Article Text

Abstract
Background: Improvement 1–2 years after head injury is well established but the pattern thereafter is unclear. Past studies have not examined representative head injury populations and typically report findings in terms of functioning across social, psychological, neurobehavioural, or cognitive domains rather than global outcome.
Objective: To determine the late outcome of a representative cohort of participants admitted to hospital after a head injury 5–7 years previously and to identify early and late factors correlating with persisting disability and change between one and 5–7 years.
Methods: A representative cohort of head injured people whose outcome one year after injury was reported previously, were followed up 5–7 years after injury. Participants were assessed using structured and validated measures of global outcome (Glasgow Outcome Scale Extended), cognitive impairment, psychological wellbeing, health status, and social factors.
Results: Of 475 survivors studied at one year, 115 (24%) had died by seven years. In survivors at 5–7 years, disability remained frequent (53%); and the rate, similar to that found at one year (57%). Sixty three participants (29%) had improved but 55 (25%) deteriorated. The persistence of disability and its development after previous recovery each showed stronger associations with indices of depression, anxiety, and low self-esteem than with initial severity of injury or persisting cognitive impairment.
Conclusions: Admission to hospital after head injury is followed 5–7 years later by disability in a high proportion of survivors. Persistence of disability and development of new disability are strongly associated with psychosocial factors that may be open to remediation, even late after injury.
- CHI, Community Health Index
- DRS, Disability Rating Scale
- GGNHSB, Greater Glasgow National Health Service Board
- GOSE, Glasgow Outcome Scale-Extended
- outcome
- head injury
- disability
Statistics from Altmetric.com
- CHI, Community Health Index
- DRS, Disability Rating Scale
- GGNHSB, Greater Glasgow National Health Service Board
- GOSE, Glasgow Outcome Scale-Extended
A representative cohort of young people and adults with a head injury who had been admitted to hospital in Glasgow had a surprisingly high rate of persisting sequelae when followed up one year later.1 This was found even among those considered initially to have a mild head injury, and the data indicated that annually 150 per 100 000 (95% Cl 138 to 169) young people and adults remain disabled a year after head injury. The potential for long lasting consequences highlighted the need to discover the status of the cohort five years later, and to seek features associated with disability.
Change in outcome can continue for several years after a head injury but few previous studies make comparisons between findings at one and 5–7 years in the same sample.2–5 Even these studies fail to follow up a high proportion or a representative sample of their original cohort. Indeed, Corrigan et al6 note systematic bias in long term studies of head injury because of selective loss to follow up of people with socioeconomic disadvantage, a history of substance abuse, or who were victims of violence. Where comparisons in the same participants are made between 1–2 and 5–7 years, improvement and deterioration is reported in some cases, 5 in employment,3–5 neuropsychological, and cognitive functioning,2,3,7 and in emotion and behaviour.2,3 Only a modest proportion of the variation in late outcome is accounted for by the initial severity of brain injury,8,9 and this relationship may weaken over time.3
However, most studies do not consider relationships between cognitive, emotional, and injury factors in relation to improvement and deterioration, but simply describe outcome at five years or more after injury. These relationships are relevant because even years after injury, factors might be identified that are amenable to intervention to alleviate late disability. The aims of the study now reported were therefore to determine the late outcome of a representative cohort of participants admitted to hospital after a head injury 5–7 years previously, to compare participants’ outcomes at one year, and to identify early and late factors correlating with disability and change between one and 5–7 years.
PARTICIPANTS AND METHODS
Sample
The cohort was recruited initially between February 1995 and February 1996 from five general hospitals to which patients with acute head injuries are admitted in Glasgow. During this one year period 2995 young people and adults were prospectively identified as being admitted to hospital with a head injury and characterised. All of those with either a severe injury (GCS = 8 or less, n = 102) or a moderate injury (GCS 9–12, n = 133) and a random sample of those with a mild/minor injury (GCS 13–15, n = 507) were selected for follow up. This was achieved at one year in 74 participants who had died and in 475 survivors.1
The names and dates of birth of the 475 survivors who participated in the one year follow up study1 were provided to Greater Glasgow National Health Service Board (GGNHSB) who confirmed their general practitioner’s identity using the Community Health Index (CHI). This allowed each person to be allocated as follows; not registered with a GP, no trace of participant, moved outwith the GGNHSB area, deceased (date of death provided), or registered with a GP. For the last group, the name and telephone number of the GP was given. Participants who had moved outwith the GGNHSB area were traced via their new Health Board. GPs were asked to report any reasons why their patient should not be contacted.
Ethical approval
Approval for late follow up was given by the ethics committee in each of the original recruiting hospitals.
Contact with potential participants
Participants in the one year follow up and identified as suitable for the 5–7 year follow up were contacted by letter. For participants not registered with a GP, or who were not traced, the letter was sent to their last recorded address. Those who refused or were not traced after several attempts were considered lost to follow up. Consenting participants were written to or telephoned to arrange an appointment. The research assistant interviewed participants either at the Southern General Hospital, or at home if the participant was unable to travel. Consenting participants who were unable to meet with the research assistant took part in a telephone interview or completed a postal questionnaire. Participants who were interviewed in person underwent the full assessment/interview schedule, unless they declined part or all. Assessment of cognitive and emotional status was not possible for some people with reading, language, or learning difficulties or from those for whom contact was only by telephone or postal interview.
Assessments
Outcome
The principal index used to describe the cohort, as in the initial study, was the Glasgow Outcome Scale-Extended (GOSE). This has high interrater reliability and high validity, including strong relationships with cognitive indices, self-report indices of health, emotional and neurobehavioural features, and with service need and social autonomy.10–13 The assessors in the present study (LW) and in the previous study of outcome at one year (ST)1 each independently assessed a sample (n = 12) of head injured adults. Interrater reliability was extremely high (weighted Kappa of 0.97, 95% Cl 0.95 to 1.0) with perfect agreement in 10 of the 12 cases. Disagreement in the two cases was by only one category on the GOSE.
Physical health, employment status, and social factors
Assessments used at one year were repeated: a modified McKinlay Questionnaire,14 covering physical impairments, problems/difficulties experienced, and care needs; an employment questionnaire and a review of services received. Additional measures at the 5–7 year follow up were the AUDIT,15 and the DAST-1016 as indicators of alcohol use and drug abuse respectively. The Barthel Index17 was used to indicate disability in terms of activities of daily living. A health history questionnaire was used to record reports of further head injuries, hospital admissions, health problems, and psychiatric/psychological problems. Social deprivation was rated using an index, based on postal address codes.18
Emotional factors
Validated questionnaires used to assess aspects of mood were: the Hospital Anxiety and Depression Scale,19 a self-report scale to assess anxiety and depression; the Perceived Stress Scale20 to indicate current levels of stress; the Rosenberg Self-esteem Scale21 as an indicator of self-esteem; and the Multidimensional Health Locus of Control Scale22 (to provide information about beliefs about health).
Cognitive functioning
Information processing was assessed using the Speed of Comprehension Test,23 verbal memory and learning using the Auditory Verbal Learning Test24 and Immediate and Delayed Prose Recall,24 and executive functioning using the Hayling Test.25 Each test was standardised to a z score, the scores averaged and then transformed to a percentile score to obtain an overall cognitive function score. Premorbid IQ was estimated using a regression equation.26
Statistical analysis
The statistical presentation of the results is largely descriptive, with proportions or means and standard deviations reported as appropriate. Groups are compared formally using χ2 tests for categorical variables and t tests for continuous variables.
RESULTS
From the 2962 people in the original cohort, 769 participants were selected for follow up at one year and this was achieved in 71% (n = 549). The characteristics and categories of injury severity in those traced were representative of the full sample. One year after admission, 74 people had died, three were in a vegetative state, 117 were severely disabled, 141 were moderately disabled, and 214 had made a good recovery.
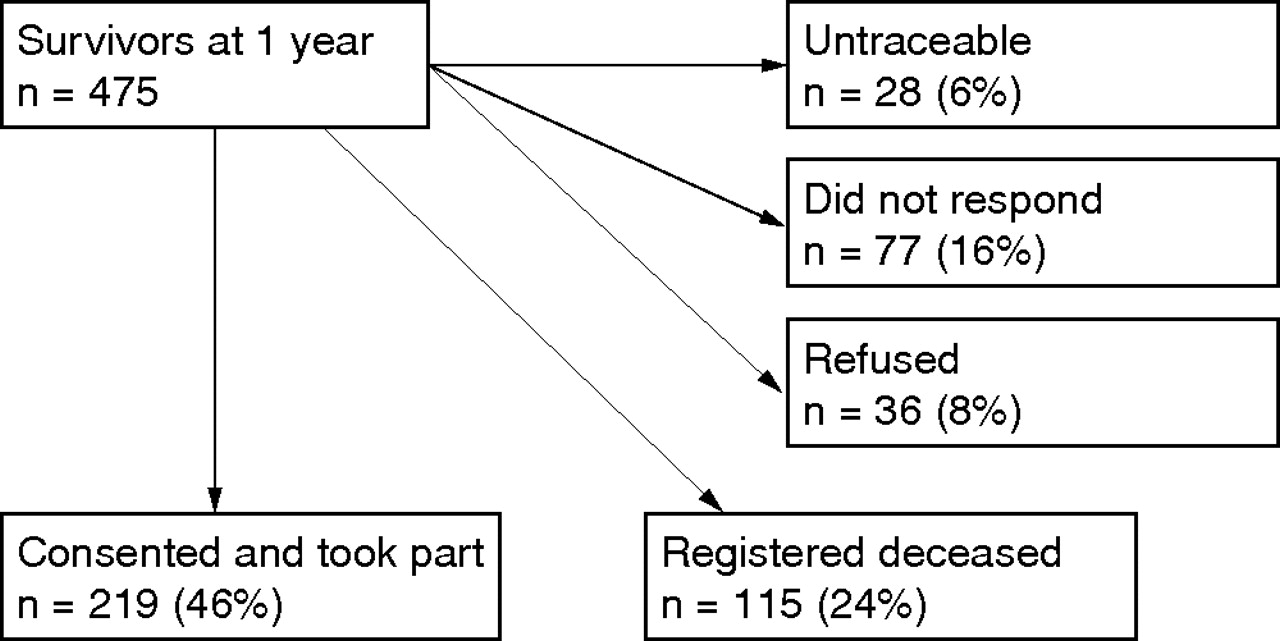
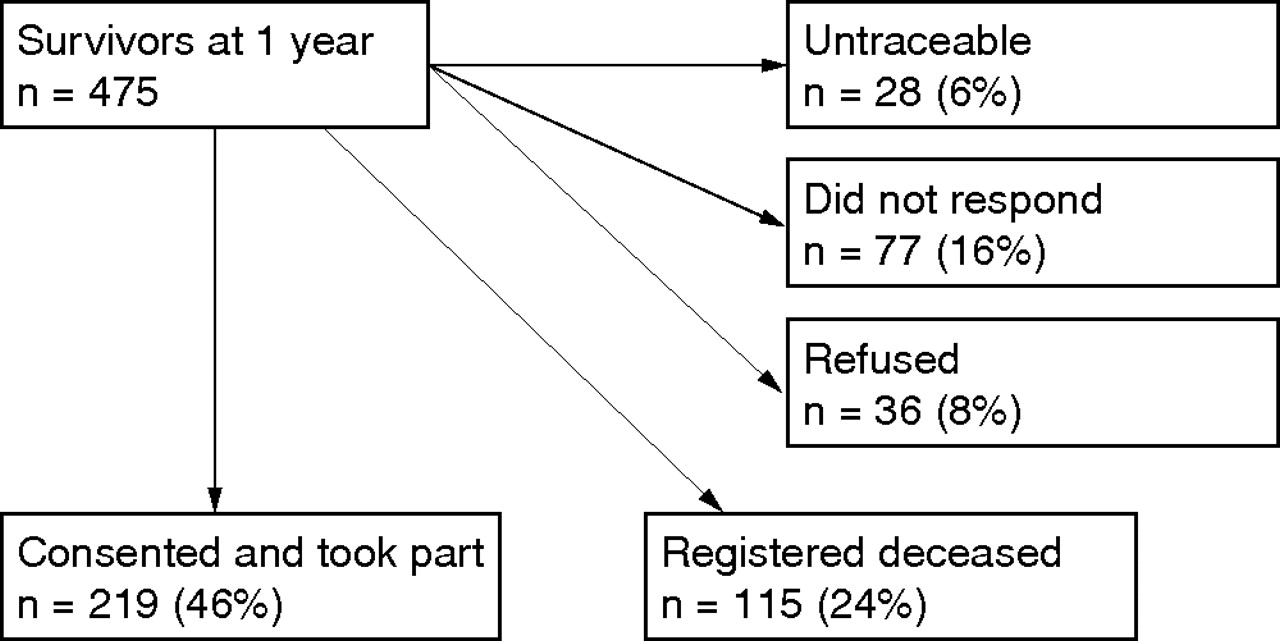
Figure 1 shows that of 475 survivors at one year, 334 (70%) were successfully followed up at 5–7 years. Of 360 survivors at 5–7 years, 219 (61%) consented to take further part and provided information that enabled assignment of outcome on the GOSE.
{kind=link}
Recruitment of cohort at 5–7 year follow up.
The 334 people who were followed up at 5–7 years consisted of 266 males and 68 females with a mean age of 40.4 years at injury. The early features of survivors (sex, initial severity, GOSE at one year, and index of social deprivation) who were untraceable or did not respond were well matched to the features of those who participated. However there was a substantial imbalance in age (50%>40 years v 23%, see table 1, p<0.001). This may be because tracing was more successful in those who had died with all of those who had died between 1 and 5 years after injury being aged over 40.
Comparison of characteristics of participants alive at one year with those traced and not traced at 5–7 years
Status of cohort 5–7 years after injury
Of the 219 survivors assessed at 5–7 years, 42 (19%) were severely disabled, 73 (33%) moderately disabled and 104 (47%) had made a good recovery. Disability was frequently found (53%), at a rate similar to that found at one year (57%). Sixty three participants (29%) had improved but 55 (25%) deteriorated.
In terms of activities of daily living, 87% of 161 participants were not disabled (Barthel Index; score 20) and less than 4% severely disabled (scores<10). Information on employment at 5–7 year follow up was available for 217 participants. Before injury, 160 (74%) of these were working or seeking employment, 49 (22%) were unemployed, and for eight (4%) work was not appropriate. This compares to 121 (56%), 72 (33%), and 24 (11%) at 5–7 year follow up.
Early factors and outcome
Death between one and 5–7 years after injury was strongly associated with age over 40 at time of injury (54% v 15%, p<0.001), with a history of brain illness before the event that resulted in recruitment to the original study (50% v 32%, p = 0.005), and with greater social deprivation (44% v 28%, p = 0.010). There was no association with severity of initial injury and this “late” mortality ranged from 36% after a mild injury to 24% after a severe injury. Allocation to a disabled outcome in survivors at 5–7 years was associated with an initially severe injury (76% v 50%, p = 0.036). Other early factors (age at injury, sex, previous head or brain injury, or social deprivation rating) were not significantly associated with allocation to disabled or good outcome (see table 2).
Association between early characteristics of participants and outcome at 5–7 years
Comparison of outcome one and 5–7 years after injury
Table 3 shows that three participants judged to be vegetative at one year died after a further one month, two years, and five years. Of those severely disabled at one year 44 (46%) died within 5–7 years. There was, however, little difference in mortality in those with moderate disability or good recovery at one year (30% v 28%). Among survivors assessed at 5–7 years, less than half (101 out of 219; 46%) remained in the same GOSE category as at one year. Sixty three (29%) had improved but 55 (25%) deteriorated.
Comparison of GOSE outcome between one and 5–7 years after injury (percentage change in brackets)
Most survivors who were disabled at a year remained disabled (89 out of 117, 76%) but 26/102 (25%) with a good recovery at one year had become disabled by 5–7 years. Six of the latter group were severely disabled: four had been diagnosed with deteriorating neurological conditions (one with Alzheimer’s disease, one with Lewy-Body dementia and psychosis, two with alcohol related dementia; respective ages at injury 76, 66, 51, and 71) and two with a psychiatric disorder (one of these was severely depressed and severely abused alcohol and the other had a severe undiagnosed depressive-like disorder). Diagnoses were provided by GPs when contacted during the 5–7 year follow up, with the exception of the patient who had the depressive-like disorder, who was discovered by the research worker.
Improvement occurred in 56 participants disabled at one year, 28 to a good recovery. These included seven who were severely disabled at one year, six of whom initially had a mild head injury.
Features relating to change in outcome between one and 5–7 years
Change in occurrence of a disabled outcome was characterised as either improvement from a category (GOSE) of moderate or severe disability at one year to good recovery at 5–7 years (that is, Disabled to Good, 28 of 117, 24%) or conversely worsening from good recovery at one year to disabled at 5–7 (Good to Disabled 26 of 102, 25%).
Improvement from Disabled to Good outcome was not strongly associated with age at injury (25% for participants aged ⩽40 v 22% for participants aged >40), sex (26% for males v 17% for females) severity of injury (26% for mild v 21% for moderate/severe), previous head injury (21% with v 18% without), other brain illness (18% with v 21% without). Likewise, deterioration from Good to Disabled outcome was not strongly associated with these “early” features (26% for participants aged ⩽40 v 25% for participants aged >40), sex (26% for males v 23% for females), severity of injury (28% for mild v 17% for moderate/severe), previous head injury (25% with v 26% without), other brain illness (22% with v 29% without). There were however, strong associations between cognitive and emotional factors assessed 5–7 years after injury and change in GOSE category between one and 5–7 years. This was investigated using separate t tests to compare Disabled at one and 5–7 years with Disabled at one year improving to Good at 5–7 years (see table 4). Improvement from Disabled to Good was strongly associated with lower self-ratings for depression, anxiety, and stress and with higher self-esteem.
Cognitive and emotional findings at 5–7 year follow up in participants who were disabled at one year
This group also had a significantly higher overall cognitive percentile score (p = 0.038), with significantly better speed of information processing and a trend towards better verbal memory. Alcohol use did not differ between these groups and drug abuse was rare.
Deterioration from Good to Disabled outcome was associated with high ratings for depression, anxiety, stress, and lower self-esteem (table 5). Mean values for these measures were similar to values in those disabled at both one and 5–7 years. Alcohol use was highest in the Good to Disabled group. In contrast, performance on cognitive tests did not differ significantly between those with a sustained good outcome and the group who had deteriorated from a Good to a Disabled outcome. Rating scores for emotional factors were similar in the Good-Disabled group and in those remaining persistently disabled.
Cognitive and emotional findings at 5–7 year follow up in participants who made a good recovery at one year
Rehabilitation and therapy services
Only 16 (7.3%) participants followed up at 5–7 years reported using any rehabilitation service or therapy when asked by free recall and given a checklist of possible options.
DISCUSSION
These findings in survivors assessed 5–7 years after admission to hospital after a head injury show that the overall rate of disability is very similar to that observed at one year. In the majority of participants, this reflected persistence of disability from the earlier assessment. Some participants who were disabled at 1 year had improved to a state of good recovery at 5–7 years but these were counterbalanced by a decline in outcome in some considered to have recovered well at one year. Death was associated with age and not with severity of injury. This is consistent with other studies that report a relatively small reduction in life expectancy if mobility is regained27 as expected in most people with head injury and as found in our cohort.
Most other studies on late outcome one and five years after injury have used a cross sectional design and consider improvement or decline within the cohort. Where comparisons have been made these have often been between specific, limited aspects, not “global” measures of outcome. An exception is the prospective study by Hammond et al5 where 301/927 people were followed up using the Disability Rating Scale (DRS) one and five years after a head injury. They report fewer people with change in disability (25% of cases) than found here (54%), with in particular fewer people becoming disabled (7%). Those successfully followed up by Hammond had higher levels of education and any differences in initial injury severity from those not followed up are not reported. The difference may reflect the more limited focus of the DRS which was introduced to track people through rehabilitation and is less sensitive to recovery of community and social status. Other studies3 with follow up at two and five years report more limited aspects of outcome, with a tendency at later follow up for overall improvement in independent living and use of transport, deterioration in employment status, but a higher incidence of emotional problems.
In the present study, the “biological factors” of the initial severity of head injury and age continued to show some relationship with outcome at 5–7 years. Other studies of outcome at five years after injury find age and/or severity of injury to be generally predictive of global outcome.5,7,28,29 However we found that the association between these variables at 5–7 years largely reflected their association with the distribution of outcome one year after injury. Thus, neither age nor initial severity of injury showed a clear association with deterioration or improvement in survivors between one and 5–7 years. Likewise, although there was an association between cognitive impairment and severe disability (either persisting or developing after one year), this association was not evident at these times for the occurrence of moderate disability.
In contrast to these findings, there was clear evidence of associations between adverse self-ratings of emotional wellbeing and moderate or severe disability. This applied both when disability had persisted and when it had developed between one and 5–7 years. The relatively low incidence of disability in terms of activities of daily living at 5–7 years further emphasises a relationship between emotional factors and global outcome. This study cannot determine to what extent emotional factors caused disability, or were a consequence of it. Nevertheless, the findings point at least to a potential for benefit from interventions appropriate to psychological factors, even several years after injury. A higher alcohol intake between one and 5–7 years was strongly associated with deterioration from good to disabled outcome. So few of the participants studied reported having received rehabilitation that there could be no meaningful analysis of the possible effect of this intervention. Clarification of this will require further study.
A unique strength of this study is that participants were drawn from a cohort that was recruited immediately after injury and was structured to represent the spectrum of head injured victims. This enabled investigation of prospectively collected information about features in the acute stage, at one year and at 5–7 years. The follow up rate at 5–7 years was very similar to that achieved at one year, and is high for the head injured population. Although the absence of information from 30% of potential participants calls for caution in extrapolating to community rates, the close similarity in the early and one year features of the participants assessed and those not available supports the view that disability may not be substantially less frequent in the latter. The structured approach to assessment and the very high interrater reliability between research workers at one and 5–7 years means that little of the change in disability found is attributable to inconsistency. The validity of the change in disability indicated by the GOSE is strongly supported by striking contrasts found in specific psychological assessments in participants whose disability status had changed.
Although there is a need for caution in extrapolating from these findings, they support the view of a high community burden from disability after head injury. Other studies emphasise the negative impact of psychosocial problems on people with brain injury and their relatives 5–7 years after injury.3 The evidence we found of an association between potentially remediable psychosocial factors and the extraordinary low access to rehabilitation point to the need to establish if there is benefit from systematic, coordinated services for the care and treatment of head injured victims.30
Since this cohort was first recruited, there has been a major investment in community services for head injury in Glasgow, and the evaluation of the benefit of this service should guide similar developments in other urban and in rural areas. Interventions that might alleviate late disability, either by promoting recovery or preventing or reversing deterioration need to be developed and evaluated. Further prospective, longitudinal studies need to identify what forms of intervention are associated with beneficial effects, but definitive, rigorous evidence will require prospective randomised comparisons, of which there are few to guide practice in this field.
In conclusion, admission to hospital, even after what was judged conventionally to be a minor head injury, is followed 5–7 years later by disability in a high proportion of survivors. Both persistence of disability and the development of new disability are associated strongly with psychosocial factors that may be open to remediation, even late after injury.
Acknowledgments
We thank Dr C Roy for his contribution to the development of the study. The study was funded by the Chief Scientist Office (CZH/4/48).
REFERENCES
Footnotes
-
Competing interests: none declared