Article Text

Abstract
The evolution of abnormal albumin excretion and its association with suggested risk factors were studied in 233 children with insulin dependent diabetes mellitus (IDDM) attending a single paediatric diabetic clinic over an eight year period. Yearly albumin:creatinine ratios (ACR; measured in mg/mmol) in early morning urine samples, glycated haemoglobin (HbA1c), and blood pressure were recorded. Thirty four (14.5%) children had a persistently raised ACR (ACR ⩾ 2.5 mg/mmol on at least three consecutive occasions) and 21 (9%) had an intermittently raised ACR (ACR ⩾ 2.5 mg/mmol on at least two occasions). Factors associated with a persistently raised ACR compared with normal albuminuria in IDDM included longer duration of diabetes, raised median HbA1c during the first five years after diagnosis, and final age adjusted systolic and diastolic blood pressure represented as standard deviation scores. The onset of persistently raised ACR in 13 of 34 children was before puberty and in 23 of 34 children it was within the first four years of diagnosis. The cross sectional prevalence of raised ACR was 12.9% at one year, 18.3% at five years, and 33% at 10 years after diagnosis. Raised ACR occurs frequently before puberty and in the early stages of childhood diabetes.
-
The cumulative prevalence of persistently raised albumin:creatinine ratios over 8.5 years was 14.5%.
-
The onset of persistent microalbuminuria may occur before puberty and during the first four years after diagnosis.
-
Persistent microalbuminuria was associated with increasing duration of diabetes, poorer glycaemic control, and increased blood pressure.
-
We recommend the routine monitoring of albumin:creatinine ratios in early morning urine in all children with insulin dependent diabetes.
- microalbuminuria
- insulin dependent diabetes mellitus
- screening
Statistics from Altmetric.com
Studies in adults with insulin dependent diabetes mellitus (IDDM) have shown that persistent microalbuminuria (albumin excretion rate (AER) 20–200 μg/minute), identified by screening, predicts the development of overt nephropathy,1-3 which can progress to end stage renal failure requiring dialysis and transplantation.4 With increasing albumin excretion there is also an increase in other microvascular complications including proliferative retinopathy.5 6
Estimates of the point prevalence of microalbuminuria in childhood vary between 7% and 20%.7-10 This variation reflects differences in definitions of microalbuminuria and mean age of study populations. Furthermore, these were not longitudinal studies and cannot comment on the cumulative prevalence of persistent microalbuminuria. In a single longitudinal study, following 156 children with IDDM over 15 years, 25% of children below the age of 21 years developed microalbuminuria within 14 years of diagnosis.11
Reported risk factors for the development of diabetic renal disease include a longer duration of IDDM, an earlier age at diagnosis, onset of puberty, poorer glycaemic control during the first five years of diabetes, smoking, and a family history of diabetic nephropathy.4 11-18 The role of a family history of hypertension as a risk factor remains controversial.19 20
We report a longitudinal evaluation of urinary albumin excretion in children with IDDM, attending a single clinic, over a period of eight years. We assessed associations between raised urinary albumin excretion and age at disease onset, duration of diabetes, pubertal status, glycaemic control, and blood pressure. An understanding of the development and progression of increased albumin excretion in childhood IDDM can guide the development of screening practices, and might have implications for these patients during adulthood.
Methods
PATIENTS
All children and adolescents still attending the diabetic clinic at Alder Hey Children’s Hospital, Liverpool between January 1993 and June 1994 were included in the study. All children with IDDM in the Liverpool area are seen in this clinic and are managed by one endocrinologist (CS). Information was collected on this unselected population from January 1986 to June 1994 by case record review.
There were 233 children of whom 114 (49%) were boys. The median duration of IDDM was 3.9 years, (interquartile range (IQR), 1.8–6.7) and the median age at onset of diabetes was 7.7 years, (IQR, 4.1–11.2).
MEASUREMENTS
Urinary albumin:creatinine ratio (ACR), blood pressure, glycated haemoglobin, and pubertal status were recorded as part of the clinical assessment at each appointment and the annual measurements were analysed.
An early morning urine sample was collected as part of each routine clinical assessment. Urinary albumin was measured by rate nephelometry (Beckman Instruments UK Ltd, High Wycombe, Bucks, UK). Urinary creatinine was measured using the modified Jaffe reaction. Results are expressed as the ratio of albumin to creatinine (mg/mmol). The overall coefficient of variation for ACR is 2.03%. Urine microscopy and bacteriological culture were performed on all samples with detectable proteinuria on dipstix, and the ACR result was discarded if the culture was positive. Urine samples were not collected from pubertal girls during menses and any sample with haematuria was excluded from the results.
ACR was used as a measure of urinary albumin excretion and was considered raised if it was ⩾ 2.5 mg/mmol. Persistently raised urinary albumin excretion is defined as an ACR ⩾ 2.5 mg/mmol on at least three consecutive occasions.21 Children with diabetes for only two years with an ACR ⩾ 2.5 mg/mmol at onset, one year and two years duration of diabetes were also classified as having a persistently raised ACR.
Intermittently raised urinary albumin excretion is defined as an ACR ⩾ 2.5 mg/mmol on at least two occasions. Children were considered to have normal albumin excretion if their ACR remained < 2.5 mg/mmol.21
Glycated haemoglobin was measured from January 1991 as haemoglobin A1c (HbA1c) using column chromatography. (Bio-Rad Haemoglobin A1c Mini Column Test; Biorad Laboratories Ltd, Hemel Hampstead, Hertfordshire, UK). The normal range for HbA1c in our laboratory in a non-diabetic population is 3.4–6.4%. The imprecision measured as the coefficient of variation was 15.8% at an HbA1c of 4.6% and 4.1% at an HbA1c of 10.2%.
Blood pressure was measured manually by mercury sphygmomanometer with an appropriate paediatric cuff. Diastolic blood pressure was defined as Korotkoff level IV. To correct for age and sex, measurements are expressed as a standard deviation score related to the 1987 Task Force data for blood pressure in normal children.22 Pubertal status was measured by Tanner staging.
STATISTICS
The data were analysed using the Minitab statistics package. Differences between the groups were evaluated by the Mann-Whitney U test and comparisons of sex by the χ2 test for categorical variables. Differences were considered significant when p < 0.05.
Results
Throughout the study period, 172 (73.8%) children had normal albumin excretion. Thirty four (14.6%) children had a persistently raised ACR and 27 (11.6%) children had an intermittently raised ACR.
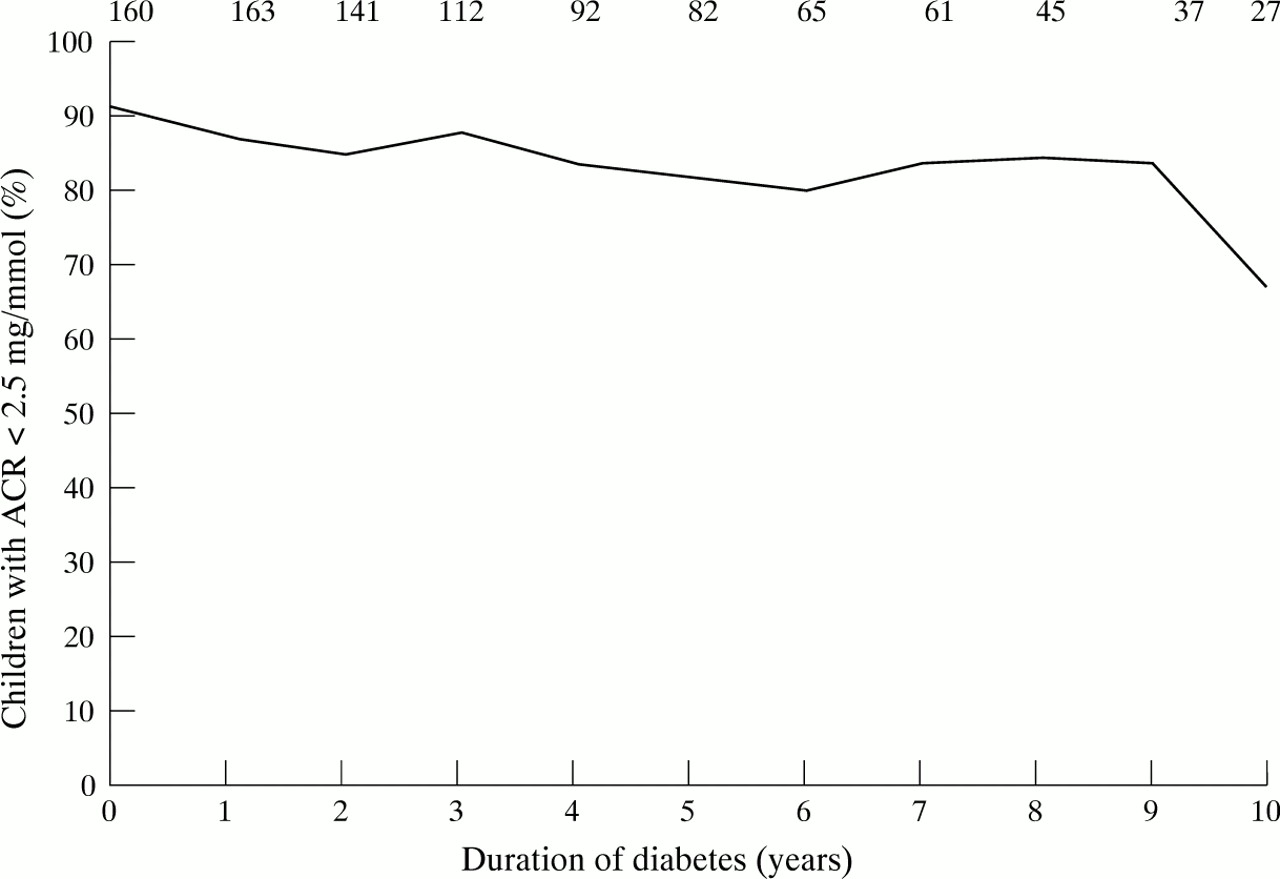
Figure 1 shows the percentage of children with an ACR < 2.5 mg/mmol at a particular duration of diabetes from which the point prevalence of a raised ACR can be calculated. At the onset of the study, 64 patients already had established IDDM, so that ACR from the onset of their disease is not available. However, clinical details from their subsequent course during the period studied is included, thus extending data available on IDDM to 10 years duration.
{kind=link}
Prevalence of children with an albumin:creatinine ratio (ACR) < 2.5 mg/mmol. Numbers at top are numbers of children.
There was an increase in the percentage of children who had an ACR ⩾ 2.5 mg/mmol at one year following diagnosis (12.9%), at five years after diagnosis (18.3%), and at 10 years (33%) after diagnosis, indicating a progressive increase in the prevalence of a raised ACR with duration of diabetes in our population.
In 24 of the 34 children with a persistently raised ACR, it remained stable throughout the period studied. However, in 10 children it increased progressively. In eight of these, the rise in ACR, over a minimum period of three years, varied from 18% to 78% each year from onset of a persistently raised ACR. In the other two children with IDDM for only two years, ACR increased in one year by 74% and 1121%. The median time to the onset of a persistently raised ACR was 48 months (IQR, 20–72). Seven patients with a persistently raised ACR had episodes of ACR > 45.5 mg/mmol, indicating macroalbuminuria.23 One patient had an ACR that was persistently > 45.5 mg/mmol throughout the study period.
The onset of a persistently raised ACR occurred in 13 children before puberty.
A comparison of clinical features in children with normal albumin excretion and those with persistently raised ACR is shown in table 1. There is no significant difference between the two groups in age at diagnosis. There is a significant difference between the two groups with respect to the age of the children at the end of the study (p < 0.001). However, the older age in children with persistently raised ACR at completion of the study reflects the longer duration of diabetes in this group (7.2 v 3.3 years; p = 0.002). There is a significantly greater proportion of girls with persistently raised ACR (p = 0.0014). The median HbA1c in the first five years after diagnosis was significantly higher in children with a persistently raised ACR (p = 0.033).
Median and IQR of children with persistently raised ACR and normal ACR
A comparison of clinical features in children with normal ACR and an intermittently raised ACR is shown in table 2. Again, this shows older age in children with intermittently raised ACR at the end of the study (p < 0.01) and poorer glycaemic control during the first five years after diagnosis (p < 0.01) in this group.
Median and IQR for children with intermittently raised ACR and normal ACR
The standard deviation scores (SDS) for systolic and diastolic blood pressure for the children with normal albumin excretion, with persistently raised ACR, and with intermittently raised ACR are shown in table 3. There is no significant difference in the SDS for both systolic and diastolic blood pressures between the normal albumin excretion group and either of the other two groups at the onset of diabetes. There is a significantly higher SDS for systolic blood pressure (median: 0.91; IQR: 0.06, 0.99) at the final measurement in the group with a persistently raised ACR compared with those with normal albumin excretion (median: 0.29; IQR: −0.21, 0.77; p = 0.026) and with those with intermittently raised ACR (median: 0.56; IQR: 0.17, 1.01; p < 0.001). There is a significantly higher final SDS diastolic blood pressure in those with persistently raised ACR (median, 0.9; IQR, 0.47, 1.2) compared with those with normal albumin excretion (median: 0.35; IQR: −0.19, 0.69; p < 0.001). There was also a significantly higher final SDS diastolic blood pressure in the group with intermittently raised ACR (median: 0.91; IQR: 0.48, 1.35; p < 0.001) than those with normal albumin excretion.
Median and IQR for systolic and diastolic blood pressure SDS at the onset of diabetes and at the end of the study period
A significant increase in systolic blood pressure SDS was found for diabetic groups with both intermittent or persistently raised ACR from the onset of diabetes to the final measurement (persistently raised ACR, p = 0.01; intermittently raised ACR, p = 0.01). There was also an increase in systolic blood pressure SDS for children with normal albumin excretion. (p = 0.05) A significant increase for diastolic blood pressure SDS from the onset of diabetes to the final measurement was found only in the group with a persistently raised ACR (p < 0.01).
Discussion
Persistent microalbuminuria with an AER of 20–200 μg/minute is predictive of nephropathy in adults with IDDM,1-4 and has led to the development of screening programmes and intervention studies.24-27 There is limited information on the evolution of urinary albumin excretion from the onset of IDDM in a childhood population. Most studies have been cross sectional in design, reporting a point prevalence of 7–20% for microalbuminuria, and by their nature unable to evaluate the prevalence of persistent microalbuminuria.7-10 A single longitudinal study of 156 children reported a cumulative prevalence of 25% for microalbuminuria within 14 years of diagnosis of IDDM.11 Variability in the estimates of prevalence can also be affected by differences in measurements used to define microalbuminuria.
The definition of microalbuminuria according to timed AER has been useful in describing accurately the natural history of renal dysfunction in adult IDDM groups. However, in a routine clinic setting and particularly with a paediatric population, the acceptability, practicality, and reliability of regular 24 hour or timed overnight urine collections is reduced. This is especially true if the child is enuretic or where poor compliance is expected. The ACR of early morning urine samples is useful as a surrogate measure for AER, with variation in the sensitivity and specificity according to the defining level of ACR chosen.28-30 An ACR ⩾ 2.5 mg/mmol in children had both a sensitivity and specificity of 94% with a positive predictive value of 66% for microalbuminuria using established definitions based on timed collections.31
In selecting a defining value, account should also be taken of the lower urinary albumin excretion seen in normal children compared with normal adults and the increase seen with age.32 33Using the ACR of early morning urine samples, an upper limit of 1.17 mg/mmol was found in a population of normal British children.8 Using an ACR ⩾ 2.5 mg/mmol as the defining value for an increased albumin excretion, and using established definitions for persistence and progression of micromicroalbuminuria,1-3 21 we describe our observations in a population of 233 children with IDDM followed longitudinally over an eight year period.
A cumulative prevalence of 14.5% with a persistently raised ACR over 8.5 years compares with 11.5% at 7.5 years in the only longitudinal study of urinary albumin excretion in childhood IDDM.11Within 14 years of diagnosis, one quarter of this group developed microalbuminuria.
It is suggested that the progression of microalbuminuria in childhood is low.34 In 10 children with a persistently raised ACR, we report a progressive increase in their albumin excretion. Adult studies indicate that these patients are at greater risk of overt nephropathy.35 Seven patients with a persistently raised ACR had, on occasions, an ACR above 45.5 mg/mmol and one patient had an ACR that was persistently greater than 45.5 mg/mmol. This value indicates nephropathy and corresponds to a urinary albumin excretion equivalent to 300 μg/minute, which is albustix positive. Adult patients with diabetic nephropathy have a progressive decline in glomerular filtration rate and ∼ 50% of untreated patients die within seven years from renal failure and cardiovascular disease.36 The prognosis of patients developing albustix positive proteinuria in childhood is not yet known.
Previous studies have indicated that the onset of microalbuminuria before puberty occurs only rarely and, consequently, screening for microalbuminuria should be recommended for children over 12 years of age.10 14 16 In a longitudinal study, three of 156 children developed persistent microalbuminuria at less than 12 years of age. However, pubertal staging of the children in that study was not discussed.11 In a further study, in which puberty was defined by age, the duration of diabetes before puberty was found to have little effect on microvascular disease.15 We have found that in 15 of 34 (44%) children with persistently raised ACR, onset was before puberty, as assessed by Tanner staging. This suggests that children with IDDM are at risk of developing increased albumin excretion before puberty and this would warrant regular screening. Whether these children carry the same risk for the progression of raised albumin excretion to the stage of overt nephropathy will require continued follow up of this group.
The association of increasing urinary albumin excretion in IDDM in childhood and the duration of disease has been demonstrated in some studies,7 11 37 but not in others.16 38 We found a clear increase in the cumulative prevalence of affected children with a raised ACR, and in those children with persistently raised ACR, a duration of IDDM of 7.2 years compared with only 3.3 years for normoalbuminuric children with diabetes. It is possible that further follow up might identify children in the normoalbuminuric group who later develop a raised ACR. Although there is increasing urinary albumin excretion with increasing disease duration, we also found that in 56% of children who developed a persistently raised ACR, its onset was within the first four years of their IDDM. These children represent 8% of the total study population, a figure equal to the percentage with early onset of persistent microalbuminuria in the other longitudinal study.11 If screening is to be undertaken, it would seem appropriate to introduce it from the early stages of disease onset.
The association between a persistently raised ACR and being a girl might reflect the finding of increased urinary albumin excretion in normal girls at all ages from 4 to 16 years.39 There was no significant difference in the duration of IDDM for both sexes. Although the girls had more episodes of diabetic ketoacidosis (data not shown), there was no difference in median HbA1c between girls and boys.
We confirm the association of persistently raised urinary albumin excretion with poorer glycaemic control early in disease.7 10 11 16 Improving glycaemic control might reduce the incidence of microalbuminuria in early IDDM.40The youngest patient in the diabetes control and complications trial was only 13 years. The risks of hypoglycaemia are increased with improved glycaemic control, which may be unacceptable in children. The intensive blood glucose monitoring and increased frequency of insulin injections are also impractical. The poorer early metabolic control in our group may explain the increase in prevalence of persistently raised urinary albumin excretion compared with the other longitudinal study11 (HbA1c values: mean (SD), 9.2% (1.4%)v 8.4% (1.3%), respectively).
An increase in blood pressure is associated with increases in urinary albumin excretion in both adults and children.16 41 There is controversy as to whether an increase in blood pressure precedes or is a result of the development of microalbuminuria.42Using routine clinic blood pressure measurements, we have found a significant increase in the SDS systolic blood pressure from onset to final blood pressure measurement for children with diabetes who had a persistently or intermittently raised ACR. However, diastolic blood pressure SDS was only raised significantly in children with a persistently raised ACR. In a comparison of children with and without raised ACR, at final measurement, the blood pressure SDS was significantly higher in the persistently raised ACR group for both systolic and diastolic measurements compared with the normoalbuminuric children with diabetes. There was no difference in blood pressure SDS between children with persistently raised ACR and normal albumin excretion at four years duration of diabetes. This time point represents the median time before the onset of persistent microalbuminuria. This suggests that the increase in blood pressure SDS observed in the children with a persistently raised ACR occurs in parallel with, or as a consequence of, microalbuminuria. This should be considered in decisions surrounding the use of anti-hypertensive agents in children with microalbuminurea who are still normotensive. Angiotensin converting enzyme (ACE) inhibitors reduce urinary albumin excretion in hypertensive and normotensive adults with diabetes and microalbuminuria, and reduce the incidence of nephropathy in normotensive patients with microalbuminuria.23-26 There are few data on the use of ACE inhibitors in childhood IDDM, although they have been shown to halt or reverse the progression of microalbuminuria in a small group of normotensive children with microalbuminuria.43
The clinical significance of intermittent microalbuminuria in childhood IDDM is unknown. Adults with diabetes who develop persistent microalbuminuria have an increased incidence of intermittent microalbuminuria before the onset of persistent microalbuminuria, and those with a greater number of episodes of intermittent microalbuminuria are more likely to develop persistent microalbuminuria.44 Twenty seven children in our population had an intermittently raised ACR. They were similar to the children with persistently raised ACR in that they were older at the end of the study period and had a higher HbA1c compared with the children with normal albumin excretion. They also had a significantly higher SDS for systolic and diastolic blood pressure at the end of the study period compared with children with normal albumin excretion.
We have shown that in an unselected population of children with diabetes, 14.5% developed persistently raised ACR, and of these, 10 increased progressively. Increasing duration of diabetes, poorer glycaemic control, and an increase in blood pressure were associated with this. The routine monitoring of children with IDDM using ACR on an early morning urine sample is a simple and reliable technique in clinical practice. It will enable the identification of groups at high risk of diabetic nephropathy. Monitoring should be extended to those in the early stages of the disease and those who are still prepubertal. Continued follow up of children with a stable but persistently raised ACR and those with an intermittently raised ACR will clarify whether they will follow a benign course or will progress ultimately to nephropathy. Diabetic children with a progressively increasing ACR should be considered for intervention studies.