Accuracy of UK Rapid Test Consortium (UK-RTC) “AbC-19 Rapid Test” for detection of previous SARS-CoV-2 infection in key workers: test accuracy study
BMJ 2020; 371 doi: https://doi.org/10.1136/bmj.m4262 (Published 11 November 2020) Cite this as: BMJ 2020;371:m4262Read our latest coverage of the coronavirus outbreak
Linked Editorial
Testing for antibodies to SARS-CoV-2

- Ranya Mulchandani, Field Epidemiology Training Programme (UK-FETP) fellow1*,
- Hayley E Jones, senior lecturer2*,
- Sian Taylor-Phillips, professor3,
- Justin Shute, biomedical scientist1,
- Keith Perry, clinical scientist1,
- Shabnam Jamarani, technical manager1,
- Tim Brooks, consultant microbiologist1,
- Andre Charlett, head of statistics and modelling1,
- Matthew Hickman, professor2,
- Isabel Oliver, director of National Infection Service1,
- Stephen Kaptoge, principal research associate4,
- John Danesh, professor4,
- Emanuele Di Angelantonio, professor4,
- Anthony E Ades, professor2,
- David H Wyllie, consultant microbiologist1
- on behalf of the EDSAB-HOME and COMPARE Investigators
- 1Public Health England, London, UK
- 2University of Bristol, Bristol, UK
- 3University of Warwick, Coventry, UK
- 4University of Cambridge, Cambridge, UK
- *Contributed equally
- Correspondence to: D Wyllie David.wyllie{at}phe.gov.uk (or @davidwyllie20 on Twitter)
- Accepted 2 November 2020
Abstract
Objective To assess the accuracy of the AbC-19 Rapid Test lateral flow immunoassay for the detection of previous severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection.
Design Test accuracy study.
Setting Laboratory based evaluation.
Participants 2847 key workers (healthcare staff, fire and rescue officers, and police officers) in England in June 2020 (268 with a previous polymerase chain reaction (PCR) positive result (median 63 days previously), 2579 with unknown previous infection status); and 1995 pre-pandemic blood donors.
Main outcome measures AbC-19 sensitivity and specificity, estimated using known negative (pre-pandemic) and known positive (PCR confirmed) samples as reference standards and secondly using the Roche Elecsys anti-nucleoprotein assay, a highly sensitive laboratory immunoassay, as a reference standard in samples from key workers.
Results Test result bands were often weak, with positive/negative discordance by three trained laboratory staff for 3.9% of devices. Using consensus readings, for known positive and negative samples sensitivity was 92.5% (95% confidence interval 88.8% to 95.1%) and specificity was 97.9% (97.2% to 98.4%). Using an immunoassay reference standard, sensitivity was 94.2% (90.7% to 96.5%) among PCR confirmed cases but 84.7% (80.6% to 88.1%) among other people with antibodies. This is consistent with AbC-19 being more sensitive when antibody concentrations are higher, as people with PCR confirmation tended to have more severe disease whereas only 62% (218/354) of seropositive participants had had symptoms. If 1 million key workers were tested with AbC-19 and 10% had actually been previously infected, 84 700 true positive and 18 900 false positive results would be projected. The probability that a positive result was correct would be 81.7% (76.8% to 85.8%).
Conclusions AbC-19 sensitivity was lower among unselected populations than among PCR confirmed cases of SARS-CoV-2, highlighting the scope for overestimation of assay performance in studies involving only PCR confirmed cases, owing to “spectrum bias.” Assuming that 10% of the tested population have had SARS-CoV-2 infection, around one in five key workers testing positive with AbC-19 would be false positives.
Study registration ISRCTN 56609224.
Introduction
After infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), most, but not all, infected people generate antibodies against the viral spike (S) or nucleoprotein (N) antigen.12 Several lateral flow immunoassays (LFIAs)—small, pregnancy test format devices that can deliver testing rapidly and at scale—have recently become available that detect antibodies against SARS-CoV-2 proteins. These devices have two potential main uses: population serosurveillance and assessment of individual risk of developing immunity to coronavirus disease 2019 (covid-19).345 The US Food and Drug Administration recently (24 September 2020) licensed an LFIA for office use (that is, in supervised environments), on the basis that it may predict immunity (https://www.fda.gov/media/139789/download); if this is validated, then it could result in widespread use of this class of devices. However, this application is also critically dependent on high test accuracy: if assay specificity is not sufficiently high, false positive results could result in non-immune people being assigned to high SARS-CoV-2 exposure environments.67
Evaluations of different LFIAs for SARS-CoV-2 have produced widely varying estimates of accuracy.28 In some jurisdictions, large numbers of devices are available, with varying levels of performance characterisation.9 In a recent Cochrane review,2 most LFIA evaluations were considered to be at high risk of bias, owing to use of a “two gate” (also known as “diagnostic case-control”) design.10 These studies evaluate LFIAs on a set of pre-pandemic blood samples and on a separate set of convalescent samples taken from cases of SARS-CoV-2 confirmed by polymerase chain reaction (PCR). This study design has been associated with overestimation of test accuracy on average across multiple clinical settings,1011 referred to as “spectrum bias.”12 The sensitivity of SARS-CoV-2 antibody tests based on PCR confirmed cases could be overestimated if people with more severe disease are more likely to have been PCR tested than those with milder illness, and if, as is known to occur,131415 people with more severe illness produce higher antibody concentrations. This tendency would make confirmed cases easier to diagnose than cases in other people who, although previously infected, were not PCR tested. Despite the importance of obtaining real world estimates of test accuracy, however, potential spectrum bias has not been assessed to date in SARS-CoV-2 antibody testing. This is partly due to the need for larger sample sizes in the alternative approach of assessing test accuracy directly in a target cohort (a so-called “one gate” design) and partly due to the lack of a true gold standard test to assess previous infection in such a cohort.
This study helps to reduce uncertainties in the evaluation of a new SARS-CoV-2 rapid antibody test, the “AbC-19 Rapid Test” (AbC-19 hereafter). Produced by the UK Rapid Test Consortium (UK-RTC), the test contains trimeric SARS-CoV-2 S protein attached to a membrane, which, when recognised by IgG antibodies, results in formation of a band visible to the user. Professional use CE marking has been obtained by self-certification. The PANDEMIC study from Ulster University, which is not yet peer reviewed, reports sensitivity of 97.7% (n=304; 95% confidence interval 95.7% to 99.3%) and specificity of 100% (n=350; 95% confidence interval reported as 100% to 100%) to detect presence of antibodies.16 This suggests that the AbC-19 test gives no false positive results. However, these may be overestimates of test accuracy, as blood samples from a number of people were excluded from this test evaluation on the basis of results of other tests (pre-selection). We evaluated AbC-19 in the detection of previous infection with SARS-CoV-2 by using venous blood samples collected from UK key workers in the EDSAB-HOME (Evaluating Detection of SARS-CoV-2 AntiBodies at HOME) study15 and pre-pandemic samples from blood donors.
Methods
Study participants
In total, across the two parts of the study, we analysed blood samples from 4842 people: 2847 people recruited through the EDSAB-HOME study,15 and an additional 1995 pre-pandemic samples from the COMPARE blood donor study. Each sample was from a separate individual.
EDSAB-HOME study: recruitment
EDSAB-HOME is a study of key workers in the UK (ISRCTN 56609224).15 People were eligible to enrol in the study if they were currently working at their place of work, aged 18 years or over, and able to read English and had an in-use personal email address and mobile phone number. Anyone who was currently experiencing covid-19 compatible symptoms, had experienced any such symptoms in the previous seven days, met the government’s criteria for “exceptionally vulnerable,” was unable to read normal sized print, or was taking part in any covid-19 vaccine trials was not eligible for enrolment. Symptom history was not part of the eligibility criteria. All data and samples were collected in June 2020 and form a convenience sample. The purpose of the study was to assess the accuracy of LFIAs suitable for deployment at scale in key workers in the UK. All participants completed an online questionnaire, which included information on any previous tests they had had for SARS-CoV-2, their beliefs about whether they had had covid-19, and any signs and symptoms that they or their household members had experienced since 1 January 2020. On the basis of this information, we categorised participants by using a version of the World Health Organization’s criteria for confirmed, suspected, and probable cases, adapted to the UK context and taking into account the confirmation of community transmission on 5 March 2020 (supplementary material, table S1).15 Previous PCR status was self-reported and validated by comparison with national laboratory records after recruitment. Recruitment into the study was through three streams: fire and police officers (stream A), healthcare workers who were recruited without any restrictions on previous PCR status (stream B), and healthcare workers recruited only if they had a history of SARS-CoV-2 PCR positivity (stream C) (fig 1). On attending a study clinic, each participant had a venous blood sample taken, which was anticoagulated using EDTA. In participants with previous PCR positivity, onset of illness occurred a median of 63 (interquartile range 52-75) days before the clinic visit. Plasma was separated by centrifugation and stored at −80°C until use. No samples were frozen and thawed more than five times. Demographic details are in the supplementary materials (table S2), as is additional information on the relation between PCR testing and symptoms.
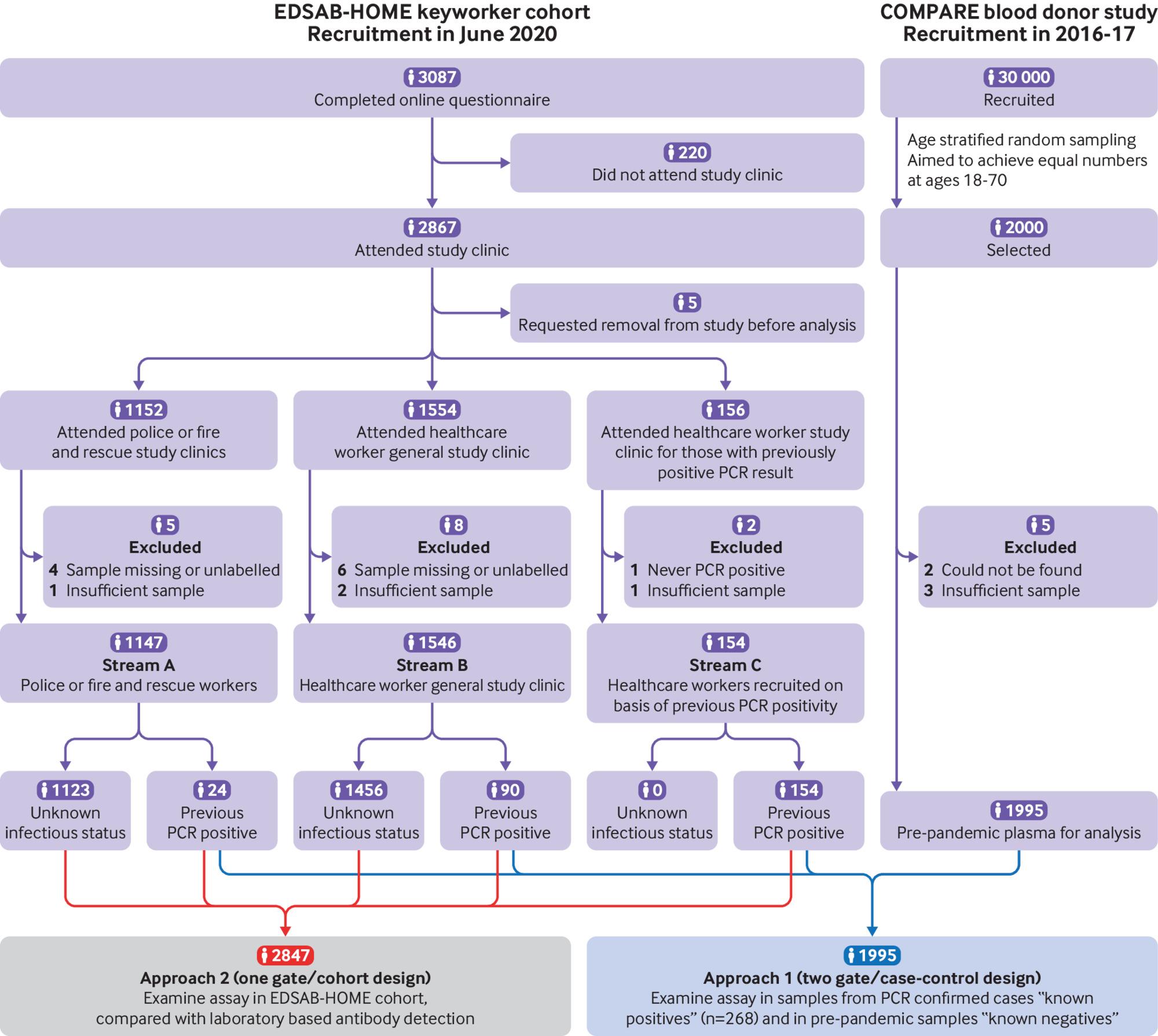
Flow diagram of recruitment and analysis. PCR=polymerase chain reaction
{kind=link}
COMPARE study
We used stratification by age, sex, and region to randomly select 2000 participants as “known negative” samples from among a pool of almost 29 029 participants recruited into the COMPARE study, a pre-pandemic (2016-17) blood donor cohort in England (ISRCTN 90871183). Of these participants, 1995 had samples available for analysis (fig 1). The selection strategy aimed to maximise national geographical representativeness of the sample, with approximately equal numbers of people across participating age groups (18-70 years). Demographic details are in the supplementary materials (table S3).
Approach 1: PCR positive cases and pre-pandemic samples as reference standard
We used two approaches to estimate the accuracy of AbC-19, both pre-specified (fig 1). In approach 1, we estimated the sensitivity and specificity of AbC-19 by using two sets of samples with known previous infection status: pre-pandemic samples (“known negatives”) from the COMPARE study (n=1995) and samples collected from participants in EDSAB-HOME who self-reported having had a previous PCR positive test for SARS-CoV-2 (“known positives”) (n=268).
Approach 2: Laboratory immunoassays as reference standard
When the EDSAB-HOME protocol was written, large scale development and evaluation of SARS-CoV-2 immunoassays was an emerging field. We pre-specified the use of a laboratory reference standard indicative of previous SARS-CoV-2 infection as a single assay with the highest published accuracy available to us after sample collection; as anticipated in the protocol, this was the Roche Elecsys assay, which measures antibodies against the N protein.17 We also analysed all samples with the EUROIMMUN anti-S IgG immunoassay, which detects antibodies against the S protein S1 domain, one domain present in the AbC-19 test antigen. We repeated immunoassays that failed for technical reasons, in accordance with usual clinical practice, and excluded samples with insufficient volume for testing from analyses. Although the primary reference standard used here is the Roche Elecsys immunoassay (threshold 1.0), having previously noted the strong positive correlation between Roche Elecsys and EUROIMMUN assay results (ρ=0.9315), in sensitivity analyses we also used a EUROIMMUN immunoassay (threshold 0.8, as described15) and a composite reference standard defined as positive on either Roche Elecsys or EUROIMMUN versus negative on both. We made these comparisons separately for the known positive (n=268) and all other EDSAB-HOME samples (n=2579), to assess for potential spectrum bias associated with estimating test sensitivity from PCR confirmed cases relative to other people with evidence of previous infection. We refer to the latter sample set (n=2579) as samples from people with unknown previous infection status. We analysed samples from 2847 EDSAB-HOME study participants (fig 1), a group comprised of police, fire, and healthcare staff who are of working age and worked throughout lockdown.15
Laboratory protocol
Test evaluation (product FG-FD51919, lot A2007003) was performed in an accredited WHO Pre-Qualification Evaluating Laboratory based in PHE Colindale, London, by experienced laboratory staff following training by the manufacturer. Trained staff dropped 2.5 μL of plasma into the lateral flow device followed by 100 μL of chase buffer; devices give a qualitative (positive or negative) result for presence of IgG antibodies and include a control band. A result was considered positive if two bands were present and negative if only the control band was present. Devices in which a control band did not develop were considered to have given invalid results (n=5) and were repeated. Three readers independently read each device using the WHO scoring system for subjectively read assays (0=negative; 1=very weak, but definitely reactive; 2=medium to strong reactivity).18 For assessment of test sensitivity and specificity, and in measuring discordance in AbC-19 positivity across the multiple readers, scores of 1 and 2 were grouped together as “positive.” If the three independent readers disagreed on the positivity of a sample, the majority reading was taken as the “overall” or consensus test result in our primary analysis, as per the WHO protocol.18
None of the staff who ran the laboratory immunoassays had access to any clinical information on the samples, and laboratory immunoassays were all completed before any testing of the index test. For all EDSAB-HOME samples and the first 350 pre-pandemic samples analysed, readers were blind to the reference standard (including randomising order of known positives and negatives), as well as to any information on study participants or results on other assays. The additional 1650 pre-pandemic samples were analysed after the other samples, for which complete blinding was difficult. We retested known negative samples if they tested positive on the AbC-19 device. For all other samples, we retested if the result was different from the composite reference standard defined above. Our primary results are those based on the initial set of readings for each sample. Results following retesting are reported as secondary, as only discordant samples were retested, which does not reflect how the test would be used in the real world. More details are in the supplementary materials.
Statistical analysis
We estimated 95% confidence intervals around proportions by using Wilson’s method in R 3.5.1. In approach 1, we estimated AbC-19 test sensitivity and specificity as the proportion of known positive samples that tested positive and the proportion of known negative samples that tested negative, respectively. Estimates of sensitivity are also presented by days since onset of symptoms and separately for people who reported no symptoms. Test specificity estimates are further reported by age group.
In approach 2, AbC-19 test sensitivity and specificity are reported for each of the immunoassay reference standards described above. AbC-19 test results are also stratified by adapted WHO categorisation. To facilitate evaluation of potential spectrum bias associated with estimating test sensitivity from PCR confirmed cases, we stratified approach 2 estimates by whether participants were known to have had PCR confirmed SARS-CoV-2 infection (known positive sample set: n=268) or whether their previous infection status was unknown before antibody testing (n=2579). However, to reflect the “one gate” nature of EDSAB-HOME streams A and B, we also report as a secondary analysis results from all stream A and B participants, regardless of previous PCR positivity (n=2693).
Additional post hoc analyses assessed the association between age, sex, and ethnicity and specificity, using multivariable logistic regression; anti-S1 antibody indexes (EUROIMMUN) and AbC-19 test sensitivity; and the level of disagreement between three independent reviewers. These analyses are described in the supplementary materials.
Sample size calculations
Study size was based on sample size calculations done as part of the EDSAB-HOME research protocol (see supplementary materials).
Positive and negative predictive values
We calculated positive and negative predictive values for prevalence of previous infection of 5%, 10%, 15%, 20%, and 25% as functions of estimated sensitivity and specificity. We calculated 95% confidence intervals by using a simulations based approach in R, accounting for the sampling variation (uncertainty) in both estimates. We used the estimates of specificity based on pre-pandemic sera (known negatives). We present two sets of estimates of positive predictive value and negative predictive value based on alternative estimates of test sensitivity: sensitivity based on analysis of PCR confirmed cases and sensitivity based on comparison with the primary (Roche) immunoassay reference standard in people with unknown previous infection status.
Accounting for multiple readers
For each sample set (known positives, known negatives, and unknown previous infection status), we report numbers of disagreements between the three independent reviewers. In the presence of discordant results across readers, we anticipated that estimating test sensitivity and specificity based on the majority reading would lead to a slight upward bias in these estimates. To explore the potential extent of this, within approach 1 we did additional analyses in which each reading was treated as a separate “test.” We fitted multinomial distributions to tables of cross classified readings, assuming a log-linear model for underlying probabilities. Full details are available in the supplementary materials.
Patient and public involvement
As part of the EDSAB-HOME study design, patient and public involvement was provided by a public panel run through NIHR Birmingham Biomedical Research Centre and NIHR Applied Research Collaboration West Midlands. The panel commented on study design, acceptability, and strategies for effective recruitment. The questionnaire, communications with the participants, and all public facing documentation were informed and refined by this engagement. We did not seek public engagement in the design of the laboratory aspects of the study or in the interpretation of the results.
Results
Approach 1: sensitivity and specificity in “known positives” and “known negatives”
In 1995 pre-pandemic known negative samples from the COMPARE study, test specificity was 97.9% (95% confidence interval 97.2% to 98.4%) (table 1). Specificity was slightly lower in women (96.9%, 95.6% to 97.8%) than in men (98.9%, 98.0% to 99.4%) (adjusted odds ratio favouring false positivity in women 2.9, 95% confidence interval 1.5 to 5.9). After retesting of discordant samples, a female excess was still evident (adjusted odds ratio 4.7, 1.4 to 17) (table S4).
Approach 1: specificity of AbC-19 Rapid Test estimated from 1995 pre-pandemic samples (“known negatives”)
Among 268 (9.4%) EDSAB-HOME participants who had had a positive PCR test for SARS-CoV-2, test sensitivity was 92.5% (88.8% to 95.1%) (table 2). In this group, the first positive PCR test had occurred a median of 59 days previously. Days since first positive test was 21 or more in 251/268 cases. Sensitivity was estimated to be substantially lower among the 12 participants who reported no symptoms (sensitivity 58.3%, 32.0% to 80.7%) than among the 256 who reported symptoms (sensitivity 94.1%, 90.6% to 96.4%), and may decline slightly in PCR positive people with longer times between symptoms and blood sampling (table 2; figure S1).
Approach 1: sensitivity of AbC-19 Rapid Test based on samples from 268 people with previous positive polymerase chain reaction test (“WHO confirmed” category: “known positives”)
False negative AbC-19 tests occurred predominantly in samples with lower EUROIMMUN anti-S indices (fig 2, A; figure S1). Three participants (all asymptomatic) had clear negative results on both immunoassays in addition to the AbC-19 device.

Relation between AbC-19 test results and immunoassay indices. A: AbC-19 Rapid Test results by EUROIMMUN and Roche Elecsys assay titre, showing whether participant was asymptomatic, among 268 “known positives” (approach 1). B: AbC-19 results by EUROIMMUN and Roche Elecsys titre among all 2579 “unknown previous infection status” EDSAB-HOME stream A and B participants (ie, all study participants except cases confirmed by polymerase chain reaction) (approach 2). Lines reflect Roche threshold (1.0) and EUROIMMUN rule-out (0.8) and rule-in (1.1) thresholds recommended by manufacturers. 0.8 threshold was used for EUROIMMUN in this study
{kind=link}
Approach 2: analysis of “unknown previous infection status” EDSAB-HOME study samples
In EDSAB-HOME participants with unknown previous infection status (all those who had not had a positive PCR test; fig 2, B), antibody indices from anti-N and anti-S assays were highly correlated (Spearman’s ρ=0.93; P<0.001). We observed clear delineation between two main clusters of participants (with versus without antibodies), whereas the true previous infection status of a small minority of samples is less clear.
Among participants with unknown previous infection status testing positive on the Roche reference standard, 62% (218/354) reported symptoms compatible with covid-19 since 1 January 2020. The remaining 136 included 55 (16%) people who reported no compatible symptoms and 81 (23%) who “did not know” whether they had had any compatible symptoms.
Table 3 shows estimates of sensitivity and specificity of the AbC-19 test based on comparison with the three immunoassay reference standards, across all EDSAB-HOME study participants. Among the unknown previous infection status samples, sensitivity was 84.7% (80.6% to 88.1%) and specificity was 98.9% (98.4% to 99.3%) on the basis of the Roche reference standard (table 3). This was lower than sensitivity among the PCR confirmed cases, which was estimated as 94.2% (90.7% to 96.5%) on the basis of the same reference standard. In sensitivity analyses, we observed a similar pattern on the basis of the EUROIMMUN reference standard and a composite of the two assays (table 3). This is expected given the strong positive correlations between the immunoassay results studied (fig 2).
Approach 2: AbC-19 results on all EDSAB-HOME samples, compared with immunoassay reference standards
Retesting discordant samples did not substantially alter these estimates (table S4). Test accuracy estimates did not vary across recruitment stream A or B (tables S5 and S6). Based on comparison of test results in all EDSAB-HOME stream A and B samples with the Roche reference standard, regardless of previous PCR positivity (one gate estimate), AbC-19 test sensitivity was estimated as 86.6% (83.2% to 89.4%) (table S7).
Between reader variation
With the AbC-19 device, many bands were weak visually; for example, among the 462 samples from streams A and B that tested positive with the Roche reference standard, consensus scoring found that 62 (13%) had no visible band, 199 (43%) had a band scored 1, and 201 (44%) had a band scored 2. Expert readers differed in rating the device as positive or negative in 189/4842 (3.9%) devices, requiring a consensus decision (table S8). A log-linear regression model fitted to the known positives and known negatives estimated the sensitivity and specificity of an individual reader reading the device as 91.4% (95% credible interval 88.2% to 93.9%) and 97.6% (97.0% to 98.1%), respectively (supplementary material, table S8). These point estimates are lower than the estimates derived when using the consensus approach used in WHO evaluations with sensitivity and specificity of 92.5% (88.8% to 95.1%) and 97.9% (97.2% to 98.4%) (table 1 and table 2).
Different test sensitivity in PCR positive versus immunoassay positive samples
Among participants from streams A and B with immunoassay positive results, we investigated why AbC-19 test sensitivity in people who had not had a previous positive PCR test was less than in those who had had confirmation by PCR. As the AbC-19 test detects anti-S antibody, we compared results with anti-S antibody indices obtained using the EUROIMMUN immunoassay. PCR positive participants had higher anti-S antibody titres (median 4.14 v 5.63 units; P=0.001; fig 3, A). As the AbC-19 test band strength observed by the three observers increases, so too does the anti-S antibody index detected by EUROIMMUN immunoassays, showing that band strength is proportional to antibody concentrations (fig 3, B). Importantly, at low antibody concentrations, corresponding to EUROIMMUN indices of less than 3, the AbC-19 test is insensitive (fig 4). However, such low concentrations are common: 84/263 (32%) participants who had previously been PCR positive had anti-S antibody indexes less than 3, compared with 146/372 (39%) who had not but were seropositive (fig 3, A). In summary, compared with a less selected population, fewer PCR positive people had the low antibody concentrations at which the AbC-19 test is insensitive.

Relation between AbC-19 test results and anti-S immunoassay indices. A: cumulative anti-S (EUROIMMUN) antibody index, stratified by polymerase chain reaction (PCR) status. B: AbC-19 test band strength and its relation to anti-S (EUROIMMUN) antibody index. Test bands strength refers to sum of test band intensities (scored as 0, 1, or 2) by three observers. EIA=enzyme immunoassay
{kind=link}

Sensitivity of AbC-19 test at varying levels of anti-S antibody index. LFIA=lateral flow immunoassay
{kind=link}
Positive and negative predictive values
Table 4 shows estimates of positive and negative predictive value. Given the different estimates of sensitivity noted above from approaches 1 and 2, we observed some differences across the two sets of estimates of positive and negative predictive value presented. We consider the approach 2 estimates to be most applicable to a potential target testing population of adult frontline workers seeking antibody testing, as we would expect people with PCR confirmation to be less likely to seek antibody testing.
Positive predictive value and negative predictive value for alternative values of prevalence of previous infection. Values are percentages (95% credible intervals)
Assuming a scenario of testing 1 million key workers with unknown previous infection status, of whom 10% had actually been previously infected, we estimate that approximately 84 700 true positive and 18 900 false positive results would occur, meaning that approximately one in five positive test results would be false positive (positive predictive value of 81.7%, 76.8% to 85.8%; table 4).
Discussion
In a series of analyses involving two complementary and distinct cohorts, we made several observations relevant to the performance of emerging, scalable antibody tests for SARS-CoV-2. Firstly, on the basis of an analysis of pre-pandemic blood samples from almost 2000 blood donors in England, we estimated the specificity of the AbC-19 test to be 97.9% (95% confidence interval 97.2% to 98.4%). That is, 2.1% of people who did not have a previous SARS-CoV-2 infection incorrectly tested positive. Next, we analysed samples from 2847 key workers in the UK. Among those who self-reported previous PCR positivity, we estimated the sensitivity of the AbC-19 test to be 92.5% (88.8% to 95.1%). In this group, participants with PCR confirmed covid-19 had symptom onset a median of 63 (interquartile range 52-75) days before the sample was taken, which is sufficient for antibody development.217 This group is not, however, a representative sample of all people who have been infected with SARS-CoV-2: we would expect asymptomatic and lower severity cases to be under-represented, particularly given limited test availability in the early stage of the pandemic when many people became ill. We found evidence that this estimate of test sensitivity is upwardly biased, owing to lack of representativeness, by comparing AbC-19 test results with results on a sensitive immunoassay17 separately among those with previous PCR confirmation versus those with unknown previous infection status before antibody testing. Among the participants with PCR confirmed infection, comparison with this alternative reference standard produced a similar estimate of sensitivity (94.2%, 90.7% to 96.5%).
By contrast, among EDSAB-HOME participants who did not know or were unsure of their previous infection status (that is, all participants who had not had a previous positive PCR test, a likely user group for the test), we estimated the sensitivity of the AbC-19 test to be lower (84.7%, 80.6% to 88.1%) using the same immunoassay reference standard. This “spectrum bias”12 effect occurred because the PCR positive participants had, on average, higher antibody concentrations than other seropositive people. As people who have had SARS-CoV-2 previously confirmed by PCR would probably be less likely to seek antibody testing than other people, we consider this lower estimate (84.7%) to be a more appropriate estimate of test sensitivity for a potential use case in which people were to choose to take the test to find out their own previous infection status. For an alternative potential use of population serosurveillance,34 the estimate of test sensitivity of 86.6% (83.2% to 89.4%), which derives from an analysis of all EDSAB-HOME stream A and B participants, irrespective of PCR positivity, may be more appropriate. Finally, we observed that AbC-19 test bands were often weak, a finding also reported in another laboratory based evaluation of AbC-19.16 In our study, discordant interpretation by highly trained laboratory technicians accounted for almost 4% of tests.
Strengths and weaknesses of study
Key strengths of this study include precise estimation of test specificity owing to study of almost 2000 pre-pandemic samples, and evaluation in a cohort of almost 2900 key workers consisting of people both with known and with unknown previous infection status, enabling study of potential spectrum bias. Our study also has potential limitations. Firstly, in common with all evaluations of SARS-CoV-2 antibody tests, a “gold standard” test to evaluate a new test against is lacking. In this study, we aimed to estimate sensitivity and specificity to detect previous SARS-CoV-2 infection. Our approach to estimating test specificity based on pre-pandemic samples (collected in 2016-17) is therefore robust, as we can be confident that these samples were taken from people never infected with SARS-CoV-2. Unbiased estimation of test sensitivity for this target is, unfortunately, more difficult. We took presence of antibodies according to a sensitive immunoassay to be a proxy for previous infection.1215 After infection, most, but not all, infected people seroconvert.12 However, antibody concentrations decline over time.131519 As our approach will necessarily miss any individuals without antibodies, we may have overestimated the sensitivity of the AbC-19 test to detect previous infection, particularly over a longer time period. Furthermore, results on the immunoassays we used as reference standards are themselves subject to some small degree of misclassification as to whether antibodies are present.
Secondly, we evaluated AbC-19 in a laboratory setting, using venous blood samples, rather than having participants do the test themselves using finger prick samples. Tests were read manually, as specified in the manufacturer’s instructions for use; we used a majority of three reads as the test result, which we have shown may overestimate test sensitivity by about 1% compared with a single trained laboratory reader. The sensitivity and specificity of the test if used by untrained members of the general public at home may be lower still, a factor that would need further investigation if these tests were to be used by the general population.3 Thirdly, our cohort of key workers included few people aged over 65 years, suggesting the need for further evaluation of the assay at older ages when risk of covid-19 is substantially higher.
Finally, of the 354 participants with a positive Roche immunoassay result who had unknown previous infection status before antibody testing (the denominator for our estimate of 84.7% test sensitivity), 62% reported symptoms compatible with covid-19 since 1 January 2020. Although study eligibility criteria did not depend on symptoms, people who believed that they had had covid-19 because of previous symptoms may have been more likely to volunteer. This could mean that our estimate of test sensitivity is upwardly biased.
Comparison with other studies
Most previous evaluations of LFIAs have used a “two gate” design, in which tests are performed on two groups of samples: PCR positives and pre-pandemic sera.24202122 This study design remains an important tool in evaluating accuracy, owing to the lack of a gold standard test, as discussed above. However, we have shown that using only PCR confirmed cases can overestimate test sensitivity. Therefore, results from these previous studies may be optimistic and should be interpreted with caution. Notably, the PCR confirmed cases in our study were key workers, few of whom were admitted to hospital and a small minority of whom were asymptomatic. The extent of spectrum bias may be greater if sensitivity is estimated using only PCR positive hospital patients.
To our knowledge, only one previous evaluation of the AbC-19 test has been described in a medRxiv pre-print article that is yet to be peer reviewed.16 That previous study reported estimates of sensitivity and specificity of 97.7% (95.7% to 99.3%) and 100% (100% to 100%), respectively (notably the latter confidence interval, around an observed proportion of 350/350, is reported more appropriately as 98.95% to 100% on the manufacturer’s website23). Our estimates of both sensitivity and specificity are, therefore, lower than those from the earlier study. In a low prevalence setting, the difference in specificity would be especially important: for example, if 1 million people were tested, of whom 10% had been previously infected with SARS-CoV-2, the previous study predicts no false positives using the AbC-19 test, whereas our study predicts 18 900 false positives. The difference in results was probably driven by sample selection factors: Robertson et al estimated specificity by using only samples that were negative on three immunoassays.16 This means, for example, that any pre-pandemic samples that falsely tested positive using any of three immunoassays would be excluded. Similarly, sensitivity was estimated from only samples that were positive on EUROIMMUN and at least one other immunoassay. Exclusion of samples with unclear “true” antibody status can be expected to lead to overestimation of both test sensitivity and specificity.
Meaning of study: possible explanations and implications for clinicians and policy makers
For a population with 10% prevalence of previous infection, we estimated a positive predictive value of 81.7% for the AbC-19 test. This means that about one in five positive AbC-19 tests would be a false positive. If the AbC-19 test were to be used for mass population screening in a relatively low prevalence setting, we would anticipate a large number of false positive results (for example, 18 900 for every 1 million tests carried out). Consequently, AbC-19 test positives would need to be checked with a confirmatory assay, a practice followed in HIV and syphilis serodiagnosis, if such an assay for SARS-CoV-2 could be shown to be sufficiently specific for this purpose. The false positive rate may be higher still if accuracy of the test is lower when deployed in the field than observed in our laboratory study. We also emphasise that our study does not answer the question of whether previous infection, or presence of antibodies, implies immunity, nor the duration of antibody or immune response. The alternative use of LFIAs for population surveillance requires statistical adjustments for imperfect sensitivity and specificity.3424 The precise adjustment, however, would depend on whether the objective was to estimate the proportion previously infected or simply the proportion with antibody. Considering the decline in antibody over time, the adjustment needed to estimate the proportion previously infected would be difficult to calculate. Finally, if people were to use and read the test themselves, rather than the test being read by trained laboratory technicians, or if a digital reader were developed, the accuracy of the test as read using these alternative approaches would need to be evaluated.
Conclusions
In summary, we found evidence that the sensitivity of the AbC-19 test is lower among populations with unknown previous infection status than among PCR confirmed cases of SARS-CoV-2. This highlights the scope for overestimation of SARS-CoV-2 antibody test sensitivity in other studies, in which sensitivity has been estimated from only PCR confirmed cases. Assuming a prevalence of 10% for previous SARS-CoV-2 infection, and that the performance observed in this laboratory study can be reproduced in field use, our findings suggest that around one in five key workers testing positive with the AbC-19 assay would be false positives.
What is already known on this topic
A previous study reported 97.7% sensitivity and 100% specificity of the AbC-19 Rapid Test to detect SARS-CoV-2 antibodies
However, these findings may be optimistic because the study excluded participants with unclear antibody status according to laboratory based immunoassays
Most studies evaluating accuracy of SARS-CoV-2 antibody tests have used a “two gate” or “diagnostic case-control” design, but the effect of spectrum bias on estimates of test sensitivity is unclear
What this study adds
Using pre-pandemic samples, the specificity of AbC-19 was 97.9% (97.2% to 98.4%), implying that, at 10% prevalence of previous infection, around one in five positive results would be incorrect
Evidence of spectrum bias existed, with ~10% higher sensitivity (absolute difference) in key workers with polymerase chain reaction confirmed infection, suggesting that two gate studies may overestimate sensitivity
Trained laboratory staff reported that test bands were often weak and disagreed on device positivity for 3.9% of tests, so accuracy may be lower if used by members of the public
Acknowledgments
We thank the following people who supported laboratory testing, data entry, and management: Sarah Nalukenge, Jake Hall, Amy Gentle, Honour Gartland, Rashara Harewood, Joshim Uddin, Beejal Vaghela, and Shahmeen Ali. We also thank Steve Harbour and Neil Woodford, who provided staff, laboratories, and equipment; the blood donor centre staff and blood donors for participating in the COMPARE study; and Antoanela Colda and Richard Stewart for their invaluable contributions in the Milton Keynes General Hospital study site.
COMPARE Investigators: Jane Armitage, professor, University of Oxford, UK; Donna Cullen, consultant nurse, NHS Blood and Transplant, Bristol, UK; Susan Mehenny, operational change manager, NHS Blood and Transplant, Bristol, UK; Gail Miflin, director of clinical services, NHS Blood and Transplant, Bristol, UK; Carmel Moore, clinical trial coordinator, Anglia Ruskin University, UK; David J Roberts, associate medical director, NHS Blood and Transplant, Oxford, UK; Jennifer Sambrook, project manager, NHS Blood and Transplant, Cambridge, UK.
EDSAB-HOME Study Site Investigators: Philippa Moore, consultant microbiologist, Gloucestershire Hospitals NHS Foundation Trust, Gloucester, UK; John Boyes, consultant microbiologist, Gloucestershire Hospitals NHS Foundation Trust, Gloucester, UK; Anil Hormis, consultant anaesthetist, The Rotherham NHS Foundation Trust, Rotherham, UK; Neil Todd, consultant microbiologist, York Teaching Hospital NHS Foundation Trust, York, UK; Ian Reckless, consultant physician, Milton Keynes University Hospital NHS Foundation Trust, Milton Keynes, UK; Ray Borrow, professor, Seroepidemiology Unit, PHE Manchester, UK; Ezra Linley, clinical scientist, Seroepidemiology Unit, PHE Manchester, UK.
Footnotes
Contributors: RM, HEJ, STP, TB, MH, IO, and DW planned the study. SK, JD, EDA, and DW planned the specificity investigations. KP and JS planned the laboratory based investigation. KP, JS, SN, JH, AG, HG, and SJ conducted experiments. DW, RM, EDSAB-HOME investigators, and COMPARE investigators collected samples. RB, EL, and TB collated samples and performed assays. HEJ, AEA, RM, SK, and DW did the statistical analyses. RM, HEJ, STP, AEA, and DW wrote the paper. RM and HEJ contributed equally. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted. DW is the guarantor.
Funding: The study was commissioned by the UK Government’s Department of Health and Social Care. It was funded and implemented by Public Health England, supported by the National Institute for Health Research (NIHR) Clinical Research Network (CRN) Portfolio. The Department of Health and Social Care received a report containing these data on 10/9/2020, but had no role in the study design, data collection, analysis, interpretation of results, writing of the manuscript, or the decision to publish. DW acknowledges support from the NIHR Health Protection Research Unit in Genomics and Data Enabling at the University of Warwick. HEJ, AEA, MH, and IO acknowledge support from the NIHR Health Protection Research Unit in Behavioural Science and Evaluation at University of Bristol. STP is supported by an NIHR Career Development Fellowship (CDF-2016-09-018). Participants in the COMPARE Study were recruited with the active collaboration of NHS Blood and Transplant (NHSBT) England (www.nhsbt.nhs.uk). Funding for COMPARE was provided by NHSBT and the NIHR Blood and Transplant Research Unit (BTRU) in Donor Health and Genomics (NIHR BTRU-2014-10024). The academic coordinating centre for COMPARE was supported by core funding from: NIHR BTRU, UK Medical Research Council (MR/L003120/1), British Heart Foundation (RG/13/13/30194), and the NIHR (Cambridge Biomedical Research Centre at the Cambridge University Hospitals NHS Foundation Trust). This work was supported by Health Data Research UK, which is funded by the UK Medical Research Council, Engineering and Physical Sciences Research Council, Economic and Social Research Council, Department of Health and Social Care (England), Chief Scientist Office of the Scottish Government Health and Social Care Directorates, Health and Social Care Research and Development Division (Welsh Division), Public Health Agency (Northern Ireland), British Heart Foundation, and Wellcome. JD holds a British Heart Foundation professorship and an NIHR senior investigator award. The views expressed are those of the author(s) and not necessarily those of the NHS, NIHR, or Department of Health and Social Care.
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: funding for the study as described above; TB has received grants from the UK Government, HEJ has received grants from PHE/NIHR, and STP has received grants from NIHR during the conduct of the study; outside of this work, RB and EL perform meningococcal contract research on behalf of PHE for GSK, Pfizer, and Sanofi Pasteur, MH has received personal fees from Gilead and MSF, SJ and JD have received grants from Merck, Novartis, Pfizer, and AstraZeneca and personal fees and non-financial support from Pfizer Population Research Advisory Panel, and JS and KP report financial activities on behalf of WHO in 2018 and 2019 in evaluation of several other rapid test kits; no other relationships or activities that could appear to have influenced the submitted work.
Ethical approval: The EDSAB-HOME study was approved by the NHS Research Ethics Committee (Health Research Authority, IRAS 284980) on 2 June 2020 and the PHE Research Ethics and Governance Group (REGG, NR0198) on 21 May 2020. EDSAB-HOME is registered at http://www.isrctn.com/ISRCTN56609224. Ethical approval for use of the samples from COMPARE is covered by NHS Research Ethics Committee Cambridge East (18/12/2015; ref 15/EE/0335). COMPARE is registered at http://www.isrctn.com/ISRCTN90871183. All participants gave written informed consent.
Data sharing: Data are available on reasonable request to the corresponding author.
The manuscript’s guarantor affirms that this manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
Dissemination to participants and related patient and public communities: Links to this work will be included on the study website (https://www.gov.uk/government/publications/evaluating-detection-of-sars-cov-2-antibodies-at-home-study), and participants will be alerted that the work has been published.
Provenance and peer review: Not commissioned; externally peer reviewed.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.