Selective serotonin reuptake inhibitors and venlafaxine in early pregnancy and risk of birth defects: population based cohort study and sibling design
BMJ 2015; 350 doi: https://doi.org/10.1136/bmj.h1798 (Published 17 April 2015) Cite this as: BMJ 2015;350:h1798
- Kari Furu, director and senior researcher1,
- Helle Kieler, associate professor in obstetrics and gynaecology2,
- Bengt Haglund, associate professor and senior researcher2,
- Anders Engeland, professor and senior researcher13,
- Randi Selmer, senior researcher1,
- Olof Stephansson, associate professor and senior consultant in obstetrics and gynaecology24,
- Unnur Anna Valdimarsdottir, professor56,
- Helga Zoega, associate professor5,
- Miia Artama, senior researcher78,
- Mika Gissler, research professor910,
- Heli Malm, specialist in obstetrics and gynaecology1112,
- Mette Nørgaard, associate professor and senior consultant in clinical epidemiology13
- 1Department of Pharmacoepidemiology, Division of Epidemiology, Norwegian Institute of Public Health, PB 4404 Nydalen, NO 0403 Oslo, Norway
- 2Department of Medicine Solna, Centre for Pharmacoepidemiology, Karolinska Institutet Stockholm, Sweden
- 3Department of Global Public Health and Primary Care, University of Bergen, Bergen, Norway
- 4Department of Women’s and Children’s Health, Division of Obstetrics and Gynecology, Karolinska Institutet, Stockholm, Sweden
- 5Centre of Public Health Sciences, Faculty of Medicine, School of Health Sciences, University of Iceland, Reykjavik, Iceland
- 6Department of Epidemiology, Harvard T H Chan School of Public Health, Boston, MA, USA
- 7Department of Medical Genetics, University of Helsinki, Helsinki, Finland
- 8Department of Child Psychiatry, University of Turku, Turku, Finland
- 9THL National Institute for Health and Welfare, Helsinki, Finland
- 10Nordic School of Public Health, Gothenburg, Sweden
- 11Teratology Information Service, HUSLAB and Helsinki University Central Hospital, Helsinki, Finland
- 12Department of Clinical Pharmacology, Helsinki University, Helsinki, Finland
- 13Department of Clinical Epidemiology, Institute of Clinical Medicine, Aarhus University Hospital, Aarhus, Denmark
- Correspondence to: K Furu kari.furu{at}fhi.no
- Accepted 10 March 2015
Abstract
Objective To assess whether use of specific selective serotonin reuptake inhibitors (SSRIs) or venlafaxine in early pregnancy is associated with an increased risk of birth defects, with emphasis on cardiovascular birth defects even when accounting for lifestyle or other familial confounding.
Design Multicountry population based cohort study, including sibling controlled design.
Setting Nordic population (Denmark, Finland, Iceland, Norway, and Sweden) identified from nationwide health registers at different periods in 1996-2010.
Population The full study cohort included women giving birth to 2.3 million live singletons. The sibling cohort included 2288 singleton live births. The sibling controlled analyses included sibling pairs who were discordant for exposure to SSRIs or venlafaxine and birth defects.
Main outcome measure Prevalence of birth defects, including subtypes of cardiac defects. Odds ratio of birth defects from logistic and conditional logistic regression.
Results Among 36 772 infants exposed to any SSRI in early pregnancy, 3.7% (n=1357) had a birth defect compared with 3.1% of 2 266 875 unexposed infants, yielding a covariate adjusted odds ratio of 1.13 (95% confidence interval 1.06 to 1.20). In the sibling controlled analysis the adjusted odds ratio decreased to 1.06 (0.91 to 1.24). The odds ratios for any cardiac birth defect with use of any SSRI or venlafaxine were 1.15 (95% confidence interval 1.05 to 1.26) in the covariate adjusted analysis and 0.92 (0.72 to 1.17) in the sibling controlled analysis. For atrial and ventricular septal defects the covariate adjusted odds ratio was 1.17 (1.05 to 1.31). Exposure to any SSRI or venlafaxine increased the prevalence of right ventricular outflow tract obstruction defects, with a covariate adjusted odds ratio of 1.48 (1.15 to 1.89). In the sibling controlled analysis the adjusted odds ratio decreased to 0.56 (0.21 to 1.49) for any exposure to SSRIs or venlafaxine and right ventricular outflow tract obstruction defects.
Conclusions In this large Nordic study no substantial increase was found in prevalence of overall cardiac birth defects among infants exposed to SSRIs or venlafaxine in utero. Although the prevalence of septal defects and right ventricular outflow tract defects was higher in exposed infants, the lack of an association in the sibling controlled analyses points against a teratogenic effect of these drugs.
Introduction
Depression is common in pregnancy.1 Selective serotonin reuptake inhibitors (SSRIs) are the most frequently used antidepressants in pregnant women, with as many as 3% of such women in Europe and 4-10% in North America receiving these drugs.2 3 4 5 6
The results of previous studies assessing the risk of birth defects after use of SSRIs in pregnancy have been conflicting.7 Most consistently reported were cardiovascular birth defects.8 9 10 11 12 13 14 15 One study16 found an increased risk of cardiovascular defects with combined use of SSRIs or venlafaxine and benzodiazepines. Increased risks of anal atresia,7 hypospadias,7 14 clubfoot,7 limb reduction defects,7 craniosynostosis,8 omphalocele,7 8 gastroschisis,8 and cystic kidneys17 have also been reported with use of SSRIs in early pregnancy, but less consistently. A few studies reported no increased risk of congenital birth defects associated with use of SSRIs in pregnancy.13 18 19
Venlafaxine is a serotonin-norepinephrine reuptake inhibitor used increasingly as an alternative to SSRIs.20 Recently, a case-control study from the United States, based on 77 exposed cases and 14 exposed controls, reported that use of venlafaxine in early pregnancy was associated with several types of birth defects, with odds ratios ranging from 1.5 to 6.3.21
Limitations of previous studies include uncertain information on drug use, recall bias from self reports, limited information on confounding factors, and low statistical power. Larger studies are necessary for more definitive conclusions about particular types of birth defects and associations with specific drugs, rather than classes of drugs.22
The Nordic countries, representing a total population of about 26 million people, have similar nationwide registers of births and dispensed drugs, enabling large studies on the effects of rare drug exposures during pregnancy on birth defects.23 We performed a population based cohort study and a sibling controlled analysis within five Nordic countries to assess predefined and previously reported associations between exposure to individual SSRIs or venlafaxine in the first trimester and the risk of specific birth defects, with emphasis on cardiovascular defects, adjusting for important covariates such as familial factors.
Methods
Data sources and study population
In this population based study we included women from Denmark, Finland, Iceland, Norway, and Sweden who gave birth to a live singleton infant between 1996 and 2010. From nationwide health registers in each Nordic country we obtained data on births, dispensed drugs, birth defects, and potential confounders. These registers include prospectively collected health information on all inhabitants. A civil personal registration number is assigned to each resident at birth or immigration, enabling data linkage between the registers. Reporting to the registers is mandatory and regulated by national laws.
Each participating country contributed data for different periods corresponding to the availability of the prescription databases and other health registers. Accordingly we identified all live born singletons in Denmark 1997-2010, Finland 1996-2006, Iceland 2003-07, Norway 2005-10, and Sweden 2006-10. We also identified siblings born to the same mother during these periods.
Ascertainment of exposure
The Nordic prescription registers include data on dispensed drugs, substance, brand name, and formulation, together with date of dispensing.23 All drugs are classified according to the World Health Organization’s Anatomical Therapeutic Chemical (ATC) classification.24 The following SSRIs were included in the analyses: fluoxetine (ATC code: N06AB03), citalopram (N06AB04), paroxetine (N06AB05), sertraline (N06AB06), fluvoxamine (N06AB08), and escitalopram (N06AB10), and in addition venlafaxine (N06AX16). We considered infants to have been exposed in utero if they were born to women who filled a prescription for an SSRI from 30 days before the first day of the last menstrual period until the end of the first trimester (defined as 97 days after the last menstrual period).
Major birth defects
From the medical birth, patient, and malformation registers we retrieved data on maternal characteristics, the pregnancy and delivery, and major birth defects diagnosed within 365 days after birth. The patient registers record information on diagnoses and hospital visits.25 26 During the study period, birth defects were recorded according to the international classification of diseases, 10th revision (ICD-10) in Denmark, Norway, Sweden, and Iceland, whereas ICD-9-CM codes (Atlanta modification for birth defects) were used in Finland (see appendix 1 on bmj.com for ICD codes).
We categorised cardiovascular birth defects into any cardiac defects; situs anomalies and looping defects; conotruncal and major aortic arch anomalies; ventral septal defect or atrial septal defect; atrioventricular septal defects; right ventricular outflow tract obstruction defects; and left ventricular outflow tract obstruction defects. In addition we assessed several specific birth defects based on results from previous studies8 9 15 17: anal atresia, hypospadias, clubfoot, limb reduction defects, craniosynostosis, omphalocele, gastroschisis, and cystic kidneys.
Potential confounding factors
We included the potential confounders of country of residence, maternal age at delivery, calendar year of delivery, birth order, maternal smoking during pregnancy, maternal diabetes, and concurrent drug use. The presence of maternal diabetes was defined as dispensed antidiabetic drugs (ATC code: A10) from 90 days before the first day of the last menstrual period to 97 days after the last menstrual period. Concurrent drugs considered as confounders included antiepileptics (N03), anxiolytics and hypnotics (N05B, N05C), and agents acting on the renin-angiotensin system (C09) dispensed from 30 days before the first day of the last menstrual period until 97 days after the last menstrual period.
Statistical analyses
We used logistic regression analysis to estimate odds ratios with 95% confidence intervals for all major and specific types of birth defects according to exposure status, with adjustment for the included confounders. Owing to missing data on confounders, the number included in the adjusted analyses (n=2 145 050) was slightly lower than the number included in the crude analyses (n=2 303 647). In our primary analyses we assessed odds ratios for birth defects by exposure in early pregnancy to any SSRI and venlafaxine and to each specific SSRI or venlafaxine. In each instance the reference group comprised births of infants not exposed to any antidepressant (ATC code N06A) in utero. We present only the results from analyses with more than five births among exposed infants with the specific defect or defect group.
To adjust further for potential confounding from family related factors, we conducted sibling controlled analyses by restricting the study population to women with at least two children in the dataset. Furthermore, we restricted the sibling analyses to families with siblings who were discordant for both exposure and outcome. Using conditional logistic regression we compared the prevalence of birth defects overall, any cardiac defects, and right ventricular outflow tract obstruction defects in infants exposed to any SSRI and venlafaxine with the prevalence in siblings not exposed to any antidepressants.
Predefined sensitivity analyses were performed for a shorter and a longer period of exposure—that is, dispensed drugs from the first day of the last menstrual period until 97 days after the last menstrual period and from 90 days before the first day of the last menstrual period until 97 days after the last menstrual period, respectively. In addition we conducted secondary multivariable analyses stratified by use of anxiolytics and hypnotics. Finally, to account for confounding by severity of underlying psychiatric condition, we restricted the primary analyses to pregnant women without a previous hospital admission for a psychiatric condition.
All analyses were conducted using SAS software, version 9.3 (SAS Institute, Cary, NC). The study was approved and performed according to ethical and legal requirements in each country.23
Patient involvement
There was no patient involvement in this study.
Results
The full study cohort included 2 303 647 singleton live births and the sibling cohort included 2288 singleton live births. In the full study cohort, 36 772 (1.6%) infants were exposed to a selective serotonin reuptake inhibitor (SSRI) or venlafaxine during the first trimester in 1996-2010. The proportion of infants exposed to an SSRI or venlafaxine increased during the study period: from 0.6% in 1996-2000 to 1.5% in 2001-05 and 2.2% in 2006-10. Table 1⇓ presents the characteristics of the full study cohort and the sibling cohort according to drug exposure status. Citalopram and sertraline were the most commonly used SSRIs (table 2⇓).
Maternal and infant characteristics by exposure to selective serotonin reuptake inhibitors (SSRIs) or venlafaxine during first trimester*
Exposure to antidepressants during first trimester
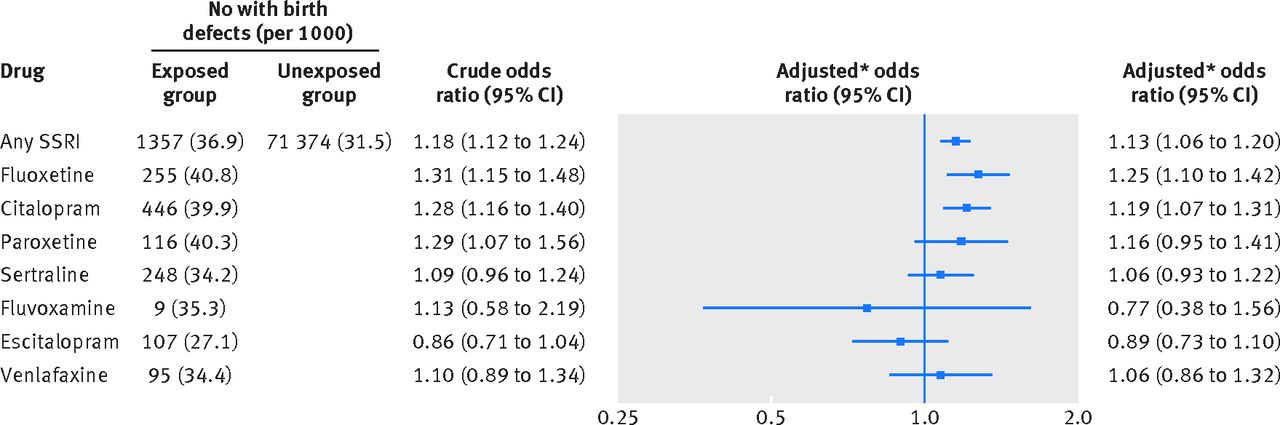
Among the 36 772 infants exposed to SSRIs or venlafaxine during the first trimester, 1357 (3.7%) had a diagnosis of a major birth defect compared with 71 374 (3.2%) of the 2 266 875 unexposed infants (adjusted odds ratio 1.13, 95% confidence interval 1.06 to 1.20, fig 1⇓).

Fig 1 Selective serotonin reuptake inhibitors (SSRIs) or venlafaxine in early pregnancy and risk of birth defects. *Adjusted for maternal age, year of birth, birth order, smoking, maternal diabetes, country, and use of other prescribed drugs (antiepileptics (ATC code N03), anxiolytics and hypnotics (N05B and N05C), and angiotensin converting enzyme inhibitors (C09))
{kind=link}
The prevalence of overall cardiac birth defects was 1.5% among infants exposed to any SSRI or venlafaxine compared with 1.2% among infants in the unexposed group (1.15, 1.05 to 1.26). Apart from escitalopram, in utero exposure to each specific SSRI and to venlafaxine was associated with an increased prevalence of cardiac birth defects, with adjusted odds ratios between 1.13 and 1.34. Similarly, and except for escitalopram, atrial or ventricular septal defects were positively associated with maternal use of each specific SSRI and with venlafaxine (fig 2⇓).

Fig 2 Selective serotonin reuptake inhibitors (SSRIs) or venlafaxine in early pregnancy and risk of cardiac birth defects. *Adjusted for maternal age, year of birth, birth order, smoking, maternal diabetes, country, and use of other prescribed drugs (antiepileptics (ATC code N03), anxiolytics and hypnotics (N05B and N05C), and angiotensin converting enzyme inhibitors (C09))
{kind=link}
The adjusted odds ratio for right ventricular outflow tract obstruction defects after exposure to any SSRI was 1.48 (1.15 to 1.89), with estimates for specific SSRIs varying from 1.40 to 2.54 (fig 2). Use of paroxetine was associated with an increased prevalence of conotruncal and major arch anomalies (2.27, 1.01 to 5.07), whereas associations with other SSRIs were less clear.
The prevalence of clubfoot and omphalocele was increased after exposure to any SSRIs, but we found no increased prevalence of hypospadias, limb reduction, craniosynostosis, gastroschisis, or cystic kidneys (fig 3⇓). Exposure to citalopram and sertraline were both associated with an increased prevalence of clubfoot, and sertraline also with anal atresia.

Fig 3 Selective serotonin reuptake inhibitors (SSRIs) or venlafaxine in early pregnancy and risk of non-cardiac birth defects. *Adjusted for maternal age, year of birth, birth order, smoking, maternal diabetes, and country, and use of other prescribed drugs (antiepileptics (ATC code N03), anxiolytics and hypnotics (N05B and N05C), and angiotensin converting enzyme inhibitors (C09))
{kind=link}
In the sibling controlled analyses we identified 895 families with at least one exposed pregnancy and at least one birth with a malformation (tables 1 and 3⇓). The adjusted odds ratios in the sibling controlled analyses were attenuated compared with estimates from the covariable adjusted analyses in the full cohort. The confidence intervals were also wider in the sibling controlled analyses.
Selective serotonin reuptake inhibitors or venlafaxine in early pregnancy and birth defects. Odds ratios in unmatched and sibling controlled analyses
The level of the odds ratios was not influenced by the order of exposure and outcome between the discordant siblings—that is, a first exposed sibling with a birth defect and an unexposed second sibling without a birth defect would yield odds ratios similar to a first unexposed sibling with no birth defects and a second exposed sibling with a birth defect.
In the predefined sensitivity analyses, using two different time windows for exposure, the effect estimates for birth defects associated with any SSRI were similar to those in the primary analyses. Stratification according to use of anxiolytics and hypnotics did not result in substantial variation of risk estimates between strata. The estimates were not substantially changed by restricting the primary analyses to women without previous admissions to hospital for psychiatric disorders (data not shown).
Discussion
In this large multinational population based study including over 2.3 million births from the Nordic countries, exposure to selective serotonin reuptake inhibitors (SSRIs) in utero was associated with a 13% increased prevalence of major birth defects and a 15% increased prevalence of cardiac defects in a covariate controlled analysis. However, we found no increased prevalence in the sibling controlled analyses, suggesting that the small observed increased risk when including mothers and their infants in the analyses could be explained by familial related factors or other lifestyle related factors not adjusted for. Similarly, each specific SSRI increased the prevalence of right ventricular outflow tract obstruction defects, with adjusted odds ratios ranging from 1.40 to 2.54, whereas no association was found in the sibling controlled analysis (0.71, 0.28 to 1.78). No significant association was found between venlafaxine and birth defects.
Comparisons with other studies
Some of the births in our study have been included in previous national studies.11 12 15 27 The observed increased prevalence of overall major birth defects in association with exposure to SSRIs was lower than the 21-30% increased risk reported in previous Danish studies,11 12 27 but extends the findings from a previous Finnish study reporting no substantial increased risk of overall birth defects.15 In our data, SSRI use was associated with an increased prevalence of cardiovascular defects; mainly driven by a 30% increase after exposure to paroxetine or fluoxetine, which is an effect of similar size to that reported from databases in the United Kingdom18 and the United States.8 Previous studies reporting risks of birth defects in association with the combined use of SSRIs and benzodiazepines included small numbers of exposed infants, with ambiguous findings.16 28 Our study showed no increased risk of birth defects with combined use of these drugs.
Our estimated 45% increased prevalence of septal defects associated with exposure to fluoxetine is an extension of the previous findings from Denmark11 12 and Finland.15 In contrast, one study8 reported no association between maternal use of fluoxetine and septal defects (adjusted odds ratio 1.0, 95% confidence interval 0.5 to 2.2), but given the lack of precision, those estimates may well have been in line with our findings. In our data, exposure to paroxetine was associated with a nearly 40% increased prevalence of septal defects, which contrasts with previous findings from Denmark,11 12 Finland,15 and the USA,8 but is in accordance with findings from the Netherlands (adjusted odds ratio 1.6, 95% confidence interval 0.4 to 5.6).29 However, the estimated effect of sertraline on septal defects in our data does not support previous findings from Denmark11 12 and the USA,8 reporting a twofold to threefold increased prevalence of septal defects in offspring exposed to sertraline. We found exposure to all types of SSRI to be associated with an increased prevalence of right ventricular outflow tract obstructions, which is an extension of the previously reported findings from Finland15 and consistent with findings from earlier studies from the USA.8 9 However, two recent cohort studies from the USA and the UK, respectively, suggested no substantial increase in the risk of cardiac birth defects associated with use of antidepressants during the first trimester.30 31 These findings are in accordance with our estimates when controlling for confounding by a sibling controlled design.
When we examined other specific birth defects reported in previous studies, we did not find an increased prevalence of hypospadias, limb reductions, gastroschisis, cystic kidneys, or craniosynostosis. One study8 reported a fivefold increased prevalence of omphalocele associated with sertraline. We found a twofold increased prevalence of omphalocele in infants exposed to SSRIs, but this estimate was based on only 10 cases. In our data, exposure to sertraline was associated with a 2.5-fold increased prevalence of anal atresia, corroborating but lower than the 3-4-fold increased odds previously estimated.8 With a prevalence of 0.5 per 1000 in SSRI exposed infants, the estimated absolute increase of anal atresia was low in our study.
Contrary to our results, a recent case-control study found positive associations between prenatal exposure to venlafaxine and various birth defects, including cardiac defects.21 The findings may, however, have been complicated by methodological limitations, including the small numbers included and a study design susceptible to recall bias.
Mechanism
Biological mechanisms remain unknown for most drug-defect associations, but a growing body of evidence from animal studies has suggested that the neurotransmitter serotonin is important as a signaling molecule in a variety of cells and tissues during embryogenesis, including heart development.32 Disruption of the serotonin signaling caused by exposure to SSRIs may thus result in disturbances of cardiac development, providing a biologically plausible explanation for the increased risk of cardiac birth defects.32 33 34
Strengths and limitations of this study
Our study was based on prospectively collected data from five Nordic countries, and the large numbers allowed us to study individual SSRIs and specific birth defects with independent ascertainment of exposure and outcome up to 1 year of age without any risk of recall bias. None the less, non-adherence to the dispensed antidepressants may have yielded misclassification of exposure and thus biased the relative estimates towards the null. However, previous Nordic studies comparing data on use of SSRIs from prescription databases with self reported SSRI use in pregnant women indicate the prescription data to be quite accurate and reliable for regular use of drugs such as antidepressants.35 36 37
Although we had data on several important confounders, including maternal age, diabetes, use of other potentially teratogenic drugs, and self reported smoking, residual confounding cannot be ruled out. By using dispensed drugs as a proxy for diabetes we may have missed those women with untreated diabetes type 2. A Danish cross sectional study based on a population survey found that women with an unhealthy lifestyle were about 1.5-fold more likely to be current users of SSRIs than those with a healthy lifestyle.38 We were unable to include information on maternal use of alcohol or other lifestyle factors in our study. These factors may, however, be correlated with smoking. Thus adjusting for smoking may at least partly have controlled for some of the effect. Still, we find it likely that our estimates would have been even closer to 1.0 if we had been able to better control for lifestyle factors. This is further corroborated by our findings in the sibling controlled design. To use a sibling design when both exposure and outcome are rare, a large study population is required. Even though our study included 2.3 million births, the number in the sibling cohort was moderate. The sibling design has the advantage of controlling for familial factors that may be difficult to measure and control for in more conventional analyses. But sibling analyses reduce the size of the study population, since only sibling pairs discordant for both exposure and outcome are informative and contribute to the effect estimate. These births may represent a selected part of the population. Moreover, the sibling analysis has lower statistical power than the conventional cohort study design. Yet the upper limits of the confidence intervals were similar in the sibling analyses and the covariate adjusted cohort analyses. A possible weakness of the sibling design could be that use of SSRIs in a later pregnancy is not independent of the outcome of a first exposed pregnancy. However, in this study the order of exposure and outcome between discordant siblings did not influence the level of the odds ratios, which would suggest no such bias.
We tested several associations, but all the analyses were based on a priori stated hypotheses, which were built on previously published findings. As the number of tests in a study increases, the probability that one of them will be falsely positive also increases. We did not, however, adjust for multiple testing as this may increase the risk of type 2 errors.39 Considering lower statistical precision in the sibling controlled analyses, we focused on the major outcomes in these analyses, such as any birth defect, any cardiac defect, and right ventricular outflow tract obstruction defects.
Disentangling the potential teratogenicity of SSRIs from a potential effect of the underlying depression remains a challenge. We lacked information on severity of depression. We presumed, however, that women who had a previous hospital admission for a psychiatric disorder had more severe depression than women with no such admission. Restricting the analyses to women without previous hospital contacts for psychiatric disorders did not substantially change our relative estimates. Yet severity of the underlying illness may still vary substantially within this group of women.
We used population based data on live births, but we lacked information about prenatal diagnosis resulting in termination of pregnancy, miscarriages, or stillbirths caused by birth defects. If use of SSRIs is related to any of these outcomes, selection bias could be present. This may have led us to underestimate the association between use of SSRIs and birth defects. However, in an earlier study based on the same registers, no significant associations were found between use of SSRIs during pregnancy and risk of stillbirth or infant mortality.26 In addition there seems to be no association between use of antidepressants and late termination of pregnancy.40 Data on birth defects were obtained from medical registers, and previous validation studies suggest high validity of these diagnoses, with misclassification rates of 12% for both congenital malformations overall and cardiac defects.41 42 We cannot, however, rule out that increased awareness of the potential for cardiac defects in infants exposed to SSRIs prenatally may have introduced surveillance bias and thereby inflated our relative estimates. Such bias would particularly concern less serious cardiac defects, such as ventricular septal defects, which often remain undiagnosed in infancy. We would, however, expect such differential misclassification to be of similar magnitude between the different types of SSRIs. Furthermore, the fact that we found no increased risk of cardiac defects in infants exposed to escitalopram argues against substantial surveillance bias. The risks of channeling bias are probably small considering similar pregnant populations and that prescription patterns of SSRIs to pregnant women differ somewhat between the Nordic countries—for example, citalopram and fluoxetine are the most prescribed SSRIs in Denmark, whereas citalopram and escitalopram are most prescribed in Norway.12 43 We also have to consider that women who continue to use antidepressants in pregnancy may differ from those who were never prescribed antidepressants and those who stopped using antidepressants in pregnancy. Pregnancy is a major determinant of cessation of antidepressant treatment, which may be explained by concerns about potential adverse effects of the drugs.44
Conclusions
Taken together, the results from our covariate adjusted analyses and the sibling controlled analyses point against a substantial teratogenic effect of SSRIs. Our analyses did not suggest a teratogenic effect of venlafaxine either.
What is already known on this topic
The teratogenicity of individual selective serotonin reuptake inhibitors (SSRIs) and venlafaxine remains controversial
Few studies have had sufficient power to study the direct effect of individual SSRIs on specific birth defects
What this study adds
In this large population based cohort study including sibling controlled analyses, there was no substantial increase in prevalence of overall cardiac birth defects among infants exposed to SSRIs or venlafaxine in utero
Although the prevalence of right ventricular outflow tract defects was higher in exposed infants in the full cohort, no association was found in the sibling controlled analyses
The general absence of strong associations between birth defects and SSRIs and venlafaxine is reassuring
Notes
Cite this as: BMJ 2015;350:h1798
Footnotes
We thank Gunnar Bergman (Department of Women’s and Children’s Health, Karolinska Institutet) for help with classifying the cardiovascular birth defects.
Contributors: KF, BH, HK, and MN conceived and designed the study. BH, MG, MA, AE, MN, and UAV acquired the data in their respective countries. KF and MN drafted the manuscript. HK obtained funding and supervised the study. BH was responsible for the statistical analyses. All authors participated in interpretation of data and critical revision of the manuscript. KF and BH had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analyses. They are the guarantors.
Funding: This study was funded by the authors’ affiliations and the Swedish pharmacy company Apoteksbolaget. Apoteksbolaget had no role in the design and conduct of the study; the collection, management, analysis, and interpretation of the data; the preparation, review, or approval of the manuscript; or the decision to submit the manuscript for publication.
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Ethical approval: This study was approved by the regional ethical review board at Karolinska Institutet in Stockholm, Sweden (No 2008/1371-31/4); the Danish Data Protection Agency, Denmark; the National Institute for Health and Welfare (THL), the Social Insurance Institution of Finland and Statistics Finland, Finland; the National Bioethics Committee and the Data Protection Authority in Iceland, Iceland; and the Norwegian Data Inspectorate, Norway.
Data sharing: No additional data available.
Transparency: The lead authors (KF and MN) affirm that the manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.