Outcomes of Patients with Early Onset Colorectal Cancer Treated in a UK Specialist Cancer Center

 , , ,
, , ,
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
2.2. Treatment and Outcomes in Patients with Stage II and III EOCRC
2.2.1. Neo-Adjuvant Chemoradiation
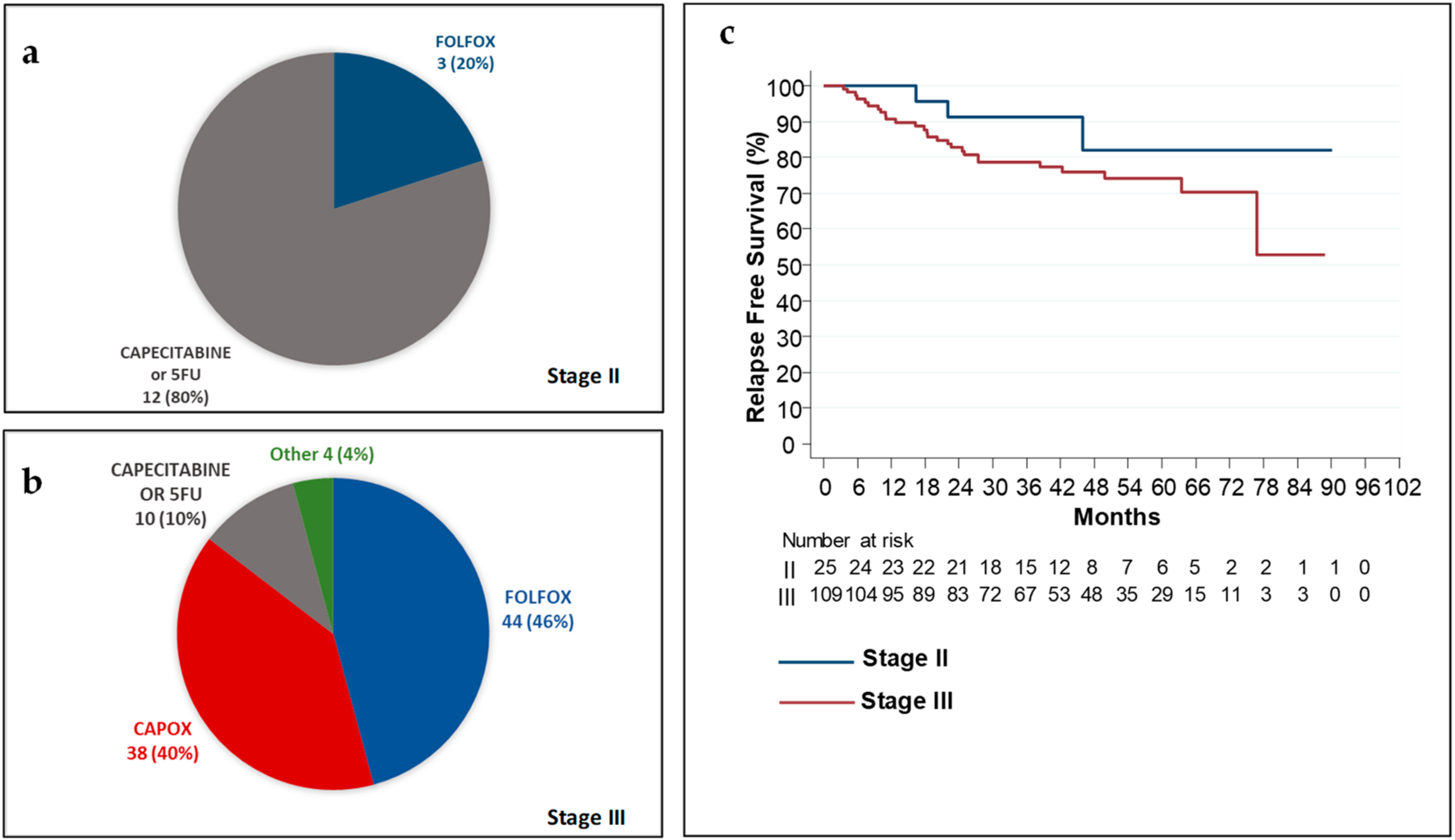
2.2.2. Curative Surgery and Adjuvant Chemotherapy
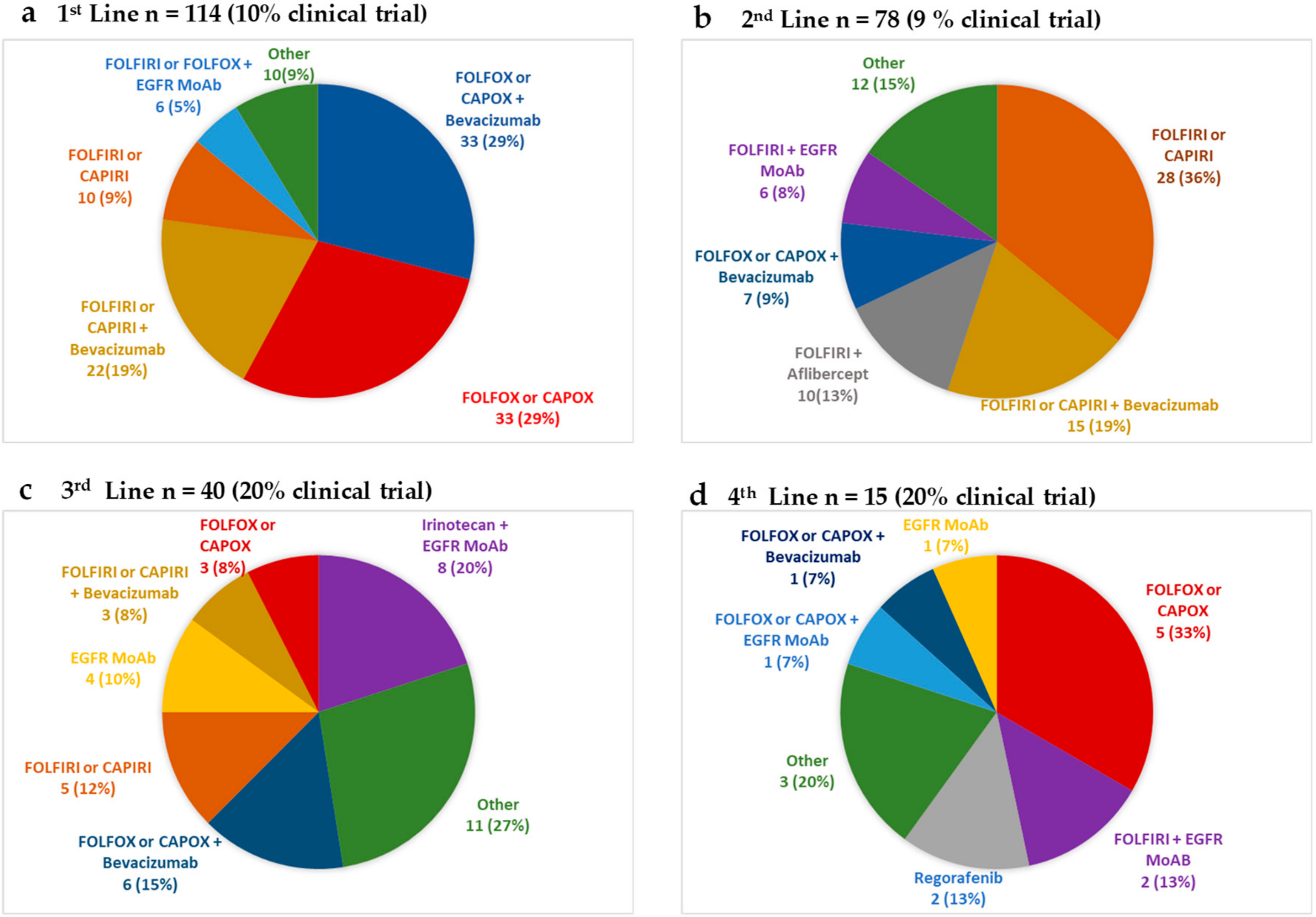
2.3. Treatment and Outcomes in Patients with Stage IV EOCRC
2.4. Prognostic Markers of Survival in Patients with Stage IV CRC
- age 20–29 (n = 13), mOS 15.9 (95% C.I 7.0–43.0)
- age 30–39 (n = 37), mOS 17.1 (95% C.I not reached)
- age 40–49 (n = 72), mOS 21.7 (95% C.I 16.2–27.7)
3. Discussion
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, 359–386. [Google Scholar] [CrossRef] [PubMed]
- Pignone, M.; Rich, M.; Teutsch, S.M.; Berg, A.O.; Lohr, K.N. Screening for colorectal cancer in adults at average risk: A summary of the evidence for the U.S. Preventive Services Task Force. Ann. Intern. Med. 2002, 137, 132–141. [Google Scholar] [CrossRef] [PubMed]
- Vuik, F.E.; Nieuwenburg, S.A.; Bardou, M.; Lansdorp-Vogelaar, I.; Dinis-Ribeiro, M.; Bento, M.J.; Zadnik, V.; Pellise, M.; Esteban, L.; Kaminski, M.F.; et al. Increasing incidence of colorectal cancer in young adults in Europe over the last 25 years. Gut 2019. [Google Scholar] [CrossRef] [PubMed]
- Troeung, L.; Sodhi-Berry, N.; Martini, A.; Malacova, E.; Ee, H.; O’Leary, P.; Lansdorp-Vogelaar, I.; Preen, D.B. Increasing Incidence of Colorectal Cancer in Adolescents and Young Adults Aged 15–39 Years in Western Australia 1982–2007: Examination of Colonoscopy History. Front. Public Health 2017, 5, 179. [Google Scholar] [CrossRef] [PubMed]
- Lui, R.N.; Tsoi, K.K.; Ho, J.M.; Lo, C.M.; Chan, F.C.; Kyaw, M.H.; Sung, J.J. Global Increasing Incidence of Young-Onset Colorectal Cancer Across 5 Continents: A Joinpoint Regression Analysis of 1,922,167 Cases. Cancer Epidemiol. Biomark. Prev. 2019. [Google Scholar] [CrossRef] [PubMed]
- Barreto, S.G.; Chaubal, G.N.; Talole, S.; DeSouza, A.; Suradkar, K.; Gaikwad, V.; Goel, M.; Shrikhande, S.V. Rectal cancer in young Indians—Are these cancers different compared to their older counterparts? Indian J. Gastroenterol. 2014, 33, 146–150. [Google Scholar] [CrossRef]
- Siegel, R.L.; Fedewa, S.A.; Anderson, W.F.; Miller, K.D.; Ma, J.; Rosenberg, P.S.; Jemal, A. Colorectal Cancer Incidence Patterns in the United States, 1974–2013. J. Natl. Cancer Inst. 2017, 109. [Google Scholar] [CrossRef]
- Ahnen, D.J.; Wade, S.W.; Jones, W.F.; Sifri, R.; Mendoza Silveiras, J.; Greenamyer, J.; Guiffre, S.; Axilbund, J.; Spiegel, A.; You, Y.N. The increasing incidence of young-onset colorectal cancer: A call to action. Mayo Clin. Proc. 2014, 89, 216–224. [Google Scholar] [CrossRef]
- Silla, I.O.; Rueda, D.; Rodriguez, Y.; Garcia, J.L.; De la Cruz Vigo, F.; Perea, J. Early-onset colorectal cancer: A separate subset of colorectal cancer. World J. Gastroenterol. 2014, 20, 17288–17296. [Google Scholar] [CrossRef]
- Perea, J.; Rueda, D.; Canal, A.; Rodriguez, Y.; Alvaro, E.; Osorio, I.; Alegre, C.; Rivera, B.; Martinez, J.; Benitez, J.; et al. Age at onset should be a major criterion for subclassification of colorectal cancer. J. Mol. Diagn. 2014, 16, 116–126. [Google Scholar] [CrossRef]
- Connell, L.C.; Mota, J.M.; Braghiroli, M.I.; Hoff, P.M. The Rising Incidence of Younger Patients With Colorectal Cancer: Questions About Screening, Biology, and Treatment. Curr. Treat. Options Oncol. 2017, 18, 23. [Google Scholar] [CrossRef] [PubMed]
- Mork, M.E.; You, Y.N.; Ying, J.; Bannon, S.A.; Lynch, P.M.; Rodriguez-Bigas, M.A.; Vilar, E. High Prevalence of Hereditary Cancer Syndromes in Adolescents and Young Adults With Colorectal Cancer. J. Clin. Oncol. 2015, 33, 3544–3549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stigliano, V.; Sanchez-Mete, L.; Martayan, A.; Anti, M. Early-onset colorectal cancer: A sporadic or inherited disease? World J. Gastroenterol. 2014, 20, 12420–12430. [Google Scholar] [CrossRef] [PubMed]
- Lynch, H.T.; De la Chapelle, A. Hereditary colorectal cancer. N. Engl. J. Med. 2003, 348, 919–932. [Google Scholar] [CrossRef]
- Yiu, R.; Qiu, H.; Lee, S.H.; Garcia-Aguilar, J. Mechanisms of microsatellite instability in colorectal cancer patients in different age groups. Dis. Colon Rectum 2005, 48, 2061–2069. [Google Scholar] [CrossRef]
- Bailey, C.E.; Hu, C.Y.; You, Y.N.; Bednarski, B.K.; Rodriguez-Bigas, M.A.; Skibber, J.M.; Cantor, S.B.; Chang, G.J. Increasing disparities in the age-related incidences of colon and rectal cancers in the United States, 1975–2010. JAMA Surg. 2015, 150, 17–22. [Google Scholar] [CrossRef]
- Siegel, R.L.; Medhanie, G.A.; Fedewa, S.A.; Jemal, A. State variation in early-onset colorectal cancer in the United States, 1995–2015. J. Natl. Cancer Inst. 2019. [Google Scholar] [CrossRef]
- Carroll, R.; Zhao, S. Trends in Colorectal Cancer Incidence and Survival in Iowa SEER Data: The Timing of It All. Clin. Colorectal Cancer 2018. [Google Scholar] [CrossRef]
- Dwyer, A.J.; Murphy, C.C.; Boland, C.R.; Garcia, R.; Hampel, H.; Limburg, P.; Lowery, J.; Zauber, A.G.; Waring, S.; Worrall, S.; et al. A summary of the Fight Colorectal Cancer working meeting: Exploring risk factors and etiology of sporadic early-age onset colorectal cancer. Gastroenterology 2019. [Google Scholar] [CrossRef]
- Meyer, J.E.; Narang, T.; Schnoll-Sussman, F.H.; Pochapin, M.B.; Christos, P.J.; Sherr, D.L. Increasing incidence of rectal cancer in patients aged younger than 40 years: An analysis of the surveillance, epidemiology, and end results database. Cancer 2010, 116, 4354–4359. [Google Scholar] [CrossRef]
- Kneuertz, P.J.; Chang, G.J.; Hu, C.Y.; Rodriguez-Bigas, M.A.; Eng, C.; Vilar, E.; Skibber, J.M.; Feig, B.W.; Cormier, J.N.; You, Y.N. Overtreatment of young adults with colon cancer: More intense treatments with unmatched survival gains. JAMA Surg. 2015, 150, 402–409. [Google Scholar] [CrossRef] [PubMed]
- Alvaro, E.; Cano, J.M.; Garcia, J.L.; Brandariz, L.; Olmedillas-Lopez, S.; Arriba, M.; Rueda, D.; Rodriguez, Y.; Canete, A.; Arribas, J.; et al. Clinical and Molecular Comparative Study of Colorectal Cancer Based on Age-of-onset and Tumor Location: Two Main Criteria for Subclassifying Colorectal Cancer. Int. J. Mol. Sci. 2019, 20, 968. [Google Scholar] [CrossRef] [PubMed]
- Russo, A.G.; Andreano, A.; Sartore-Bianchi, A.; Mauri, G.; Decarli, A.; Siena, S. Increased incidence of colon cancer among individuals younger than 50 years: A 17 years analysis from the cancer registry of the municipality of Milan, Italy. Cancer Epidemiol. 2019, 60, 134–140. [Google Scholar] [CrossRef] [PubMed]
- Segev, L.; Kalady, M.F.; Church, J.M. Left-Sided Dominance of Early-Onset Colorectal Cancers: A Rationale for Screening Flexible Sigmoidoscopy in the Young. Dis. Colon Rectum 2018, 61, 897–902. [Google Scholar] [CrossRef] [PubMed]
- Ben-Ishay, O.; Brauner, E.; Peled, Z.; Othman, A.; Person, B.; Kluger, Y. Diagnosis of colon cancer differs in younger versus older patients despite similar complaints. Isr. Med. Assoc. J. 2013, 15, 284–287. [Google Scholar]
- Olivo, R.; Ratnayake, S. Colorectal cancer in young patients: A retrospective cohort study in a single institution. ANZ J. Surg. 2019. [Google Scholar] [CrossRef]
- Gibson, F.; Pearce, S.; Fern, L.; Martins, A.; Kelly, D. Improving the identification of cancer in young people: A scoping review. Expert Rev. Qual. Life Cancer Care 2017, 2, 87–101. [Google Scholar] [CrossRef] [Green Version]
- Kasi, P.M.; Shahjehan, F.; Cochuyt, J.J.; Li, Z.; Colibaseanu, D.T.; Merchea, A. Rising Proportion of Young Individuals With Rectal and Colon Cancer. Clin. Colorectal Cancer 2018. [Google Scholar] [CrossRef]
- Wolf, A.M.D.; Fontham, E.T.H.; Church, T.R.; Flowers, C.R.; Guerra, C.E.; LaMonte, S.J.; Etzioni, R.; McKenna, M.T.; Oeffinger, K.C.; Shih, Y.T.; et al. Colorectal cancer screening for average-risk adults: 2018 guideline update from the American Cancer Society. CA A Cancer J. Clin. 2018, 68, 250–281. [Google Scholar] [CrossRef]
- Cunningham, D.; Atkin, W.; Lenz, H.J.; Lynch, H.T.; Minsky, B.; Nordlinger, B.; Starling, N. Colorectal cancer. Lancet (London, England) 2010, 375, 1030–1047. [Google Scholar] [CrossRef]
- Khan, S.A.; Morris, M.; Idrees, K.; Gimbel, M.I.; Rosenberg, S.; Zeng, Z.; Li, F.; Gan, G.; Shia, J.; LaQuaglia, M.P.; et al. Colorectal cancer in the very young: A comparative study of tumor markers, pathology and survival in early onset and adult onset patients. J. Pediatr. Surg. 2016, 51, 1812–1817. [Google Scholar] [CrossRef] [PubMed]
- Le, D.T.; Durham, J.N.; Smith, K.N.; Wang, H.; Bartlett, B.R.; Aulakh, L.K.; Lu, S.; Kemberling, H.; Wilt, C.; Luber, B.S.; et al. Mismatch repair deficiency predicts response of solid tumors to PD-1 blockade. Science (New York, NY) 2017, 357, 409–413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gray, R.; Barnwell, J.; McConkey, C.; Hills, R.K.; Williams, N.S.; Kerr, D.J. Adjuvant chemotherapy versus observation in patients with colorectal cancer: A randomised study. Lancet (London, England) 2007, 370, 2020–2029. [Google Scholar] [CrossRef]
- Iveson, T.J.; Kerr, R.S.; Saunders, M.P.; Cassidy, J.; Hollander, N.H.; Tabernero, J.; Haydon, A.; Glimelius, B.; Harkin, A.; Allan, K.; et al. 3 versus 6 months of adjuvant oxaliplatin-fluoropyrimidine combination therapy for colorectal cancer (SCOT): An international, randomised, phase 3, non-inferiority trial. Lancet Oncol. 2018, 19, 562–578. [Google Scholar] [CrossRef]
- Mauri, G.; Sartore-Bianchi, A.; Russo, A.G.; Marsoni, S.; Bardelli, A.; Siena, S. Early-onset colorectal cancer in young individuals. Mol. Oncol. 2019, 13, 109–131. [Google Scholar] [CrossRef]
- Khakoo, S.; Georgiou, A.; Gerlinger, M.; Cunningham, D.; Starling, N. Circulating tumour DNA, a promising biomarker for the management of colorectal cancer. Crit. Rev. Oncol. Hematol. 2018, 122, 72–82. [Google Scholar] [CrossRef]
- Van Cutsem, E.; Rivera, F.; Berry, S.; Kretzschmar, A.; Michael, M.; DiBartolomeo, M.; Mazier, M.A.; Canon, J.L.; Georgoulias, V.; Peeters, M.; et al. Safety and efficacy of first-line bevacizumab with FOLFOX, XELOX, FOLFIRI and fluoropyrimidines in metastatic colorectal cancer: The BEAT study. Ann. Oncol. 2009, 20, 1842–1847. [Google Scholar] [CrossRef]
- Kozloff, M.; Yood, M.U.; Berlin, J.; Flynn, P.J.; Kabbinavar, F.F.; Purdie, D.M.; Ashby, M.A.; Dong, W.; Sugrue, M.M.; Grothey, A. Clinical outcomes associated with bevacizumab-containing treatment of metastatic colorectal cancer: The BRiTE observational cohort study. Oncologist 2009, 14, 862–870. [Google Scholar] [CrossRef]
- Khakoo, S.; Chau, I.; Pedley, I.; Ellis, R.; Steward, W.; Harrison, M.; Baijal, S.; Tahir, S.; Ross, P.; Raouf, S.; et al. ACORN: Observational Study of Bevacizumab in Combination With First-Line Chemotherapy for Treatment of Metastatic Colorectal Cancer in the UK. Clin. Colorectal Cancer 2019. [Google Scholar] [CrossRef]
- Cremolini, C.; Loupakis, F.; Antoniotti, C.; Lupi, C.; Sensi, E.; Lonardi, S.; Mezi, S.; Tomasello, G.; Ronzoni, M.; Zaniboni, A.; et al. FOLFOXIRI plus bevacizumab versus FOLFIRI plus bevacizumab as first-line treatment of patients with metastatic colorectal cancer: Updated overall survival and molecular subgroup analyses of the open-label, phase 3 TRIBE study. Lancet Oncol. 2015, 16, 1306–1315. [Google Scholar] [CrossRef]
- Loupakis, F.; Cremolini, C.; Salvatore, L.; Masi, G.; Sensi, E.; Schirripa, M.; Michelucci, A.; Pfanner, E.; Brunetti, I.; Lupi, C.; et al. FOLFOXIRI plus bevacizumab as first-line treatment in BRAF mutant metastatic colorectal cancer. Eur. J. Cancer 2014, 50, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Cremolini, C.; Antoniotti, C.; Lonardi, S.; Bergamo, F.; Cortesi, E.; Tomasello, G.; Moretto, R.; Ronzoni, M.; Racca, P.; Loupakis, F.; et al. Primary tumor sidedness and benefit from FOLFOXIRI plus bevacizumab as initial therapy for metastatic colorectal cancer. Retrospective analysis of the TRIBE trial by GONO. Ann. Oncol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Blanke, C.D.; Bot, B.M.; Thomas, D.M.; Bleyer, A.; Kohne, C.H.; Seymour, M.T.; de Gramont, A.; Goldberg, R.M.; Sargent, D.J. Impact of young age on treatment efficacy and safety in advanced colorectal cancer: A pooled analysis of patients from nine first-line phase III chemotherapy trials. J. Clin. Oncol. 2011, 29, 2781–2786. [Google Scholar] [CrossRef] [PubMed]
- Lieu, C.H.; Renfro, L.A.; De Gramont, A.; Meyers, J.P.; Maughan, T.S.; Seymour, M.T.; Saltz, L.; Goldberg, R.M.; Sargent, D.J.; Eckhardt, S.G.; et al. Association of age with survival in patients with metastatic colorectal cancer: Analysis from the ARCAD Clinical Trials Program. J. Clin. Oncol 2014, 32, 2975–2984. [Google Scholar] [CrossRef] [PubMed]
- Cavestro, G.M.; Mannucci, A.; Zuppardo, R.A.; Di Leo, M.; Stoffel, E.; Tonon, G. Early onset sporadic colorectal cancer: Worrisome trends and oncogenic features. Dig. Liver Dis. 2018, 50, 521–532. [Google Scholar] [CrossRef]
- Willauer, A.N.; Liu, Y.; Pereira, A.A.L.; Lam, M.; Morris, J.S.; Raghav, K.P.S.; Morris, V.K.; Menter, D.; Broaddus, R.; Meric-Bernstam, F.; et al. Clinical and molecular characterization of early-onset colorectal cancer. Cancer 2019, 125, 2002–2010. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Stage II n (%) | Stage III n (%) | Stage IV n (%) | All Patients n (%) |
|---|---|---|---|---|
| Stage at diagnosis * | 27 (11) | 120 (50) | 93 (39) | 241 (100) |
| Sex | ||||
| Female | 13 (48) | 47 (39) | 46 (49) | 107 (44) |
| Male | 14 (52) | 73 (61) | 47 (51) | 134 (56) |
| Age | ||||
| Mean | 40 | 40 | 41 | 40 |
| Median | 40 | 43 | 43 | 42 |
| Range (min–max) | 25–49 | 25–49 | 21–49 | 19–49 |
| <20 | 0 (0) | 1 (<1) | 0 (0) | 1 (<1) |
| 20–29 | 2 (7) | 12 (10) | 10 (11) | 24 (10) |
| 30–39 | 11 (41) | 39 (33) | 28 (30) | 78 (32) |
| 40–49 | 14 (52) | 68 (57) | 55 (59) | 138 (57) |
| Ethnic Background | ||||
| White British | 14 (52) | 77 (64) | 64 (69) | 156 (65) |
| White Irish | 0 (0) | 3 (2) | 1 (1) | 4 (2) |
| White Other | 2 (7) | 8 (7) | 8 (9) | 18 (7) |
| Asian/Asian-British | 2 (7) | 14 (12) | 8 (9) | 24 (10) |
| African/Caribbean/Black British | 4 (15) | 10 (8) | 4 (4) | 18 (7) |
| Mixed/Multiple (Other Mixed) | 1 (4) | 0 (0) | 0 (0) | 1 (<1) |
| Another Ethnic Group | 4 (15) | 8 (7) | 8 (9) | 20 (8) |
| ECOG PS | ||||
| 0 | 12 (44) | 24 (20) | 16 (17) | 52 (22) |
| 1 | 15 (56) | 95 (79) | 68 (73) | 179 (74) |
| 2 | 0 (0) | 1 (1) | 4 (4) | 5 (2) |
| 3 | 0 (0) | 0 (0) | 5 (5) | 5 (2) |
| Location of primary tumor | ||||
| Caecum/ascending colon | 5 (18) | 31 (26) | 21 (23) | 57 (24) |
| Transverse colon | 3 (11) | 10 (8) | 5 (5) | 18 (7) |
| Descending colon/sigmoid | 7 (26) | 26 (22) | 31 (33) | 64 (26) |
| Recto-sigmoid | 1 (4) | 4 (3) | 11 (12) | 16 (7) |
| Rectum | 11 (41) | 49 (41) | 25 (27) | 86 (36) |
| Histology | ||||
| Adenocarcinoma | 23 (85) | 103 (86) | 83 (89) | 210 (87) |
| Mucinous adenocarcinoma | 4 (15) | 16 (13) | 3 (3) | 23 (10) |
| Signet cell | 0 (0) | 1 (1) | 5 (5) | 6 (2) |
| Unknown | 0 (0) | 0 (0) | 2 (2) | 2 (1) |
| Primary Tumor differentiation | ||||
| Well | 1 (4) | 3 (2) | 0 (0) | 4 (2) |
| Moderate | 23 (85) | 93 (78) | 60 (65) | 176 (73) |
| Poor | 3 (11) | 21 (18) | 20 (21) | 45 (19) |
| Unknown | 0 (0) | 3 (2) | 13 (14) | 16 (6) |
| KRAS | ||||
| Mutant | 8 (30) | 18 (15) | 23 (25) | 49 (20) |
| Wild type | 4 (15) | 35 (29) | 46 (50) | 85 (35) |
| Unknown | 15 (55) | 67 (56) | 24 (26) | 107 (44) |
| NRAS | ||||
| Mutant | 0 | 0 | 0 | 0 |
| Wild type | 6 (22) | 31 (26) | 28 (30) | 65 (27) |
| Unknown | 21 (78) | 89 (74) | 65 (70) | 176 (73) |
| BRAF | ||||
| Mutant | 0 (0) | 8 (7) | 4 (4) | 12 (5) |
| Wild type | 6 (22) | 24 (20) | 24 (26) | 54 (22) |
| Unknown | 21 (78) | 88 (73) | 65 (70) | 175 (73) |
| MMR | ||||
| Deficient | 3 (11) | 13 (11) | 1 (1) | 17 (7) |
| Proficient | 22 (82) | 69 (57) | 56 (60) | 148 (61) |
| Unknown | 2 (7) | 38 (32) | 36 (39) | 76 (32) |
| Hereditary Syndromes | ||||
| Lynch syndrome | 3 (11) | 7 (6) | 1 (1) | 11 (5) |
| FAP | 1 (4) | 0 (0) | 0 (0) | 1 (<1) |
| Other | 0 (0) | 3 (3) | 1 (1) | 4 (2) |
| Line of Metastatic SACT | 1st | 2nd | 3rd | 4th | 5th |
|---|---|---|---|---|---|
| Number of Patients | 114 | 78 | 40 | 15 | 6 |
| Best response for each line of SACT n (%) | CR 4 (3) | CR 1 (1) | CR 0 (0) | CR 0 (0) | CR 0 (0) |
| PR 46 (40) | PR 13 (17) | PR 3 (8) | PR 1 (7) | PR 0 (0) | |
| SD 26 (23) | SD 20 (26) | SD 9 (23) | SD 2 (13) | SD 2 (33) | |
| PD 36 (32) | PD 40 (51) | PD 28 (70) | PD 11 (73) | PD 4 (67) | |
| NA 2 (2) | NA 4 (5) | NA 0 (0) | NA 1 (7) | NA 0 (0) | |
| Regimen modification n (%) | 43 (38) | 17 (22) | 4 (10) | 3(20) | 0 |
| Median PFS for each line of SAC.T (95% CI), months | 6.9 | 5.0 | 2.0 | 3.9 | 2.7 |
| (5.8–9.4) | (3.4–6.1) | (1.7–3.8) | (1.7–5.4) | (1.5–NA) | |
| Median OS (95% C.I) for patients whose total lines of SACT in metastatic setting was: (months) | 9.0 | 14.9 | 18.7 | 31.7 | 32.0 |
| (4.1–27.7) | (9.6–19.0) | (14.3–28.6) | (20.246.5) | (N/A) |
| Prognostic Variable | Number of Patients | mOS (95% C.I) Months | p-Value |
|---|---|---|---|
| Histopathology | |||
| Adenocarcinoma | 107 | 20.2 (16.1–26.7) | p < 0.001 |
| Mucinous Adenocarcinoma | 7 | 15.8 (NA) | |
| Signet cells | 5 | 7.0 (NA) | |
| Location of Primary | |||
| Left | 90 | 22.5 (16.2–27.7) | p = 0.18 |
| Right | 33 | 15.9 (9.0–22.0) | |
| KRAS Status * | |||
| Mutant | 32 | 18.5 (11.7–26.2) | p = 0.38 |
| Wild Type | 56 | 22.6 (17.1–28.8) | |
| BRAF Status ** | |||
| Mutant | 7 | 17.1 (NA) | p = 0.45 |
| Wild Type | 34 | 23.2 (16.0–46.5) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Georgiou, A.; Khakoo, S.; Edwards, P.; Minchom, A.; Kouvelakis, K.; Kalaitzaki, E.; Nobar, N.; Calamai, V.; Ifijen, M.; Husson, O.; et al. Outcomes of Patients with Early Onset Colorectal Cancer Treated in a UK Specialist Cancer Center. Cancers 2019, 11, 1558. https://doi.org/10.3390/cancers11101558
Georgiou A, Khakoo S, Edwards P, Minchom A, Kouvelakis K, Kalaitzaki E, Nobar N, Calamai V, Ifijen M, Husson O, et al. Outcomes of Patients with Early Onset Colorectal Cancer Treated in a UK Specialist Cancer Center. Cancers. 2019; 11(10):1558. https://doi.org/10.3390/cancers11101558
Chicago/Turabian StyleGeorgiou, Alexandros, Shelize Khakoo, Penelope Edwards, Anna Minchom, Kyriakos Kouvelakis, Eleftheria Kalaitzaki, Natalie Nobar, Vanessa Calamai, Maria Ifijen, Olga Husson, and et al. 2019. "Outcomes of Patients with Early Onset Colorectal Cancer Treated in a UK Specialist Cancer Center" Cancers 11, no. 10: 1558. https://doi.org/10.3390/cancers11101558