Article Text

Abstract
Background: It is widely accepted that the passive dissemination of national clinical guidance has little or no impact on practice.
Objective: To assess the impact in England of an Effective Health Care bulletin on childhood surgery for glue ear issued in 1992 and to understand the reasons for any change (or lack of change) in practice that ensued.
Method: Time series analysis of the rate of use of surgery by children under 10 years of age from 1975 to 1997/8 in 13 English health districts.
Results: Following a rise in the rate of surgery in public (National Health Service) hospitals from 1975 to 1985, the rate declined by 1.6% a year from 1986 to 1992/3. Following publication of the guidelines in November 1992, the rate of decline increased to 10.1% a year. Even after allowing for a slight increase in the use of independent (private) hospitals between 1992/3 and 1997/8, the overall rate of decline was at least 7.9%. It appears that the rate of referral of cases by primary care physicians (general practitioners) halved during this period. Several contextual factors are thought to have contributed to the effect of the guidelines, including pre-existing professional concern about the value of surgery, the introduction of an internal market into the NHS, and growing apprehension among parents fuelled by scepticism in the mass media. During this unprecedented period of rapid change in usage, staff delivering the service remained unaware of the alterations in their own practice.
Conclusions: Passive dissemination of national guidelines can accelerate an existing trend in clinical practice if the context is hospitable. Policy makers should identify and target such situations.
- glue ear
- guidelines
- time series
Statistics from Altmetric.com
Several reviews have concluded that passive dissemination of guidelines has little or no effect on clinical practice.1–4 Nationally produced and disseminated guidelines, which take no account of the local context in which services are provided, have been found to be particularly ineffective. Despite this, governments in many industrialised countries are committed to such a policy.5,6 In England and Wales the Department of Health has funded the NHS Centre for Reviews and Dissemination to produce Effective Health Care bulletins and disseminate them to decision makers since 1992.7 One of the first, in November 1992, was on the treatment of glue ear (persistent otitis media with effusion (OME)) in children.8 This was accompanied by summaries and editorials in several leading medical journals.9,10
Surgery for glue ear had, by the late 1970s, become the most common reason for childhood surgery in England and Wales and, in some areas, the most common reason for admission of children to hospital.11 By the mid 1980s there was increasing concern about the wisdom and appropriateness of such high levels of use of surgical interventions to treat the disorder. It was not therefore surprising that these operations were the focus of one of the earliest Effective Health Care bulletins produced. The bulletin reviewed the research evidence available at the time and recognised the benefits of surgery for children with severe glue ear, but cautioned against overuse of surgery in children with milder forms of the condition which might resolve without any intervention. The implicit expectation was that the widespread dissemination of such advice would result in a reduction in the rate of surgery.
By 1992, however, the rate of surgery was already falling,12 although this was not widely recognised at the time. The epidemic had peaked in the mid 1980s and fallen steadily over the following years. So, for the guidelines to be effective, it would be necessary to show an acceleration in the decline.
The primary aim of this paper is to ascertain whether or not the passive dissemination of national guidelines to typical service providers (district general hospitals as well as teaching hospitals) had any impact on clinical practice. Studies of such interventions in other areas have reported either no clinically significant effect13–16 or only a modest impact.17 If the guidelines were shown to have had an effect on this occasion, our secondary aim was to establish why this was so.
METHODS
Annual numbers of surgical operations for glue ear performed in NHS hospitals for residents of 13 health districts (as defined in 1975) in the Oxford and East Anglian health regions had previously been obtained for 1975 to 1990/1.11 Data had come from the Hospital Activity Analysis (HAA) system up until 1986 and then from the District Information System. Data for 1991/2 to 1997/8 were obtained from Hospital Episode Statistics supplied by the Department of Health. Population denominator data were obtained from the Office for National Statistics. To ensure consistency in the resident populations being studied over the 23 years, more recent data were mapped onto the geographical areas defined in 1975 by means of patients' postcodes.
Cases were included if they were aged under 10 years and had undergone myringotomy or tympanostomy tube insertion, with or without adenoidectomy, and with or without tonsillectomy. From 1975 to 1987/8 procedures were coded according to the OPCS 3rd revision (193.1–193.4; 193.1–193.4 with 235; 193.1–193.4 with 233) and from 1988/9 the OPCS 4th revision (D15.1–15.4, 15.8, 15.9; D15.1–15.4, 15.8, 15.9 with E20; D15.1–15.4, 15.8, 15.9 with E20 and F34). Care was taken to avoid double counting when surgery was bilateral. Adjustments were made for shortfalls in the clinical coding in otolaryngology, which never exceeded a few percent in any year. It was assumed that failure to code procedures was not influenced by the procedure carried out. Intervention rates for surgery for OME were therefore adjusted according to the overall shortfall for the specialty.
For each year and health district the rate of surgery per 10 000 children aged 0–9 years was calculated. The change in rates from 1986 to 1997/8 was analysed using a Poisson regression model with robust standard errors to allow for overdispersion.18 An interaction term for the years from 1992/3 to 1997/8 was used to examine whether the change in surgery rates following publication of the Effective Health Care bulletin (November 1992) differed from the change in the preceding years. For each time period the annual change in surgery rates and its 95% confidence interval was calculated.
Estimates of the number of operations performed in independent hospitals on children aged 0–14 years resident in the Oxford and East Anglian regions in 1992/3 and in the Anglia and Oxford region in 1997/8 were obtained.19,20 From these, the number of operations performed on residents of the 13 districts in this study was calculated.
RESULTS
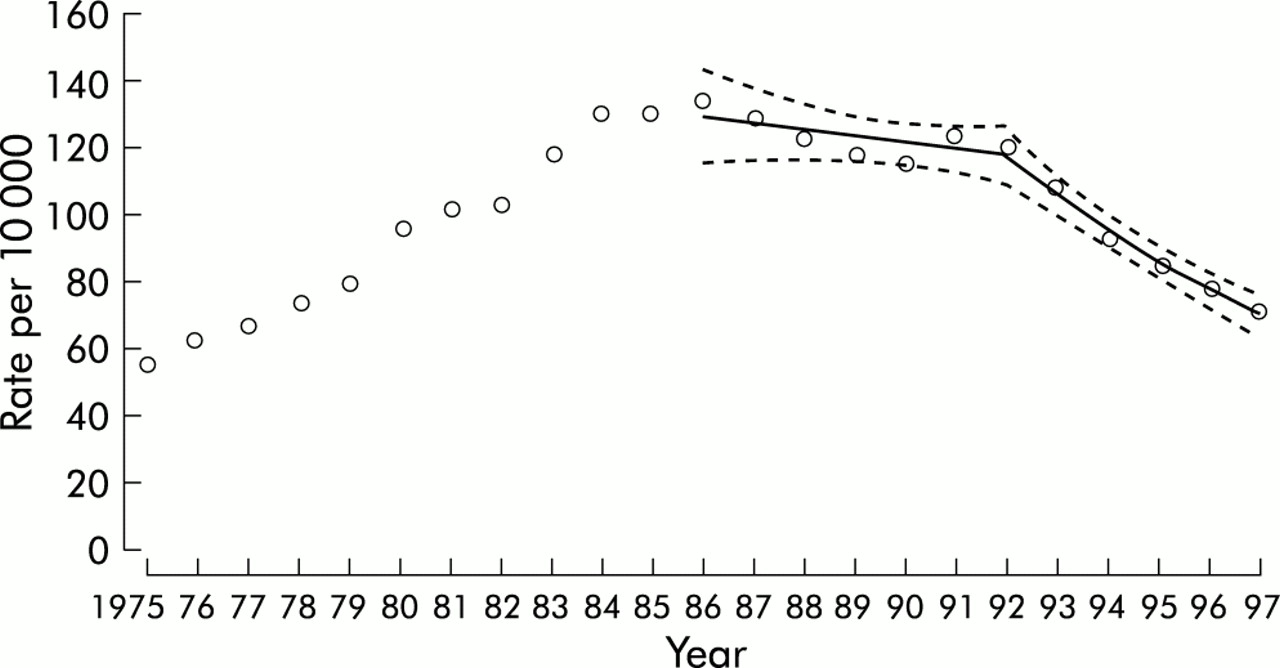
The overall rate of surgery in children aged under 10 years increased from 1975 reaching a peak in 1986 with a rate of 132 per 10 000 (table 1, fig 1). Rates in the 13 health districts ranged from 69 to 230 per 10 000 in 1986. The overall rate subsequently declined, falling to 120 per 10 000 by 1992/3 (range 91–165). The mean annual decline was –1.6% (95% confidence interval (CI) –3.9% to 0.8%). For individual districts the mean annual change ranged from a decrease of 5.0% to an increase of 9.2%. Between 1992/3 and 1997/8 the rate of decline in surgery increased so that, by 1997/8, the overall rate was 68 per 10 000 (district range 45–90). The mean annual decline was –10.1% (95% CI –7.9% to –12.3%). Rates declined in all districts with mean annual declines ranging from 5.0% to 14.2%. The decline during this period was significantly greater than in the preceding period (1986–1992/3): ratio of mean annual change in rates = 0.91 (95% CI 0.88 to 0.95).
Glue ear surgery rates in children aged under 10 years in East Anglian and Oxford regions and interdistrict range (1975 to 1997/8)

{kind=link}
Rates per 10 000 of glue ear surgery in children aged under 10 years in the Anglia and Oxford regions showing fitted Poisson regression line and 95% confidence limits. Years 1975–86 are calendar years; years 1987 onwards are the 12 months from 1 April to 31 March the following year.
To determine the impact of any change in the rate of surgery in independent hospitals, the total rate (NHS plus independent hospitals) in 1992/3 (138 per 10 000) was compared with 1997/8 (91 per 10 000). This reduced the observed mean annual decline from 10.1% to 7.9%, still significantly greater than the 1.6% annual declines which occurred before 1992/3.
DISCUSSION
The modest but steady decline in the rate of surgery for glue ear which started in the mid 1980s accelerated after 1992. Between 1992/3 and 1997/8 the rate in NHS hospitals almost halved, although there was considerable variation between the 13 districts that constituted the study population. If these changes resulted even partly from the dissemination of national guidelines in November 1992, this is in sharp contrast to previous reports from the USA,14,15 Canada,13 and the UK16,17 which found little or no effect of such an intervention. Before discussing why, on this occasion, passive dissemination of national guidelines may have been so effective, it is necessary to consider other possible explanations for the decline in the rate of surgery—namely, statistical artefacts, supply factors, and demand factors.
The observed changes in the surgical rate might have been due to statistical artefacts. This is unlikely as there were few missing data (and adequate adjustments were made when data were absent). Although management of routine data on hospital use changed twice during the 23 years, the method of data collection remained the same. We have no reason to believe that the validity of the data recording and coding declined systematically over the time period studied. One other possible artefact would be a rise in the rate of surgery in independent hospitals (privately funded cases performed in NHS hospitals were included in the data analysed). While the rate did rise in independent hospitals from 18 to 22 per 10 000, this was insufficient to cancel the significant overall decline in the use of surgery during this period.
If the observed decline in surgical rate has been real (rather than apparent), it could have arisen as a result of a reduction in the supply of services, either through a decrease in available services (otolaryngologists, hospital beds, operating theatre time) or through a change in clinicians' judgement as to the appropriate indications for surgery. With regard to the former, far from a reduction in the availability of services, the 1990s witnessed an annual 4% increase in the number of hospital consultants.21 With regard to clinician judgement, no quantitative data exist on changes in the severity of surgical cases over time. It is therefore possible that clinicians became increasingly restrictive in their advocacy and use of surgery for treating glue ear, in particular by more appropriate use of investigations and watchful waiting as suggested in the Effective Health Care bulletin.
A decrease in the use of surgery could also have resulted from a reduction in demand—fewer parents approaching their GPs who, in turn, may have been less inclined to refer children to an otolaryngologist. There are no national routine data on referral rates, although researchers carrying out a randomised trial during this period have reported a 50% decline in the number of children referred to the 13 hospitals included in that study between 1994 and 1998 (Mark Haggard, personal communication). These three factors may therefore have contributed to the accelerated decline in the use of surgery which began in 1992/3: a reduced demand from parents, a fall in the GP referral rate to otolaryngologists, and the adoption of more stringent indications for surgery by surgeons.
It seems reasonable to believe that this dampening down both of demand and of supply which started in the year following publication of the Effective Health Care bulletin was related, at least in part, to that intervention. However, GPs, otolaryngologists, and other relevant staff (audiologists, health visitors, school nurses) did not share this view when interviewed in 1996–8.22 In a qualitative study carried out in the same geographical area as the present study, researchers concluded that “the Effective Health Care bulletin has not proved to be particularly helpful for our group of interviewees in clarifying appropriate practice”. Most had not heard of it, and those who had claimed it had had little or no influence on their practice. On the basis of their respondents' opinions, the authors concluded that “our findings in this case study suggest that we cannot expect guidelines such as the Effective Health Care bulletin alone to lead to change in clinical behaviour”. Interestingly, the respondents seemed unaware that a significant change in clinical behaviour had been going on for at least three years.
What other factors might have contributed to the dramatic decline in surgery following the dissemination of the bulletin? One major organisational change to the NHS could have contributed—namely, the introduction of GP fund holding. This was implemented in annual waves; the first wave of pioneering GPs was in April 1991 with successive waves each April. Although they were only a minority of GPs over the first few years (1990/1 to 1994/5), some evidence suggests their patients made less use of minor discretionary surgery.23 Fund holding could therefore have contributed independently to the observed changes, although it offers only a partial explanation and the bulletin may have contributed to fund holders' behaviour.
The other factor that needs to be considered is the impact that adverse publicity about the effectiveness of surgery for glue ear might have had on the public and, in particular, on parental views. Even before the launch of the bulletin, the mass media had been interested in the topic.24 Public awareness was heightened when glue ear surgery became a high profile issue in the British General Election in spring 1992.25,26 Following publication of the bulletin later that year, newspapers and television reported that doubt had been thrown on the value of the operation.27,28 Media interest was further stimulated a few months later29 when an Audit Commission report on hospital services for children concluded that “too many children are being operated upon for glue ear”.30
All this adverse publicity may well have affected parents and GPs, making them more reluctant to seek a surgical answer. This was certainly the view of one medical commentator31 and, by 1995, these views were also affecting the formal purchasers of health care—the district health authorities. A survey of annual purchasing plans revealed that 23 of 129 health authorities were limiting their support for surgery for glue ear32 or even attempting a complete ban.33
Given the apparent lack of impact of the passive dissemination of national guidance reported previously, why was the publication of this particular bulletin associated with such a dramatic change in practice? We suggest that five contextual features contributed:
-
The key staff being targeted—the otolaryngologists—were already questioning the appropriateness of surgery and some had been concerned for some time about its occasional unnecessary use.
Key messages
-
The rate of surgery for glue ear in England declined dramatically during the 1990s, halving between 1992/3 and 1997/8.
-
Following publication and dissemination of national guidelines in November 1992, the rate of decline increased from 1.6% a year to 7.9%.
-
Several contextual factors probably contributed: pre-existing professional concern about the value of surgery, the introduction of an internal market into the NHS, and growing apprehension among patients fuelled by scepticism in the mass media.
-
Despite the dramatic fall in the rate of surgery, staff delivering the service remained unaware that such a change was taking place.
-
-
The rate of surgery had already peaked and started to decline. By the time the bulletin appeared, the rate had been falling for about 5 years, so the bulletin only had to accelerate a trend, not start or even reverse one.
-
Unlike most hospital services, surgery for glue ear was heavily dependent on the discretion and judgement of GPs who acted as key gate keepers to the operation. Widespread scepticism about the value of surgery was well established among GPs so that, when the bulletin appeared, many felt more confident about delaying referral to a surgeon and, instead, waiting to see if the condition would resolve without intervention.34
-
Concurrent structural changes to the NHS encouraged the use of more stringent clinical criteria before treatments were approved. GP fund holding provided general practices with a financial incentive to try to avoid surgery, while the separation of purchasing from providing raised awareness about the costs of interventions. District health authorities, in their new role as purchasers, sought budgetary savings. Obvious targets were interventions of uncertain effectiveness, the withholding of which was likely to pose little or no risk to the health of subjects, and interventions which had no effective organised lay group to lobby on behalf of sufferers. Surgery for glue ear was just such a “soft target”.
-
The growing apprehension among parents of the benefits of surgery, encouraged by media scepticism. In this respect there were parallels with the decline in the 1950s and 1960s of tonsillectomy, to which public concern and doubt are thought to have contributed.
It is impossible to assess the relative impact contributed by each of these five factors but, given the apparent lack of awareness of the contents of the bulletin among healthcare professionals, one might speculate that changes in the attitudes and behaviour of parents played a key role. In turn, such changes are likely to have been influenced significantly by mass media reports.
Our findings of a dramatic alteration in the speed of change in the use of surgery suggests that passive dissemination of national guidance can contribute to change in clinical practice if the context is appropriate. This implies that bodies responsible for producing voluntary guidelines should focus on those topics for which the environment is likely to be conducive to change. A preliminary analysis of the context might help to avoid expending effort in areas where change is unlikely in the situation that pertains.
Acknowledgments
The authors thank the Department of Health for supplying data from the Hospital Episode Statistics, Brian Williams for data on independent hospitals, Chris Grundy for post code matching, and Colin Sanderson and Jan van der Meulen for statistical advice.
REFERENCES
Linked Articles
- Action points