Public sector financial support for late stage discovery of new drugs in the United States: cohort study
BMJ 2019; 367 doi: https://doi.org/10.1136/bmj.l5766 (Published 23 October 2019) Cite this as: BMJ 2019;367:l5766
- Rahul K Nayak, resident physician1,
- Jerry Avorn, professor of medicine1,
- Aaron S Kesselheim, professor of medicine1
- 1Program On Regulation, Therapeutics, And Law (PORTAL), Division of Pharmacoepidemiology and Pharmacoeconomics, Department of Medicine, Brigham and Women’s Hospital and Harvard Medical School, 1620 Tremont Street, Boston, MA 02120, USA
- Correspondence to: A S Kesselheim akesselheim{at}bwh.harvard.edu (or @akesselheim on Twitter)
- Accepted 23 September 2019
Abstract
Objective To determine the extent to which late stage development of new drugs relies on support from public funding.
Design Cohort study.
Setting All new drugs containing one or more new molecular entities approved by the US Food and Drug Administration (FDA) between January 2008 and December 2017 via the new drug application pathway.
Main outcome measures Patents or drug development histories documenting late stage research contributions by a public sector research institution or a spin-off company, as well as each drug’s regulatory approval pathway and first-in-class designation.
Results Over the 10 year study period, the FDA approved 248 drugs containing one or more new molecular entities. Of these drugs, 48 (19%) had origins in publicly supported research and development and 14 (6%) originated in companies spun off from a publicly supported research program. Drugs in these groups were more likely to receive expedited FDA approval (68% v 47%, P=0.005) or be designated first in class (45% v 26%, P=0.007), indicating therapeutic importance.
Conclusions A review of the patents associated with new drugs approved over the past decade indicates that publicly supported research had a major role in the late stage development of at least one in four new drugs, either through direct funding of late stage research or through spin-off companies created from public sector research institutions. These findings could have implications for policy makers in determining fair prices and revenue flows for these products.
Introduction
Public sector support funds much biomedical research conducted at universities, academic medical centers, other non-profit organizations, and government laboratories. In the United States, such support comes primarily from the National Institutes of Health (NIH), but also from other federal or state entities, disease focused charities (eg, the Cystic Fibrosis Foundation), or biomedical research philanthropies (eg, the Howard Hughes Medical Institute). Such research often has a key role in elucidating potential drug targets and understanding the pathophysiology of disease—activities that are central to drug discovery. This costly upstream research could stretch back several decades before a drug reaches clinical trials or is approved by the US Food and Drug Administration or another regulator.1 One recent report found that NIH funding contributed to published research associated with all 210 new drugs approved by the FDA in 2010-16.2 However, public support often funds later stage translational research as well, and might also cover the conduct of some clinical trials required for drug approval. At some point in the development cycle of most prescription drugs, pharmaceutical manufacturers become involved and often expend substantial resources in moving drugs through pivotal clinical trials and FDA approval and in developing means of large scale production. For some new drugs, their investigation, discovery, and development occur entirely within the corporate sector, but this is uncommon.
The role of public sector contributions versus those of the pharmaceutical industry to drug discovery remains a point of controversy, with some arguing that companies’ investment in drug discovery is the key source for new drug development.3 This view, along with the costs of conducting clinical trials, is used to justify high drug prices,456 although the actual cost of drug development is difficult to accurately estimate.7 The relative contributions of publicly supported research and the pharmaceutical industry can be difficult to separate for a particular product. However, the upstream, pre-competitive, basic science research that so many new drugs depend on is generally thought to be predominantly funded by public support, while clinical trials are generally thought to be predominantly funded by the pharmaceutical industry.
One way to assess the contributions of various sectors in the drug development continuum is to define the research that justifies patent claims on the drug—the basis of drug ownership and pricing. Patent-generating research tends to occur later in development because patent law requires inventors to describe a well defined product or process before a patent can be issued. Other patentable steps can cover a drug’s synthesis, the chemical composition of its active ingredient, or its method of use. Patents provide the basis for market exclusivity, granting the patent holder ownership over the product and therefore the capacity to control the drug’s US price, as well as considerable leverage in pricing negotiations in other healthcare systems. Although patents enable a manufacturer to demand high drug prices, patent based levers have been proposed, and occasionally have been used with success, to achieve public policy goals, such as helping ensure access to essential drugs in low income settings.89101112
Previous studies have reviewed the data submitted to the FDA to investigate public sector research support of drug development that is reflected in these patents. Although some follow-on patents are clinically trivial and not germane to a drug’s innovative contribution to patient care, the patents submitted to FDA are typically those that are considered key to the drug’s invention and clinical use. Earlier analyses found public sector research institutions to be associated with the patents covering 4.6% of new molecular entities approved in 1981-90,13 6.7% of new drugs approved in 1990-99,4 9.0% of new molecular entities approved in 1988-2005,14 and, most recently, 13.6% of new molecular entities approved between 1990-2007.15 This increase in the proportion of publicly supported research contributions has been attributed to the changing nature of drug development, with large manufacturers investing proportionally less in internal basic and translational research themselves.15
Biomedical research support from the public sector has continued to grow in recent decades, although until recently it had fallen in inflation adjusted terms. By contrast, more large pharmaceutical manufacturers have focused on purchasing drugs developed in start-up companies, many spun out of public sector research institutions. We therefore sought to examine the extent of publicly supported research for new FDA approved drugs as reflected in patent data from 2008-17, including the role of start-up biotechnology companies emerging from publicly supported research.
Methods
To identify recently approved drugs originating from publicly supported research, we examined patent data listed with the FDA, using an approach similar to that used in previous studies.4131415 The FDA’s Orange Book describes the key US patents that have been granted for a drug substance (active ingredient), drug product (formulation and composition), or method of use. The Orange Book does not include other patents that might be held on the drug, such as those on manufacturing processes, although public sector institutions are less likely to contribute to these patents. It also does not include non-US patents or patents that have expired.
The Orange Book could miss patents that expired before drug approval, or intellectual contributions that were never patented, so we used additional data sources to supplement our analysis. The Merck Index, a chemical entity reference, was searched for supplementary patent information. The index generally lists one or two of the most important patents on a given drug, usually on the final formulation of the active ingredient. For many drugs, the Merck Index patent(s) were the same as those found in the Orange Book. Patents that were listed in the Merck Index alone typically had expired before drug approval and therefore were not included in the Orange Book.
The patent data available through these sources does not comprehensively capture all patents on a drug and can underestimate non-patent-based intellectual contributions to new drug discovery, particularly in circumstances where patents were not pursued. Therefore, we also used drug discovery histories to identify key missing intellectual contributions. We used the drug monograph database AdisInsight, as well as our own investigations, as described in detail below.
Data collection
Drug approval
We identified all new drugs approved by the US FDA between 2008 and 2017 using the Drugs@FDA database,16 including all drugs approved through the new drug application process for small (that is, non-biological) molecular entities. Biological treatments, vaccines, and gene treatments were excluded because they are approved through a separate biological license application pathway for which patent information is not collected by the FDA. Novel drugs were identified based on the FDA’s type 1 approval designation (drug products containing a new molecular entity) and FDA lists of new drug approvals by year.1 Treatment categorisation was assigned on the basis of the drug’s initial FDA approved indication.
Approval pathway
We defined a drug’s approval pathway using FDA listings of drugs that received standard, priority, accelerated, breakthrough, fast track, first-in-class, or Orphan Drug Act designation; a drug may have received more than one of these definitions. We considered such designations only for a drug’s initial approval. In 2008-10, the FDA did not publish fast track designation or classify drugs as first-in-class on their website. For those years, we used other published databases.1718 A full list of drugs included in this study and their FDA approval pathways is included in supplementary table S1.
Patents
As described above, we then obtained patent data for each approved drug from several sources. We issued a Freedom of Information Act request to obtain historical Approved Drug Products with Therapeutic Equivalence Evaluations (Orange Book) data files for 2001-17 that, along with a data file from March 2018, were used to obtain patent data submitted to the FDA, including those that might have expired. Since patents can be added after drug approval, we also conducted a manual search of the Orange Book for drugs with no patents listed in data files as of April 2019 and found one additional drug with a patent added by the manufacturer. The FDA requires that certain key patents be submitted by the manufacturer for inclusion in the Orange Book, including patents on the drug’s substance (active ingredient), product (formulation and composition), or method of use. The Merck Index was used to supplement patent information and typically listed one or two key patents related to the drug’s active ingredient (final formulation) or synthesis.19
We next obtained data about the patents granted for the study drugs by using the PatentsView application programing interface developed by the US Patent and Trademark Office and the PatentsView R package, using the programming language R version 3.5.0.2021 This process allowed identification of a patent’s inventor and the organization that was assigned ownership. Typically, these data reflect the information that was assigned at time of the patent grant. This method would not identify information, such as disclosure of government funding, that was later corrected. We manually investigated patents which could not be queried using this method to determine the inventor and assigned ownership for each product.
Drug monographs
Examining only the patent information from the Orange Book could provide an incomplete definition of the key contributions to a drug’s invention if key patents expired before drug approval. We used the Merck Index to identify these patents, although such an approach would miss important contributions in cases in which a patent was intentionally not pursued. Previous studies have used bibliometric approaches to capture public supported research contributions by examining publications or patent citation.214 For example, Cleary et al found every drug approved from 2010-16 had associated NIH funding contributing to published research.2 But these approaches capture the substantial role of public research on the upstream, basic science research that underpins drug discovery. In this paper, we focus on the later stage contributions by public sector institutions.
We therefore supplemented the patent analyses with the drug monograph database, AdisInsight, which details a drug’s discovery history, preclinical and clinical development, regulatory status, and pharmacological properties. To develop the monograph, researchers examine the relevant scientific publications, patents, news media, financial transactions, and regulatory documents to create an expert summary of the drug’s development history. AdisInsight then creates a descriptive narrative of the research and development history and assigns classifications of “originators” and “developers” for each drug. The originator usually refers to the institution that AdisInsight reviewers concluded originally invented or discovered the active ingredient, and developers were any institution that helped with conducting, funding, or supporting the clinical trials. Given our interest in the role of late stage research contributions, we focused on the drugs that were listed as originating from publicly supported research institutions.
Because the AdisInsight methodology is proprietary and does not provide explanations for why a monograph classified an institution in a given way, we further studied any drug that listed a publicly supported research institution as an originator in the AdisInsight listing if no Orange Book or Merck Index patent was assigned to that institution. We began with targeted web searches to verify the connection between the drug and the AdisInsight listed originating institution. One author (RKN) searched for evidence of news articles, university press releases, researchers’ academic profiles, scientific publications, US Securities and Exchange Commission (SEC) filings, and patents that confirmed that the drug’s discovery or development had late stage research contributions from the institution (that is, intellectual contributions similar to a patentable invention, such as the drug’s discovery or invention, or method of synthesis). If we found corroborating evidence, we considered the AdisInsight classification to be verified, confirming that the drug was based on publicly supported research contributions, as described further below. In one case, we were unable to corroborate the connection, and did not classify the drug as having a publicly supported research origin.
Drug development histories
Similar to the approach used to verify entries from AdisInsight, we conducted web searches to investigate the development history for each drug in the study. We examined publications focused on drug development (eg, Nature Reviews Drug Discovery), researcher or inventor biography pages, news articles, academic technology transfer sites, and Wikipedia entries to identify other late stage research contributions supported by public funds that were not captured in the process above. Because we found evidence for publicly supported research institutions’ involvement from our initial web searches, we then conducted targeted searches for the drug and the possible researchers and institutions involved to seek primary academic publications, news media sources, or SEC filings that could verify the public sector institution’s role.
Identifying public sector research institutions and spin-off companies
To better understand the development pathway for each drug, we examined the assignee information for each patent (or institution identified from the drug monograph and development history investigations) and conducted web searches to classify the organization as either a public sector research institution (universities, hospitals, non-profit foundations or institutions, or government laboratories) or a private, non-public organization (primarily biotechnology or pharmaceutical companies). For cases in which a patent had multiple assignees, we characterized the patent as held by a public sector research institution if one or more of the assignees was a public sector institution.
Whenever possible, we identified start-up firms spun out from publicly supported research institutions. For each company, we investigated the foundational history using web searches of the company’s website, new articles about the company, Wikipedia entries, SEC filings, and profiles of the company or its founders. Indications that the company was spun out from a publicly supported research institution were followed up to confirm or refute such a connection. For example, we reviewed the company’s own description of its founding, university press releases, and university profiles of the academic founder to determine whether the company could fairly be described as an academic spin-off company. Although we identified many companies that were spun out from public sector research institutions, this did not automatically mean the drug in question was based on publicly supported research. To ensure accurate categorization, we investigated whether the FDA approved drug was based on the same technologies or products that had led to the formation of the spin-off company, to characterize whether the drug truly could be considered as being based on an extension of publicly supported research.
Data analysis
Determining public sector contributions
To determine whether a drug had a major research contribution from publicly supported research late in its development, we further analyzed the contributions of the institutions involved in the development. We considered a drug to have been based on public support if we found any patents for the product that were owned by a public sector research institution or that declared government funding for the product (that is, a government interest statement). We also included drugs listed in the drug monograph database as “originating” in a public sector research institution that we could independently verify as well as from our own review of drug development histories as described above. For drugs that were included without patent data, all authors reviewed and agreed with the drug’s classification of having late stage, publicly sponsored research contribution. For a combination drug containing a new molecular entity (eg, antiviral treatments), we considered the drug to have contributions from publicly supported research if one or more of the active ingredients had contributions from a publicly supported research, consistent with the approach taken by Stevens et al.15
For spin-off companies, as described above, if we found evidence that a drug was based on the same technology or innovation that led to the creation of the company, we classified the drug as having a late stage research contribution from a spin-off company that had its origin in publicly supported research. We excluded drugs that were unrelated to a company’s original spin-off product or technology.
Many aspects of a drug can be patented, with some patents representing more important innovation than others. Firstly, for each drug in which one or more patents were central to identifying a publicly sponsored research contribution, we calculated the share of patents held by publicly supported research institutions and their spin-off companies, compared with the total patents identified for that drug. We report below the unweighted average of the share of patents held by publicly supported research institutions and their spin-off companies, with a 95% confidence interval assuming a normal distribution. Secondly, we determined whether the oldest patent identified was held by a publicly supported research institution or a spin-off company. Thirdly, we examined all the Orange Book patents for that drug to determine whether publicly supported research led to patents on its substance (active ingredient) or product (formulation and composition), which are typically more foundational.
To analyze whether drugs based on publicly sponsored research or spin-off contributions were significantly more likely to have been granted expedited FDA review or be a first-in-class drug, we conducted a Fisher’s exact test of independence with a Bonferroni adjusted alpha level of 0.007 (0.05/7).
Patient and public involvement
While we recognize that patients and members of the public are the ultimate stakeholders and end users in late stage new drug discovery, we were unable to involve them as partners in considering the research question, the analysis, or the outcomes. The analysis required in-depth legal and specialist knowledge with access to large databases. We plan to make the published information available to key public interest and advocacy groups to further transparency around the pathways to late stage new drug discovery.
Results
Patent and originator information
We identified 248 novel drugs that represented new molecular entities approved for the first time between January 2008 and December 2017 (21 were combinations, of which some had more than one new molecular entity, leading to 253 new molecular entities). Using the FDA Orange Book, we identified at least one patent for 230 (93%) products. The Merck Index identified at least one patent for an additional 14 (6%) products, leaving only five products (2%) with no available patent information. We identified drug monographs for 246 (99%) products, and either patent or monograph data were available for all but one drug (n=247).
Publicly supported research contributions
Our review of patents and supporting data found that a quarter (n=62) of all new products had documented late stage research contributions from a publicly supported research institution or spin-off company. Forty eight products (19% of all new drug approvals) had evidence of direct publicly supported research (table 1 and table 2). For all but one, the contributions were related to the drug’s initial discovery, synthesis, or other key intellectual property leading to a patentable invention. For 30 of these drugs, publicly supported research institutions directly held one or more of the key patents. Another seven drugs had direct publicly supported research origins, although the patents listed in the Orange Book were held by a spin-off company. The remainder of drugs with public support contributions was found through the drug monograph database and investigations of the drugs’ discovery and development histories. One of these drugs, benznidazole, a treatment for Chagas disease, is a distinct case because it received development support from the Drugs for Neglected Diseases Initiative and others, and is being sold on a “no profit no loss” basis.22 However, the drug was originally developed by Hoffman-La Roche in the 1970s, which then donated the rights to the drug to the Brazilian government in 2003.23
New drugs with publicly supported research contributions in 2008-12
New drugs with publicly supported research contributions in 2013-17
Fourteen (6%) drugs were developed by spin-off companies that were based wholly or in part on publicly supported research; all but two were identified through patents listed in the Orange Book (table 3). For example, the hepatitis C treatment sofosbuvir (Sovaldi) and other sofosbuvir-containing combination drugs were in this category because they originated at Pharmasset, a spin-off company based on federally funded research performed at Emory University.24 In addition to these 14 drugs, at least 10 other drugs had origins in spin-off companies, but these were excluded because it was unclear whether these drugs were related to the technologies or drugs that initially gave rise to the spin-off company. Full details of the rationale used to classify drugs as having publicly supported or spin-off research contributions can be found in appendix 1.
New drugs with contributions from spin-off companies based on publicly supported research
We identified most of the drugs that had publicly sponsored research or spin-off contributions through patent data available through the Orange Book (n=47). Two were found from patents in the Merck Index, while eight came from the drug monograph classification and five from our own drug history investigations. The contributions of each of the date sources are shown in figure 1. The data sources had strong concordance (appendix 2).

Proportion of new drugs with publicly sponsored research or from spin-off companies, identified by data source. The figure shows the breakdown of the relative share of the data sources used to identify publicly supported research contributions. The first four columns represent the drugs identified as having public sponsored research origins, and the last column represents those with spin-off company origins. Most drugs identified as publicly supported research contributions had Orange Book patents assigned to either to a public sector institution (28/62) or spin-off company (an additional 7/62). Two more drugs were primarily identified by Merck Index patents, six by AdisInsight entries, and five by the authors’ investigation of the drug’s history. Finally, 14 drugs were identified as originating in a spin-off company. For the spin-off drugs, 12 had Orange Book patents held by the spin-off company (the remaining two had Orange Book patents held by the successor company of the spin-off). OB=Orange book; MI=Merck Index; AI=AdisInsight; DH=drug history (author’s investigation); SO=spin-off company
{kind=link}
Contributions by drug class
Late stage, publicly supported research contributions by drug class were concordant with the overall total number of approvals by drug class (table S2). In hematology-oncology, 17 (27%) drugs were based on publicly supported research; 13 (33%) drugs were in infectious diseases, and 10 (63%) were among diagnostics agents Each of these drug classes had a higher share of drugs from publicly supported research than the average in our sample. Conversely, for psychiatric drugs, we did not find late stage, publicly supported research contributions for any of the 15 recently approved drugs.
Patent characteristics
Of the 48 drugs identified as having late stage, publicly supported research contributions, 38 (80%) had at least one patent held by a publicly supported research institution or spin-off company. For these drugs, 70% (95% confidence interval 60% to 81%) of the patents, on average, were held by a publicly supported research institution or spin-off (table 4). A US government interest statement was declared on at least one patent in the case of 17 drugs. For 32 (84%) drugs, the oldest patent identified was held by a publicly supported research institution or spin-off company. Of the 35 drugs for which we identified at least one Orange Book patent held by a publicly supported research institution or spin-off company, 27 (77%) had at least one patent held on the key properties of the drug’s product or substance. Similar findings applied to drugs with late stage contributions from a spin-off company (table 4).
Characteristics of patents on new drugs with origins in publicly supported research contributions. Data are number of drugs unless stated otherwise
FDA approval process
New drugs based on contributions from publicly supported research or spin-off companies were substantially more likely to receive FDA approval through one or more expedited development or review pathways than new drugs without these characteristics (68% v 47%, P=0.005) and to be first in class (45% v 26%, P=0.007; table 5). Both are indicators of potentially greater therapeutic importance.
Regulatory designations and other classifications of new drugs by the US Food and Drug Administration. Data are number (%) of drugs unless stated otherwise
Discussion
Principal findings
In the present study, we studied all new drugs approved by the FDA in 2008-17 to determine whether their patents or other late stage, drug discovery contributions documented origins in publicly supported research. The development of a new drug treatment is a complicated process. Important and costly contributions come from both the public and the private sectors, in varying proportions. Under current patent law, making a seminal discovery about an important drug target, or even taking development of a new approach almost to the point of creating a marketable product, are not sufficient to win intellectual property rights to the drug that emerges from this chain of research. However, an entity (usually a pharmaceutical company) that performs these final steps is usually granted ownership over the product, and thus the chance to establish its price (in the US) and own the revenue it generates. Substantial private investment from industry is critical for many drugs for basic and clinical research, but by funding the clinical trials and the regulatory compliance necessary to win FDA approval, the role of the publicly supported research investments that served as the basis of the drug’s discovery are often not as clearly attributed.
Our analysis found that publicly supported research in non-profit institutions (19%) or spin-off companies that had their origins in public funded research (6%) made important late stage intellectual contributions to at least one in four new drugs approved in the past decade. These data highlight the substantial and increasing role of late stage, publicly supported research in the development of new drugs (fig 2),4131415 in addition to the more widely acknowledged contributions of public funding to the foundational basic science discoveries on which most new products are based.
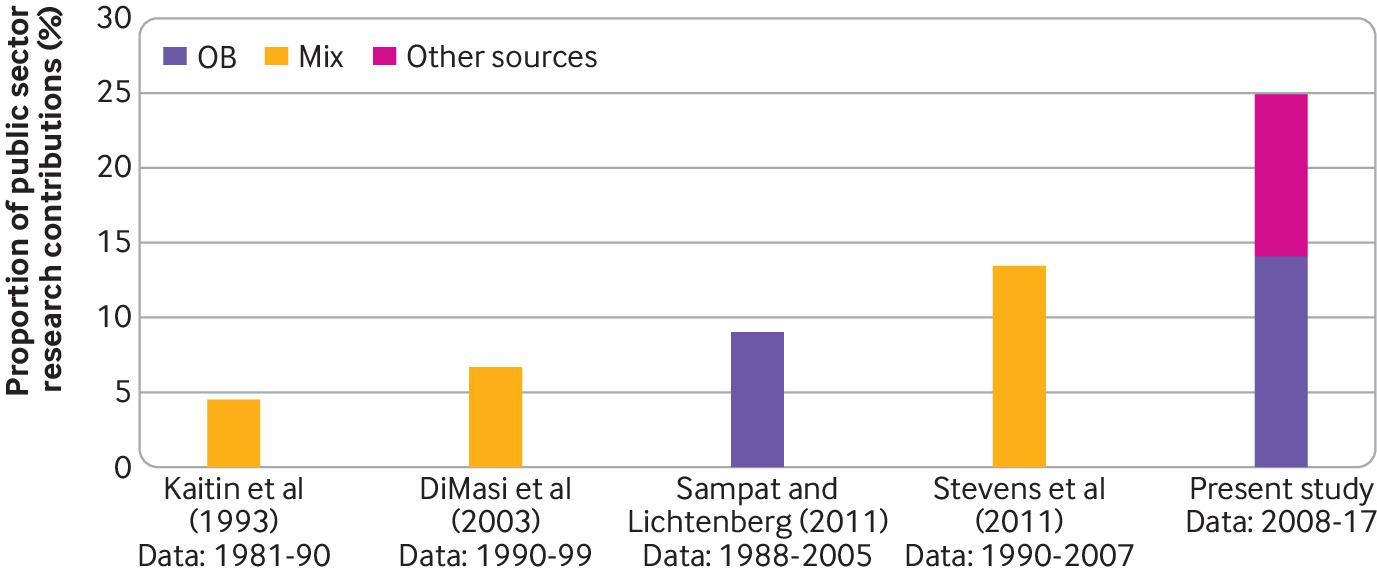
Changes in rates of publicly sponsored research contributions to new drug discovery, by study over time with data sources used. The figure compares the present study with previous studies examining public sector contributions to new drug discovery via patent analysis. The Kaitin and DiMasi studies used the Tufts Center for the Study of Drug Development databases that use Orange Book patents as well as other proprietary datasets (not fully described). The analysis by Sampat and Lichtenberg examined patents listed only in the Orange Book. The Stevens et al study examined the Orange Book, proprietary licensing databases, and conducted a survey of university technology transfer managers to identify drugs that originated in public sector institutions. The relative contributions of the various sources were not disclosed, and how the studies dealt with contributions from public sector spin-off companies is not clear. However, the study period for Stevens et al was similar to that of Sampat and Lichtenberg, so the difference between their findings might be a result of the additional sources used. OB=Orange Book
{kind=link}
Strengths and limitations of study
This study had several limitations. Firstly, we identified a product as having a late stage, publicly supported research component if the patent and drug discovery history documented a key contribution by a public sector entity or spin-off company in its development. This method does not confirm that such public investment was the only source of a drug’s creation, or that there was no private sector contribution. We did not attempt to weigh the relative importance of public versus private sector innovation for particular drugs; for many products, important corporate investment occurred as well. As a result, the substantial contributions of public support to late stage drug development would not confer partial public ownership of most of these products under current patent law. In fact, this flow of publicly funded research knowledge into the private sector for commercialization seems to have been a major goal of the original Bayh-Dole legislation, rather than an unintended consequence of it.25
Secondly, our analysis relies primarily on patents listed in the Orange Book and proprietary databases of drug development to identify public sector origins, which represents a limited set of patents associated with a drug, even though these patents are generally considered the most important in a product’s intellectual genealogy. Further investigation into the origins of each drug might have yielded additional relevant information. This approach might underestimate the contributions of publicly supported and academically based researchers who collaborate with pharmaceutical companies if a patent derived from such collaboration is held by the sponsor. For example, Ciba-Geigy (now Novartis) held the patent for imatinib for years but had not developed the product clinically until Brian Drucker at Oregon Health and Science University persuaded the company to provide him with samples of it for his research on chronic myeloid leukemia, leading to the profitable product Gleevec, approved in 2001.26 Although that drug preceded the study period under consideration, the patents on the drugs were held by Novartis and there was no patent evidence held by (or royalty payments made to) the academic medical center that was essential in its development.
A third limitation is that we did not include biological agents in this study despite their clinical and economic importance. This exclusion was because the FDA does not collect patent data for drugs approved through the Biologic License Application process. Biological medicines represent an increasingly important component of drug treatment both clinically and economically, and the current regulatory framework limits the opportunity to produce generic drugs. Further research to investigate the role of late stage publicly supported research for biological medicines is necessary. Lastly, we limited our investigations to English language publications, websites, and media coverage to verify key contributions made by publicly supported research.
Our approach is not the only way of quantifying public sector research contributions, because it could miss a great deal of important scientific discovery funded and conducted with the support of public funding. The patent based approach used also underestimated the additional role of upstream basic and translational science research supported by public funds that is critical to the discovery of new drugs; this contribution has been clearly described by others.227 In addition, previous studies in the US and the UK have shown how publicly funded research create substantial direct and indirect economic value, complementing private industry research expenditure, innovation, and privately held patents.2829 Thus, our approach does not capture the totality of returns generated as a result of public investment.30
Our analysis did not consider the relative amounts of financing that comes from public and private sector sources. We did not tabulate the cost of clinical development within industry required for final product development and regulatory approval, which can be substantial. We also did not consider the substantial public subsidies for the drug development enterprise, which include federal expenditures in the form of research and development tax credits and the Orphan Drug Act tax credit, which was a subsidy equal to 50% of the cost of the qualifying trial (until 2017, when it was reduced to 25%). Our study also did not take into account direct funding of drug development in the form of publicly funded clinical trials as well as research and small business grants, and indirect support in the form of public sector research institutions hosting industry funded clinical trials.
Comparison with other studies
One difference between our analysis and previous studies is that earlier research relied predominantly on patent data provided in the FDA Orange Book,4131415 which could underestimate the role of publicly supported research if patents had expired at the time of drug approval, were never pursued, or were held by spin-off companies. Limiting our analysis to only those drugs with Orange Book patents held by public sector research institutions would have identified 28 drugs, or just 11% of new approvals (table 4). We would have missed, for example, an additional seven drugs that were ultimately determined to have publicly supported research origins, but the listed Orange Book patents were held by spin-off companies. Incorporating other patent sources, drug histories, and basic investigations to confirm a drug’s development history, including the role of spin-off companies with origins in publicly support research, more accurately represents the late stage contributions of public sector funding to drug discovery and development.
These findings also reflect the continuing trend of an increasing role of publicly supported research in late stage research leading to new drug discovery, which has also been seen in previous studies (fig 2).4131415 This increasing trend might be because of ongoing congressional funding of biomedical research through the NIH since the 1990s.3132 The fruits of that earlier publicly supported research would be seen in recent drug approvals, because it typically takes a decade or more from drug discovery to approval. In addition, university-owned patents of all kinds have increased as a share of all US patents from 0.28% in 1969 to 0.83% in 1985 to 1.89% in 2012.33 This rising share reflects increased productivity as a result of more biomedical research funding as well as policies to more actively pursue patents by academic technology transfer offices in the nearly four decades since passage of the Bayh-Dole Act.34 For example, we identified at least 17 drugs for which US government interest was disclosed on patents; this number is likely to be an underestimate owing to evidence that government funding is underdisclosed on patent applications.93536 Because our study examined the assignee data on the patent grants, we would miss any updates submitted to the US Patent and Trademark Office of corrections clarifying government contributions. Recent analysis found these corrective updates to be as high as 20-30% of all patents for some academic insitutions.37
Our data also indicate that drugs with contributions from publicly supported research or spin-off companies are 1.4 times as likely to receive an expedited FDA approval process and 1.7 times as likely to be first in class (table 5). Although these data are crude measures of innovativeness, they suggest that publicly supported research is not only leading to new drugs but also leading to new classes of drugs with novel mechanisms of action, a finding consistent with previous studies.1529383940
Policy implications
These findings have several implications for healthcare and regulatory policy, particularly in the US. The US biomedical enterprise underlies a substantial proportion of new drug development,41 although by no means all of it.42 At the same time, drug prices are substantially higher in the US than anywhere else in the world, with Americans paying on average about twice the per capita amount for prescription drugs as citizens of other advanced industrialized contries.4344 Identification of drugs with late stage, publicly supported research contributions, particularly those for which such institutions hold key patents, could represent a useful policy lever. Such drugs include nusinersen (Spinraza, for spinal muscular atrophy; list price US$750 000 (£610 400; €685 000) in the first year of use),45 eliglustat (Cerdelga, for Gaucher disease; $310 250/year),46 and enzalutamide (Xtandi, for prostate cancer; $129 000/year).47 The prices of these drugs, each of which relied on substantial academic development, have been criticized in the US and all are substantially lower in other countries.
For these and other drugs, the contributions of publicly funded research to their development could be expected to be compensated by more favorable pricing to payors, the largest of which is the US government itself. Although the university that largely developed Xtandi did receive a lucrative licensing agreement, such compensation is often not the case. Whether such payments—most of them far less lucrative—represent adequate compensation to the innovator institution for its role in drug development is unclear.48 In addition, such agreements when they exist do not benefit those who purchase these drugs at such high prices. Beside commercial insurers and state governments, such payors include the federal government and patients themselves—all of whom have already made investments into a drug’s creation, such as through taxpayer support of NIH funding.4950 Given the current US debate on whether the public is getting a fair return on public investment51 and when rising drug prices are defended as being necessary to fund industry innovation, without which new treatments would be expected to slow dramatically, our findings can inform this public discussion.
In theory, the US government retains a fully paid license, as well as so-called march-in rights, for patents with government funded origins. These provisions could allow the government to use the patented product for its own purposes or, in the case of march-in rights, grant additional licenses to others if needed to address health needs. Raising the prospect of using these authorities has had some effect in cases in which the NIH helped negotiate agreements on the licensing of stem cell patents. In addition, the US Centers for Disease Control and Prevention was able to liberalize the licensing of patents related to avian flu, and the manufacturer of ritonavir reduced a planned price increase for government agencies after a march-in petition was submitted to the NIH.52 But to our knowledge, neither authority has ever been activated by a federal agency for any drug, even in the face of critical drug shortages or extreme price spikes.8 Of course, these legal authorities, even if they were ever to be exercised, would only apply to drugs for which government patent rights can be identified. Government interest statements are underdisclosed and this study represents only a limited patent landscape analysis for each drug; thus, only a subset of drugs with public sector contributions in this study had definitively identified US government interests.
However, hundreds of public sector institutions have recognized their ethical obligation to make technology transfer agreements that will promote the public’s interest and equitable access to medicines, although how well these principles are practiced by many institutions is unclear.101112 While these technology transfer principles were developed and implemented primarily to promote access in low and middle income countries, this approach could also be used to ensure the public has access to very costly taxpayer funded drugs. Additionally, other broadly applicable policy tools might be available, such as negotiating lower drug prices (currently not in practice in the US) or even issuing compulsory licenses to meet public health needs regardless of drug origin or patent ownership, although greater justifications for the use of such interventions might be needed for high priced drugs with identified public sector contributions.
Conclusion
We reviewed comprehensive patent and related data to trace the intellectual contributions of publicly supported research to the discovery and development of new drugs. Our findings highlight the important role of public and philanthropic funding in the drug research and development ecosystem. We found that such institutions and their corporate spin-off companies were central to the development of at least a quarter of all new drugs approved by the FDA in 2008-17, either through direct contributions to drug development or through the formation of spin-off companies based on earlier public funding. Drugs approved following major public sector funding were more likely to receive an expedited development or approval pathway designation from the FDA and more likely to be a first-in-class treatment, suggesting that they were more likely to be novel and potentially clinically important.
Our findings also document a substantial increase in the share of drugs in the US with publicly supported research origins compared with previous studies. This increased share could reflect our more comprehensive methodological approach as well as growing taxpayer funding for biomedical research and increased pursuit of patents by public supported research institutions over the past few decades. These findings provide additional data for the ongoing debate on support for public sector biomedical research, and the best ways to take these key contributions into account in determining the ownership of and fair prices for new drugs, especially those priced at very high levels.
What is already known on this topic
Publicly sponsored research has a substantial role in the upstream, basic science investigations behind most new drugs
About 14% of new molecular entities approved in 1990-2007 had late stage, patentable contributions from a public sector research institution
What this study adds
Among 248 new small molecule drugs approved by the US Food and Drug Administration in 2008-17 containing a new molecular entity, 25% had key late stage research contributions from public sector research institutions (19%) or spin-off companies from one of these institutions (6%), often with key patents on the drug credited in part to these institutions
These publicly sponsored drugs were more likely to receive expedited regulatory designation and be first in class, suggesting high therapeutic importance
Publicly sponsored research has a substantial and growing role in late stage drug discovery and development, and this information can inform policies related to drug pricing and fair compensation for public sector investment.
Acknowledgments
We thank ChangWon C Lee (Brigham and Women’s Hospital/Harvard Medical School) for his research assistance in the revision process.
Footnotes
Contributors: RKN contributed to the design, conduct, analysis, and interpretation of results; JA contributed to the design and interpretation of results; ASK contributed to the design and interpretation of results. All authors contributed to and approved the final manuscript. The authors had full access to all the data in the study and all authors shared final responsibility for the decision to submit for publication. RKN is guarantor. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding: This work was supported by the Arnold Ventures, Open Society Foundations, and the Engelberg Foundation. ASK is also supported by the Harvard-MIT Center for Regulatory Science. The funders had no role in study design, data collection, data analysis, data interpretation, or writing of the report.
Competing interests: All authors have completed the ICMJE uniform disclosure form at http://www.icmje.org/coi_disclosure.pdf and declare: support from the Open Society Foundations, Arnold Ventures, Engelberg Foundation, and Harvard-MIT Center for Regulatory Science for the submitted work; no financial relationships with any organizations that might have an interest in the submitted work in the previous three years, and no other relationships or activities that could appear to have influenced the submitted work.
Ethical approval: This study was not submitted for institutional review board review because it is based on publicly available data and involved no health records (45 Code of Federal Regulations [CFR] 46.102).
Data sharing: No additional data available.
The lead author affirms that the manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.