Article Text

Abstract
It is thought that Helicobacter pyloriinfection may influence growth rate in children. The aim of this study was to evaluate the prevalence of H pylori infection in healthy Italian children, and to look for differences in height between infected and non-infected subjects. Two hundred and sixteen children, aged 3 to 14 years, were tested for H pylori infection by13C-urea breath test. Centile values for height were calculated. Composite indices for socioeconomic class and household crowding were also determined. Forty nine of 216 children (22.7%) wereH pylori positive. The prevalence of infection increased with age. Eight of 49 H pylori positive children (16.3%) were below the 25th centile for height, compared with 13 of 167 H pylori negative children (7.8%). This difference became significant in children aged 8.5 to 14 years; in this group (n = 127), eight of 31 infected children (25.8%) were below the 25th centile for height, compared with eight of 96 non-infected children (8.3%). A significant correlation was found between socioeconomic conditions, household crowding, and H pylori status. By using stepwise logistic regression, only the centile value for height was significantly related to H pylori status in older children. Thus H pylori infection was associated with growth delay in older children, poor socioeconomic conditions, and household overcrowding. This finding is consistent with the hypothesis that H pylori infection is one of the environmental factors capable of affecting growth.
- growth
- height
- Helicobacter pylori
- urea breath test
Statistics from Altmetric.com
Helicobacter pylori infection is a common chronic infection1 associated with chronic gastritis,2 gastric and duodenal ulcer,3 and probably gastric cancer.4 Once acquired, the infection lasts several decades, with a very low spontaneous eradication rate.H pylori is generally acquired early in life5and socioeconomic conditions are regarded as the most important risk factors for acquisition of the infection.6
Like other chronic diseases, H pylori infection might impair growth. Three studies have already shown a difference in height between infected and non-infected children. One study in the developing world detected H pylori infection mostly in poor children, and short stature appeared to be related to a low nutrient intake rather than to H pylori itself.7 A subsequent study from Europe showed that over half of children investigated for short stature were infected with H pylori.8However, no controls were considered. A Scottish study found thatH pylori infection was associated with growth delay only in girls around puberty.9
Common to all these studies, however, is a lack of information about the socioeconomic conditions which may affect height, as shown by the positive correlation between increasing height observed over past centuries and better living conditions in industrially developed societies.10 The exact mechanism of this association has not been completely elucidated but the gradual disappearance of chronic infections is a plausible explanation.11
The aim of our study was to look for differences in stature between infected and non-infected children, taking into account socioeconomic conditions and household crowding. The 13C-urea breath test12 was used for H pylori detection since it is easy to perform, non-invasive, and accurate in determining the presence of infection.
Methods
STUDY POPULATION
Between 1994 and 1995, a cross sectional study was carried out on all schoolchildren aged 3 to 14 years living in San Giovanni Rotondo (Italy). Subjects for the study were selected from the school register, after random stratified sampling with proportional allocation by age and sex. Before starting the study, a letter explaining its purpose was sent to all enrolees’ parents.
QUESTIONNAIRE
The letter contained a questionnaire which was designed to obtain demographic information on the parents, such as their date and place of birth, race, educational level, type of occupation, type of house, number of rooms, and number of people who lived in the house. Parents were also asked if their children had suffered from any relevant disease in the past or had been given antibiotics in the last month. A consent form was signed by all parents before participation in the study. The study protocol was approved by the ethics committee of ‘Casa Sollievo della Sofferenza’ Hospital in San Giovanni Rotondo.
METHODS OF ANALYSIS
We constructed a composite index for socioeconomic class based on parents’ occupation and education by applying the Hollingshead index.13 Five occupational categories and five educational levels were used for each parent (table 1). A score of 0 was given to the lowest level of education and occupation and a score of 4 was given to the highest. Four socioeconomic classes (from I to IV) were obtained on the basis of the sum of parents’ educational and occupational scores (table 1).
Socioeconomic class was obtained by scoring the educational and occupational levels of both parents. A score of 0 was given to parents with the lowest level of education and occupation. A score of 4 was given to parents with the highest level. Four socioeconomic classes (from I to IV) were obtained on the basis of the scores of parents’ educational and occupational levels
A crowding index was obtained by dividing the number of people living in the household by the number of rooms. Two classes were identified: class I had a crowding index less than 1 and class II greater than 1.
UREA BREATH TEST
Children were tested for H pylori infection by a13C-urea breath test,12 which was performed after an overnight fast. Each subject received the test meal consisting of 210 ml of milk and 75 mg of [13C] -urea (13C, 99%; Isotec, Ohio, USA). Breath samples were taken before and every 15 minutes after ingestion of the test meal for one hour. 13C enrichment in breath was determined by isotope ratio mass spectrometry (ANCA-NT, Europa Scientific, Crewe). The δ values were expressed in relation to the PDB international standard, after correction for the oxygen isotope effect.14Analytical data were expressed as percentages of13CO2 recovery of the administered dose per hour. The percentage of the cumulative dose of13CO2 at one hour (CD60) was calculated by trapezoidal rule. CO2 production was assumed to be 300 mmol/m2 of body surface area per hour.15 Body surface area was calculated using the weight–height formula of Haycocket al.16 The 13C-urea breath test was considered positive if the CD60 was ⩾ 1.2% (by using this cut off, sensitivity and specificity of the urea breath test are respectively 95% and 100%).17
HEIGHT AND WEIGHT MEASUREMENT
The standing height (cm) and the weight (kg) of each subject were recorded by the same experienced paediatrician (MP) who was unaware of the H pylori status of the children. Centile values of height and weight were calculated by using standard Italian height and weight charts. For statistical purposes, children were sorted into two groups, the 25th centile values for height or weight being the threshold values.
OTHER MEASUREMENTS
All children who were below the 25th centile value for height were evaluated for coeliac disease. IgG and IgA class antigliadin (AGA) and antiendomysial antibodies (EmA) were assayed by means of a commercial enzyme linked immunosorbent assay (ELISA) (Eurospital, Trieste, Italy).
STATISTICAL ANALYSES
Univariate statistical analysis was made by Student’st test and the χ2 test.18 A stepwise logistic regression analysis was carried out to evaluate the independent influence of each variable (centile value of height and weight, sex, socioeconomic class, and crowding class) on H pylori status.18
ANALYSIS OF NON-RESPONDERS
All non-responders were interviewed by telephone and reasons for non-response were recorded (classified as not willing to participate or uncertain about participating in the study). Information on demographic data and children’s height was obtained from the parents.
Results
The sample population consisted of 308 children. The response rate was 70% so the final sample studied was 216 subjects. We found no significant difference between responders and non-responders so far as socioeconomic or crowding indices and children’s height or weight were concerned.
Forty nine out of 216 children (22.7%) were infected with H pylori. No difference in sex between H pyloripositive and negative subjects was found. The prevalence rate of infection increased with age, from 0% in the youngest group (3–4 years) to 33% in the oldest group (13–14 years). Figure 1 shows the prevalence rate in the different age groups: a bimodal distribution is evident with two peaks of prevalence at 5 and 11 years.

Prevalence of H pylori infection in Italian children.
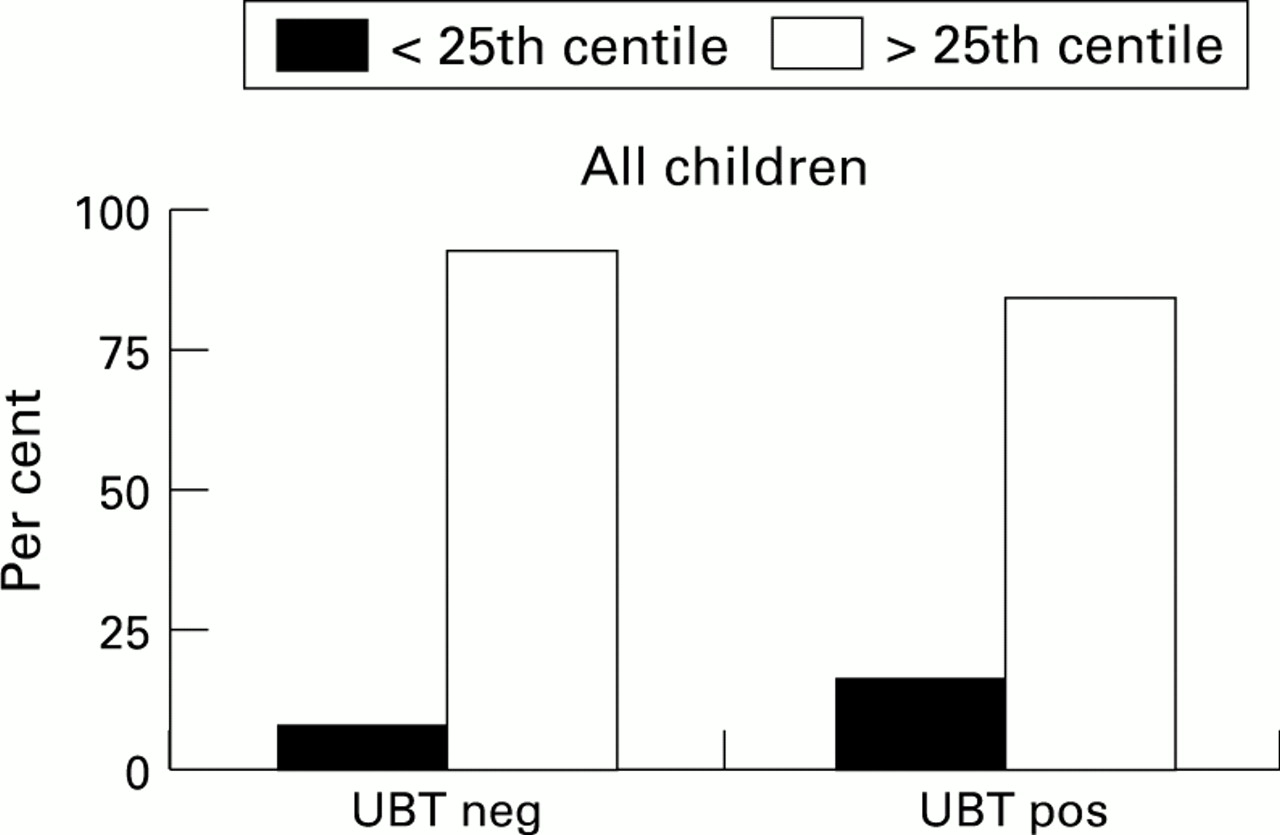
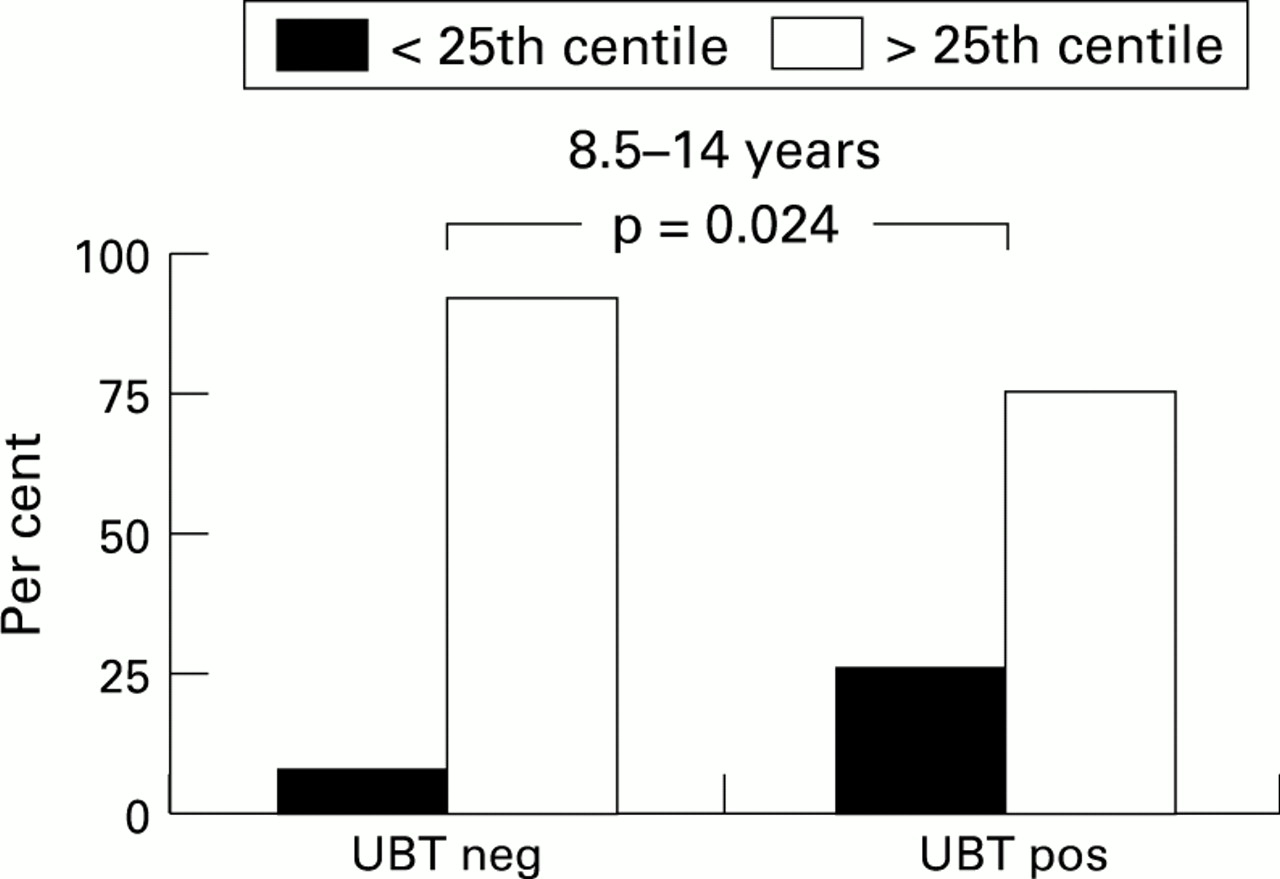
Children were divided according to their centile value for height (fig2). We found that 16.3% (8/49) H pylori positive children were below the 25th centile for height (p = 0.09), compared with 7.8% of H pylori negative children (13/167). Although the trend was not significant, H pylori infected children tended to have a lower centile value for height than non-infected children. This trend became significant when only the older children were considered. Thus in children aged 8.5 to 14 years, 25.8% of H pyloripositive children (8/31) were below the 25th centile for height (p = 0.024) compared with 8.3% of H pylori negative children (8/96) (fig 3). Neither the affected nor the unaffected children who were below the 25th centile for height were found to be positive on antigliadin and antiendomysial antibody testing. Centile values for weight and body surface area were also considered, but we found no difference between infected and non-infected children (data not shown).

H pylori infected and non-infected children divided by height centiles (UBT neg/pos = 13C-urea breath test negative/positive).

{kind=link}
{kind=link}
{kind=link}
H pylori infected and non-infected children aged 8.5 – 14 years divided by height centiles. (UBT neg/pos = 13C-urea breath test negative/positive).
When H pylori status was taken as the dependent variable, stepwise logistic regression analysis showed that the only variables which entered into the model were the socioeconomic class (F = 10.87; p = 0.001) and the centile value for height (F = 2.42; p = 0.12, NS). When the older children were considered independently, the only variables which entered into the model were the centile value for height (F = 6.74; p = 0.011) and socioeconomic class (F = 3.24; p = 0.07, NS).
Discussion
The overall prevalence of H pylori infection in children living in south Italy is about 23%. This figure is higher than the rate reported in children living in north Italy19and in Europe,20-22 but lower than in Africa21 23 or India.24 Our results may reflect the situation in a city with acceptable living conditions, where most people have a job and live in their own houses; however, the social environment is basically rural, the cultural background not generally high, and poor sanitation is still common. As several other studies have shown, poor socioeconomic conditions associated with overcrowding and inadequate hygiene at home are important risk factors for H pylori infection.21 25 Indeed, in our study a significant correlation was found between socioeconomic conditions, household crowding, and H pylori status, confirming the previously reported data. Since environmental factors are important in determining H pylori acquisition, the prevalence rate is expected to increase with age. In our study population, we found no cases of infection in children aged 3 to 4 years, and 33% prevalence in those aged 13 to 14 years.
The effect of H pylori on growth was studied by dividing the children into two different groups according to age. Our hypothesis was that if H pylori infection were able to influence growth, this would be more evident in older children with a long lasting infection than in younger children with a recently acquired infection. Since it is mainly affected by age, height by itself cannot be used to test the hypothesis. By considering the centile value for height, a significant difference in height was found between infected and uninfected children in those older than 8.5 years. In this age group, when the H pylori status was taken as the dependent variable in a logistic regression analysis, only the centile value for height was able to enter into the model. This finding is consistent with the hypothesis that once acquired in early childhood H pylori infection takes several years before it starts to affect growth.
The mechanisms by which H pylori infection might lead to short stature are largely unknown. One possible explanation is that it could cause dyspeptic symptoms, but this does not seem to be the case in the present study since all children were healthy and had not suffered from any relevant illnesses in the past. Alternatively, the infection could result in a low energy intake and malnutrition. This is also unlikely since no effect on growth was observed in the younger subjects and all the children were well nourished. Moreover, no difference in the centile value for weight or in body surface area was detected among infected and non-infected children. A third explanation is based on the assumption that long standing infection induces low grade chronic gastric inflammation and the release of cytokines like interleukin-826 which would in turn affect growth.27 However, there are no data on the circulating levels of these cytokines in infected children, nor is it very likely that these substances influence distant organs. Finally, H pylorimay be associated with a poor socioeconomic background, malnutrition, and exposure to other chronic diseases which could affect growth independently. In our study, socioeconomic status was related with the presence of H pylori infection. However, none of the children with short stature had suffered from relevant chronic infectious diseases in the past nor did any have overt signs of malnutrition. Moreover, logistic regression analysis showed that height was not influenced by socioeconomic status or crowding class. Consequently, even if poor socioeconomic conditions or household overcrowding could determine early acquisition of the infection,H pylori is associated with short stature through mechanisms that are independent of socioeconomic status or crowding class.
Our findings that H pylori infection acquired in childhood is associated with short stature and poor socioeconomic conditions have at least two implications. First, H pylori infection could be one of the environmental causes of growth delay. The decline in incidence of H pylori infection related to general improvements in socioeconomic conditions could be responsible in part for the trend toward increased height growth observed during the last century in developed countries. Second, therapeutic intervention against H pylori infection in children could be recommended not only to prevent ulcer disease or gastric cancer but also to avoid interference with growth. In this respect, we recommend a well designed study in which growth velocity rather than height by itself is evaluated, either before and after H pylorieradication.
We conclude that H pylori infection in Italy is common in childhood, with a prevalence rate approaching 33% by the age of 14. Early acquisition of H pylori infection seems to depend on poor socioeconomic conditions and household overcrowding and is related to short stature. Mechanisms by which H pylori infection might influence growth are unknown, although a direct effect cannot be excluded. Further investigations are needed to discover whether therapeutic intervention in otherwise healthy H pyloriinfected children would avoid restricted or delayed growth.
Acknowledgments
Supported by European Concerted Action BIOMED, BMH1-CT93-1239. We thank B Geypens, V Contangelo, E Squarcella, M G Latiano, A Luypaert, L Swinnen, S Rutten, N Gorris, and D Claus for their skilful technical assistance. Statistical analysis was carried out by G Leandro MD, biostatistician.