for walking and cycling respectively was 4.8 and 7. We therefore have some evidence to suggest that journeys provide sufficient duration and intensity for health and fitness gains.12 Forty four per cent of the original participants had dropped out or failed to respond by the 12 month follow up. However, this is a common finding in other areas of physical activity promotion.13
Conclusions
Workplaces should use the intervention pack to promote active commuting. The packs must be individualised to provide maps and distances relative to that workplace. Information on how to obtain the pack is available from the Health Education Board for Scotland (www.hebs.scot.nhs.uk). Future research should focus on how to raise awareness of active commuting and how to assist people to maintain this behaviour in the long term.
Acknowledgments
We thank a local advisory board involving Sharon McNeish, Daniel Wight, Hugh Harris, and Roger Downie for guidance on the conduct of the project, the Robertson Centre for Biostatistics for advice on data management, Karen Elliot for secretarial support, the participants for responding, and two anonymous referees for helpful comments.
Funding: Scottish Executive, Chief Scientists Office, for the conduct of the randomised controlled trial and the Health Education Board for Scotland and Greater Glasgow Health Board for funding the development of the written materials for the intervention.
Conflicts of interests: none.
Linked Articles
- In this issue