Utilization of Mobile Mental Health Services among Syrian Refugees and Other Vulnerable Arab Populations—A Systematic Review

 ,
, 
Abstract
:1. Introduction
1.1. Background
1.2. Study Motivation
Cultural Modulators of Distress and Treatment Acceptance
2. Materials and Methods
2.1. Information Source and Search Strategy
2.2. Inclusion/Exclusion Criteria
2.3. Data Extraction
2.4. Inter-Rater Reliability
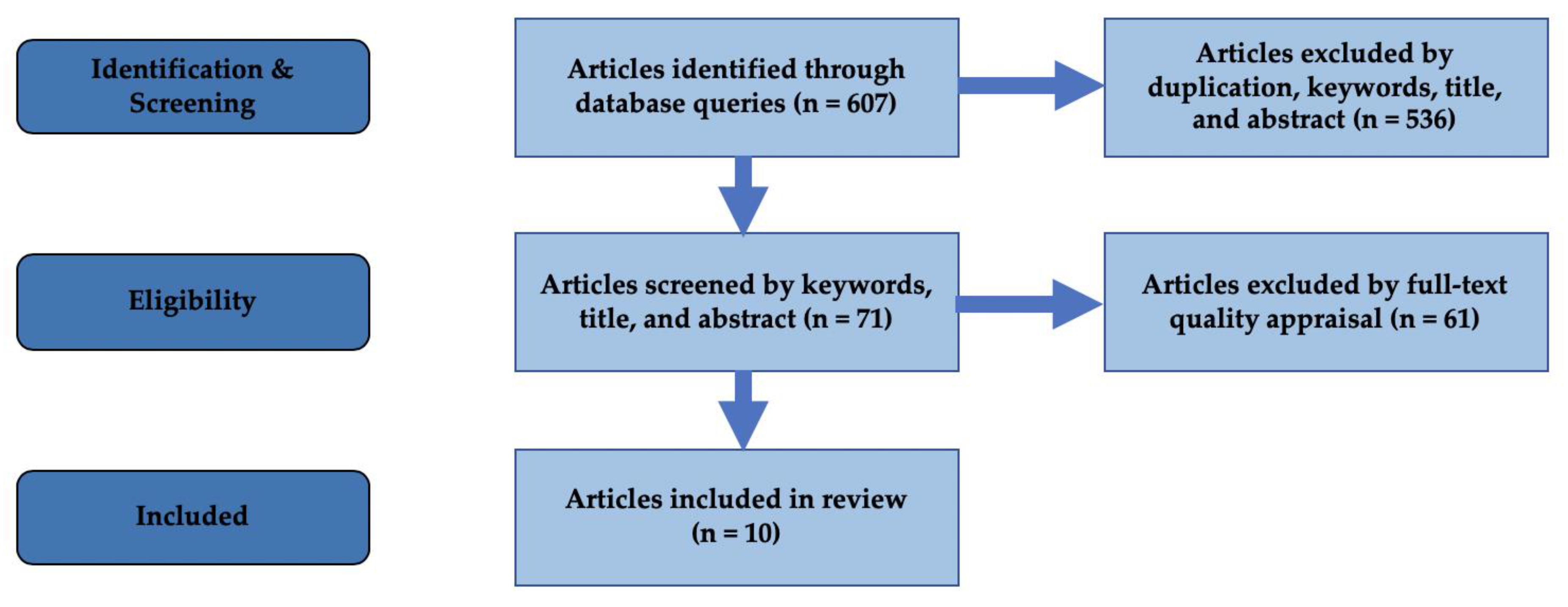
3. Results
3.1. Review Results
3.2. Inter-rater Reliability
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- UNHCR. Refugee Statistics. 2018. Available online: https://www.unrefugees.org/refugee-facts/statistics/ (accessed on 2 April 2019).
- United Nations. Figures at a Glance. Available online: https://www.unhcr.org/figures-at-a-glance.html (accessed on 23 April 2019).
- Connor, P. Where Syrian Refugees Have Resettled Worldwide. 2018. Available online: https://www.pewresearch.org/fact-tank/2018/01/29/where-displaced-syrians-have-resettled/ (accessed on 20 May 2019).
- Refugee Health Technical Assistance Center. Mental Health. 2011. Available online: https://refugeehealthta.org/physical-mental-health/mental-health/ (accessed on 8 April 2019).
- Bogić, M.; Njoku, A.; Priebe, S. Long-term mental health of war-refugees: A systematic literature review. BMC Int. Heal. Hum. Rights 2015, 15, 29. [Google Scholar]
- Ben-Zeev, D.; Fathy, C.; Jonathan, G.; Abuharb, B.; Brian, R.M.; Kesbeh, L.; Abdelkader, S. mHealth for mental health in the Middle East: Need, technology use, and readiness among Palestinians in the West Bank. Asian J. Psychiatry 2017, 27, 1–4. [Google Scholar] [CrossRef] [PubMed]
- WHO GOe. mHealth: New Horizons for Health through Mobile Technologies. 2011. Available online: https://www.who.int/goe/publications/goe_mhealth_web.pdf (accessed on 3 September 2019).
- Global Mobile Phone Subscribers to Reach 4.5 Billion by 2012. Cellular News. Available online: http://www.celllular-news.com/story/29824.php (accessed on 9 March 2008).
- Haenssgen, M.J. The struggle for digital inclusion: Phones, healthcare, and marginalisation in rural India. World Dev. 2018, 104, 358–374. [Google Scholar] [CrossRef] [Green Version]
- Lupton, D. Critical Perspectives on Digital Health Technologies: Digital Health Technologies. Sociol. Compass 2014, 8, 1344–1359. [Google Scholar] [CrossRef]
- Haas, S.; Wohlgemuth, S.; Echizen, I.; Sonehara, N.; Müller, G. Aspects of privacy for electronic health records. Int. J. Med Inform. 2011, 80, e26–e31. [Google Scholar] [CrossRef]
- Sarría-Santamera, A.; Hijas-Gómez, A.I.; Carmona, R.; Feliu, L.A.G. A systematic review of the use of health services by immigrants and native populations. Public Health Rev. 2016, 37, 28. [Google Scholar] [CrossRef] [Green Version]
- Kaya, E.; Caman, O.K.; Kilic, C.; Uner, S. Refugees’ access to and utilization of health services: Challenges and solutions in Turkey. Eur. J. Public Heal. 2018, 28, 214–273. [Google Scholar] [CrossRef]
- Woodward, A.; Fyfe, M.; Handuleh, J.; Patel, P.; Godman, B.; Leather, A.; Finlayson, A.E. Diffusion of e-health innovations in ‘post-conflict’ settings: A qualitative study on the personal experiences of health workers. Hum. Resour. Health 2014, 12, 22. [Google Scholar] [CrossRef] [Green Version]
- Batniji, R.; Khatib, L.; Cammett, M.; Sweet, J.; Basu, S.; Jamal, A.; Wise, P.; Giacaman, R. Governance and health in the Arab world. Lancet 2014, 383, 343–355. [Google Scholar] [CrossRef] [Green Version]
- Saleh, S.; Farah, A.; Dimassi, H.; El Arnaout, N.; Constantin, J.; Osman, M.; El Morr, C.; Alameddine, M.; Ramirez, M.; Menson, W.; et al. Using Mobile Health to Enhance Outcomes of Noncommunicable Diseases Care in Rural Settings and Refugee Camps: Randomized Controlled Trial. JMIR mHealth uHealth 2018, 6, e137. [Google Scholar] [CrossRef]
- Barber, B.K.; McNeely, C.A.; El Sarraj, E.; Daher, M.; Giacaman, R.; Arafat, C.; Barnes, W.; Abu Mallouh, M. Mental Suffering in Protracted Political Conflict: Feeling Broken or Destroyed. PLoS ONE 2016, 11, e0156216. [Google Scholar] [CrossRef] [Green Version]
- Hassan, G.; Kirmayer, L.J.; MekkiBerrada, A.; Quosh, C.; el Chammay, R.; Deville-Stoetzel, J.B.; Youssef, A.; Jefee-Bahloul, H.; Barkeel-Oteo, A.; Coutts, A.; et al. Culture, Context and the Mental Health and Psychosocial Wellbeing of Syrians: A Review for Mental Health and Psychosocial Support staff working with Syrians Affected by Armed Conflict; UNHCR: Geneva, Switzerland, 2015. [Google Scholar]
- International Medical Corps, UNICEF. Mental Health/Psychosocial and Child Protection for Syrian Adolescent Refugees in Jordan; IMC & UNICEF: Amman, Jordan, 2014. [Google Scholar]
- Koga, P.M.; Pirzada, A.F. Ulysses in California: Dignity in Refugee Mental Health; World Mental Health Day, 10 October 2015; World Federation of Mental Health: Occoquan, VA, USA, 2015; pp. 12–13. [Google Scholar]
- Achotegui, J. Extreme stress and mental health: The immigrant syndrome with chronic and multiple stress (Ulysses syndrome). Migr. Mag. 2006, 59–85. [Google Scholar]
- Joseph, S. Gender and Family in the Arab World. In Arab Women. Between Defiance and Restraint; Olive Branch Press: New York, NY, USA, 1996; pp. 194–202. [Google Scholar]
- Chan, S.R.; Torous, J.; Hinton, L.; Yellowlees, P. Mobile Tele-Mental Health: Increasing Applications and a Move to Hybrid Models of Care. Health 2014, 2, 220–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crawford, P.R.; Lehmann, H.P.; Sockolow, P.S. Health Services Research Evaluation Principles. Methods Inf. Med. 2012, 51, 122–130. [Google Scholar] [CrossRef] [PubMed]
- Ossebaard, H.C.; Van Gemert-Pijnen, L. eHealth and quality in health care: Implementation time. Int. J. Qual. Health Care 2016, 28, 415–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajan, J.; Moura, J.; Gourley, G.; Kiso, K.; Sizilio, A.; Cortez, A.M.; Riley, L.; Veras, M.A.D.S.M.; Sarkar, U. Understanding the barriers to successful adoption and use of a mobile health information system in a community health center in São Paulo, Brazil: A cohort study. BMC Med. Inform. Decis. Mak. 2016, 16, 146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzla, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The prisma statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burchert, S.; Alkneme, M.S.; Bird, M.; Carswell, K.; Cuijpers, P.; Hansen, P.; Heim, E.; Shehadeh, M.H.; Sijbrandij, M.; Hof, E.V.; et al. User-Centered App Adaptation of a Low-Intensity E-Mental Health Intervention for Syrian Refugees. Front. Psychol. 2019, 9. [Google Scholar] [CrossRef] [Green Version]
- Atallah, N.; Khalifa, M.; El Metwally, A.; Househ, M. The prevalence and usage of mobile health applications among mental health patients in Saudi Arabia. Comput. Methods Programs Biomed. 2017, 156, 163–168. [Google Scholar] [CrossRef]
- Ramia, J.A.; Shehadeh, M.H.; Kheir, W.; Zoghbi, E.; Watts, S.; Heim, E.; El Chammay, R. Community cognitive interviewing to inform local adaptations of an e-mental health intervention in Lebanon. Glob. Ment. Health 2018, 5. [Google Scholar]
- Morina, N.; Ewers, S.M.; Passardi, S.; Schnyder, U.; Knaevelsrud, C.; Müller, J.; Bryant, R.A.; Nickerson, A.; Schick, M. Mental health assessments in refugees and asylum seekers: Evaluation of a tablet-assisted screening software. Confl. Health 2017, 11, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hashemi, B.; Ali, S.; Awaad, R.; Soudi, L.; Housel, L.; Sosebee, S.J. Facilitating mental health screening of war-torn populations using mobile applications. Soc. Psychiatry Psychiatr. Epidemiol. 2016, 52, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Jefee-Bahloul, H.; Duchen, D.; Barkil-Oteo, A. Attitudes towards Implementation of Store-and-Forward Telemental Health in Humanitarian Settings: Survey of Syrian Healthcare Providers. Telemed. e-Health 2016, 22, 31–35. [Google Scholar] [CrossRef]
- Knaevelsrud, C.; Brand, J.; Lange, A.; Ruwaard, J.; Wagner, B.; Berger, T.; Gläsmer, H.; Morina, N.; Langrial, S. Web-Based Psychotherapy for Posttraumatic Stress Disorder in War-Traumatized Arab Patients: Randomized Controlled Trial. J. Med. Internet Res. 2015, 17, e71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jefee-Bahloul, H.; Moustafa, M.K.; Shebl, F.M.; Barkil-Oteo, A. Pilot Assessment and Survey of Syrian Refugees’ Psychological Stress and Openness to Referral for Telepsychiatry (PASSPORT Study). Telemed. e-Health 2014, 20, 977–979. [Google Scholar] [CrossRef] [PubMed]
- Mucic, D. Transcultural telepsychiatry and its impact on patient satisfaction. J. Telemed. Telecare 2010, 16, 237–242. [Google Scholar] [CrossRef]
- Gearing, R.E.; Schwalbe, C.S.; MacKenzie, M.J.; Brewer, K.B.; Ibrahim, R.W.; Olimat, H.; Al-Makhamreh, S.S.; Mian, I.; Al-Krenawi, A. Adaptation and translation of mental health interventions in Middle Eastern Arab countries: A systematic review of barriers to and strategies for effective treatment implementation. Int. J. Soc. Psychiatry 2012, 59, 671–681. [Google Scholar] [CrossRef]
- Abaza, H.; Marschollek, M. mHealth Application Areas and Technology Combinations. Methods Inf. Med. 2017, 56, e105–e122. [Google Scholar] [CrossRef]


{kind=link}
| Participants |
|
| Interventions |
|
| Comparisons |
|
| Outcomes |
|
| Study Design |
|
| Research Questions |
|
| Journal | Search Query |
|---|---|
| PubMed | (mobile health OR mHealth OR m-Health OR telemedicine OR tele-medicine OR telepsychiatry OR tele-psychiatry) AND (Syria OR Arab OR Arabic OR Saudi Arabia OR Lebanon OR Jordan OR refugee OR “middle east” OR “Middle eastern”) AND (“mental health” OR depression OR PTSD OR psychiatry OR psychiatric) |
| PyscInfo | (mobile health OR mHealth OR m-Health OR telemedicine OR tele-medicine OR telepsychiatry OR tele-psychiatry) AND (Syria OR Arab OR Arabic OR Saudi Arabia OR Lebanon OR Jordan OR refugee OR “middle east” OR “Middle eastern”) AND (“mental health” OR depression OR PTSD OR psychiatry OR psychiatric) |
| ACM | +(“Mobile Health” mHealth telemedicine tele-medicine telepsychiatry tele-psychiatry) +(refugee syria arab arabic “Saudi Arabia’” Lebanon Jordan “Middle East” “middle eastern”) +(“Mental health” depression PTSD psychiatry psychiatric) |
| DOAJ | (mobile health OR mHealth OR m-Health OR telemedicine OR tele-medicine OR telepsychiatry OR tele-psychiatry) AND (Syria OR Arab OR Arabic OR Saudi Arabia OR Lebanon OR Jordan OR refugee OR “middle east” OR “Middle eastern”) AND (“mental health” OR depression OR PTSD OR psychiatry OR psychiatric) |
| Title | Authors | Year Published | Study Type | Objectives | Study Population | Sample Size | Key Findings & Feasibility Results | Barriers Identified |
|---|---|---|---|---|---|---|---|---|
| User-Centered App Adaptation of a Low-Intensity E-Mental Health Intervention for Syrian Refugees [28] | Burchert, Alkneme, Bird, et al. | 2019 | Qualitative study. (Interviews) | To assess mHealth prototype acceptance | Adult Syrian Refugees in Germany, Sweden, and Egypt | 128 | • 78% reacted positively to the potential health impact of the prototype intervention | • Technical literacy • Problems with internet access • Acceptability • Credibility • Technical requirements |
| The prevalence and usage of mobile health applications among mental health patients in Saudi Arabia [29] | Atallah, Khalifa, Metwally, et al. | 2018 | Qualitative study. Cross-Sectional (Surveys) | To explore the prevalence of use of mHealth applications for mental health | Adult, mental health patients in Saudi Arabia | 376 | • 64% use mobile phones to access health data • 64% expressed interest in using mobile phones to track progress of their mental health • 46% reported running 1-2 healthcare applications on their mobile phones | NA |
| Community cognitive interviewing to inform local adaptations of an e-mental health in tervention inLebanon [30] | Abi Ramia, Harper-Shehadeh, Kheir, et al. | 2018 | Qualitative study. (Interviews) | To investigate the use of community-driven adaptation of evidence based e-mental interventions outlined by WHO (Step-by-Step) | Lebanese, Palestinian, and Syrian Health workers and community members in Lebanon | 66 | • Significant adaptation of WHO’s Step-by-Step online intervention to the Lebanese community • 30% decrease in length • Additional videos with alternate delivery methods • Greater focus on enjoyable activities • Support styles were adapted to gender norms • Several other minor changes | • Gender differences in preferred intervention styles • Length of intervention • Privacy and security of data • General distrust of healthcare providers • Lack of mental health awareness |
| mHealth for mental health in the Middle East: Need, technology use, and readiness among Palestinians in the West Bank [6] | Ben-Zeev, Fathy, Jonathan, et al. | 2017 | Qualitative study. Cross-Sectional (Surveys) | To assess mobile phone use and interest in mHealth for mental health | Adult Palestinians in the West Bank | 272 | • 93.4% own a mobile phone • 99.6% use social media regularly • 88.2% thought mobile health interventions would be helpful to people with mental health problems • 66% report interest in mHealth for mental health | NA |
| Mental health assessments in refugees and asylum seekers: evaluation of a tablet-assisted screening software [31] | Morina, Ewers, Passardi, et al. | 2017 | Randomized Crossover Trial | To investigate the efficacy and feasibility of psychological screening software for touch-screen devices | Adult refugees and Asylum seeksers in Zurich, Switzerland originating from Afghanistan, Iraq, Turkey, Sri Lanka, and Sudan. | 30 | • No significant difference between conventional and mobile application screening, suggesting feasibility and efficacy • Improved time efficiency using mobile application | NA |
| Facilitating mental health screening of war-torn populations using mobile applications [32] | Hashemi, Ali, Awaad, et al. | 2016 | Qualitative study. Cross-sectional (Surveys and Interviews) | To investigate the efficacy and utility of a mobile application for mental health screening | Palestinian children in Gaza | 986 | • Screened children were found to suffer from a wide range of hyperarousal, re-experiencing, depressive, and somatic symptoms • The open data kit (ODK) open source mobile application proved to be an easy, efficient, and feasible data collection tool in a resource constrained setting | NA |
| Attitudes Towards Implementation of Store-and-Forward Telemental Health in Humanitarian Settings: Survey of Syrian Healthcare Providers [33] | Jefee-Bahloul, Duchen, Barkil-Oteo | 2016 | Cross-Sectional (Surveys) | To investigate perception and feasibility of use of audio/video recordings for telepsyciatry | Adult Syrian healthcare providers in NGOs working in the Syrian disaster setting | 30 | • Half of the providers believed that mental healthcare can be provided through audio/video data consultation, and that there would be benefit from such services • Providers generally believed that Syrian patients would agree to be recorded for psychiatric service | • Perceived barriers included cultural, financial, and technical barriers |
| Web-Based Psychotherapy for Posttraumatic Stress Disorder in War-Traumatized Arab Patients: Randomized Controlled Trial [34] | Knaevelsrud, Brand, Lange, et al. | 2015 | Randomized Control Trial | To investigate the efficacy of cognitive behavioral internet-based intervention | Adult, War-traumatized Arab patients in Iraq. All participants have PTSD | 159 (79 in treatment group) | • 62% of treatment group had recovered from PTSD symptoms at 3-month follow-up versus 1 patient in the control group (p < 0.001; OR 74.19) | NA |
| Pilot Assessment and Survey of Syrian Refugees’ Psychological Stress and Openness to Referral for Telepsychiatry (PASSPORT Study) [35] | Jefee-Bahloul, Moustafa, Shebl, et al. | 2014 | Cross-Sectional (Surveys) | To investigate psychological burden and openness to telepsychiatry | Adult Syrian Refugees in Kilis, Turkey | 354 | • 41.8% showed scores indicative of PTSD • 45% willing to use telepsychiatry • 34% reported perceived need to see psychiatrist | The following were negatively associated with willingness to receive telepsychiatry: • Female gender • Bilingual • Positive score testing for PTSD |
| Transcultural telepsychiatry and its impact on patient satisfaction [36] | Mucic | 2009 | Cross-Sectional (Surveys) | To investigate patient satisfaction regarding the use of videoconferencing for telepsyciatric care | Adult asylum seekers, refugees, and migrants in Denmark | 52 | • Patients reported a high level of satisfaction and willingness to use telepsychiatry again and recommend it to others. They preferred telepsychiatry in their mother tongue rather than interpreter-assisted care. | • Limited infrastructure regarding setup of telepsychiatry areas and exam rooms |
| Phases of Articles Selection | k |
|---|---|
| Initial screening | |
| 1. Author dependence on Title for inclusion/exclusion | 0.95 |
| 2. Author dependence on Abstract for inclusion/exclusion | 0.87 |
| 3. Author dependence on the Full Article for inclusion/exclusion | 0.83 |
| 4. Inclusion of non-Review articles (outcomes based studies, qualitative studies and randomized control trials) | 0.92 |
| 5. Inclusion of Review Articles | 0.93 |
| 6. Comprehensiveness of Search | 0.92 |
| Quality Evaluation | |
| 7. Quality of Topic | 0.84 |
| 8. Quality of Study Design | 0.95 |
| 9. Scientific Quality of Research | 0.89 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ashfaq, A.; Esmaili, S.; Najjar, M.; Batool, F.; Mukatash, T.; Al-Ani, H.A.; Koga, P.M. Utilization of Mobile Mental Health Services among Syrian Refugees and Other Vulnerable Arab Populations—A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 1295. https://doi.org/10.3390/ijerph17041295
Ashfaq A, Esmaili S, Najjar M, Batool F, Mukatash T, Al-Ani HA, Koga PM. Utilization of Mobile Mental Health Services among Syrian Refugees and Other Vulnerable Arab Populations—A Systematic Review. International Journal of Environmental Research and Public Health. 2020; 17(4):1295. https://doi.org/10.3390/ijerph17041295
Chicago/Turabian StyleAshfaq, Adeel, Shawn Esmaili, Mona Najjar, Farva Batool, Tariq Mukatash, Hadeer Akram Al-Ani, and Patrick Marius Koga. 2020. "Utilization of Mobile Mental Health Services among Syrian Refugees and Other Vulnerable Arab Populations—A Systematic Review" International Journal of Environmental Research and Public Health 17, no. 4: 1295. https://doi.org/10.3390/ijerph17041295