Article Text

Abstract
Background The COVID-19 crisis forced hospitals in the UK dramatically to reduce outpatient activity. To provide continuity of care and to assist patients reluctant or unable to leave their homes, video consultations were rapidly implemented across routine and emergency ophthalmology services.
Objective To describe the deployment and scaling to a large volume of teleophthalmology using a video consultation platform ‘Attend Anywhere’ in Moorfields Eye Hospital’s accident and emergency (A&E) department (London, UK).
Method Patient satisfaction, waiting time, consultation duration, outcome and management were audited following the launch of the new virtual A&E service.
Results In the 12 days following the service launch, 331 patients were seen by video consultation. 78.6% of patients (n=260) were determined not to need hospital A&E review and were managed with advice (n=126), remote prescription (n=57), general practitioner referral (n=27), direct referral to hospital subspecialty services (n=26) or diversion to a local eye unit (n=24). Mean patient satisfaction was 4.9 of 5.0 (n=62). The mean consultation duration was 12 min (range 5–31 min) and the wait time was 6 min (range 0–37 min).
Conclusion Video consultations showed greater than expected usefulness in the remote management of eye disease and supported a substantial reduction in the number of people visiting the hospital.
- health care
- patient care
- medical informatics
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
As a result of the COVID-19 pandemic, the British government enforced a national lockdown on 23 March 2020. Hospitals were required significantly to reduce outpatient services both to support social distancing and to allow National Health Service (NHS) resources to be diverted to acute care. Ophthalmology is the largest outpatient specialty in the UK, and the reduction in routine care risked allowing an epidemic of preventable blindness. The simultaneous shutdown of most high street optometry provisions further reduced access to urgent eye care.
The challenge facing Moorfields Eye Hospital (MEH) Foundation Trust was twofold: to deliver care to symptomatic patients reluctant to seek help outside of their homes and to determine which patients really did need to come into the hospital for further assessment.
Video consultations offer a partial solution in many specialties, though traditional thinking held that they are not well suited to ophthalmology. In Scotland, video consultations are being used to support live streaming of biomicroscopic eye examinations between ‘Emergency Eyecare Treatment Centres’ and hospital ophthalmologists.1 In this paper, we describe the creation of a virtual accident and emergency (A&E) teleophthalmology service at MEH to provide video consultations directly between patients and hospital doctors. This service supports drop-in access without a referral (as a traditional A&E does), allows low-risk patients to be managed without visiting the hospital and accepts higher-risk patients into a less crowded A&E for traditional care.
Methods
‘Attend Anywhere’ (Attend Anywhere Pty Ltd, Victoria, Australia) was procured by NHS England in March 2020 on behalf of secondary care to allow the national provision of video consultations. The platform supports patient-to-doctor live video consultations entirely within a web browser and is accessible from tablets and smartphones in addition to traditional laptops and PCs. Patients can access virtual waiting rooms by following a URL in their browser. The platform was taken through information governance and data security signoff processes, and a DCB-0160 clinical safety report was produced to mitigate risks that the dramatic change in practice could present.
To support the provision of a virtual drop-in service (mirroring the normal operation of the A&E department), a virtual Moorfields A&E waiting room was created, which was accessible via URL or from a link on the main Moorfields website. Suitable patients contacting our nurse-led telephone lines were signposted towards the video service if judged suitable. The service was also advertised via social media and word-of-mouth among local general practitioners (GPs) and community optometry providers.
Staff training was conducted remotely on the platform by two trainee ophthalmologists (CK and AT, third year of training). Training took 15 min and covered platform access, managing technical issues, troubleshooting and the agreed processes for patient management. Conduct during video consultations was also covered including clear instructions on documentation and escalation plans. A user manual and a quick reference guide were provided.
The virtual A&E service was launched on 25 March 2020, 36 hours after the lockdown was announced, and was open to the public from 9 am to 5 pm Monday to Friday (with weekend sessions added from 18 April). A daily clinical rota was created by the A&E service manager to allow adequate medical staffing throughout the day. Between 3 and 5 ophthalmologists were assigned to each half-day session. These included trainee ophthalmologists (years 3–6 of training), trust-grade doctors, fellows and consultants. Initially, the clinical staff were volunteers or those self-isolating. As the clinic grew in popularity and MEH moved to an emergency-only model, doctors from other services were redeployed to provide video consultations.
The service was open to new and existing MEH patients, and doctors performing video consultations had access to the OpenEyes electronic patient record and scanned historical A&E notes. After each consultation, a letter was written on OpenEyes to the GP and the patient outlining the consultation. The encounter was recorded and coded on the hospital’s emergency care patient administration system to ensure contemporaneous records and accurate Trust payment reconciliation. If senior input or advice was required, the team used a secure and approved clinical instant messaging application to communicate patient details (Pando, Forward Clinical Ltd, London, UK). This was also used to inform the A&E team about referred patients in order to improve the in-hospital triage process.
To facilitate audit, a record was kept of key consultation details and management plan including whether the patient was referred for a face-to-face visit. Analysis of number of callers, duration of calls, number of calls in each virtual waiting room and service provider activity were generated by a bespoke ‘R Shiny’ application,2 the current build of which is available at https://github.com/pbmthomas/AAdash. Data can be exported from the Attend Anywhere web interface for upload to this app.
Results
An audit was undertaken of the first 12 days of the new service, during which 331 video consultations occurred. Figure 1 illustrates the daily A&E video consultation volume in the 6 weeks after launch. 78.6% (260/331) of patients managed through the virtual A&E service avoided hospital attendance. The mean consultation was 12 min (range 5–31 min) and the mean patient wait time in the virtual waiting room was 6 min (range 0–37 min) compared with mean of 2 hours and 8 min for an in-person visit.
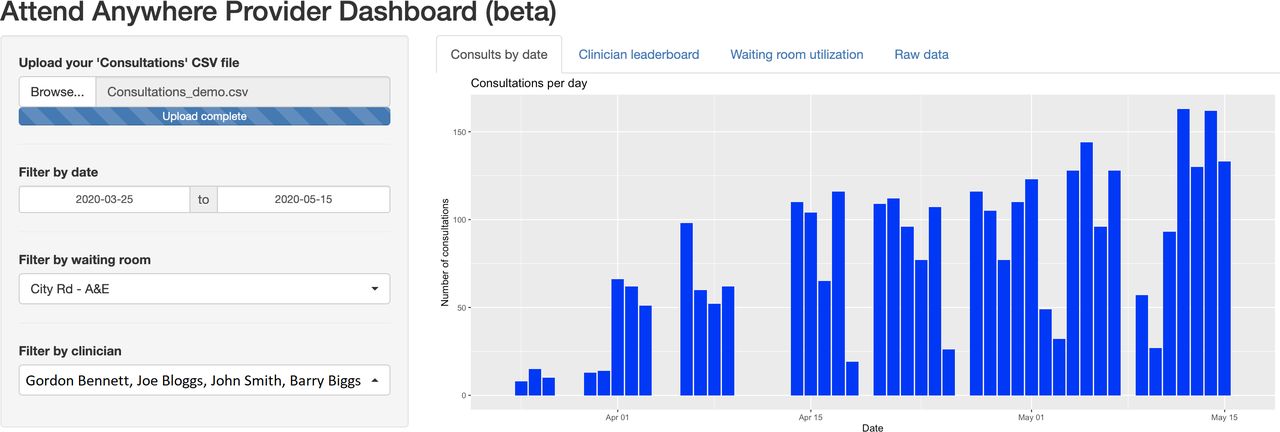
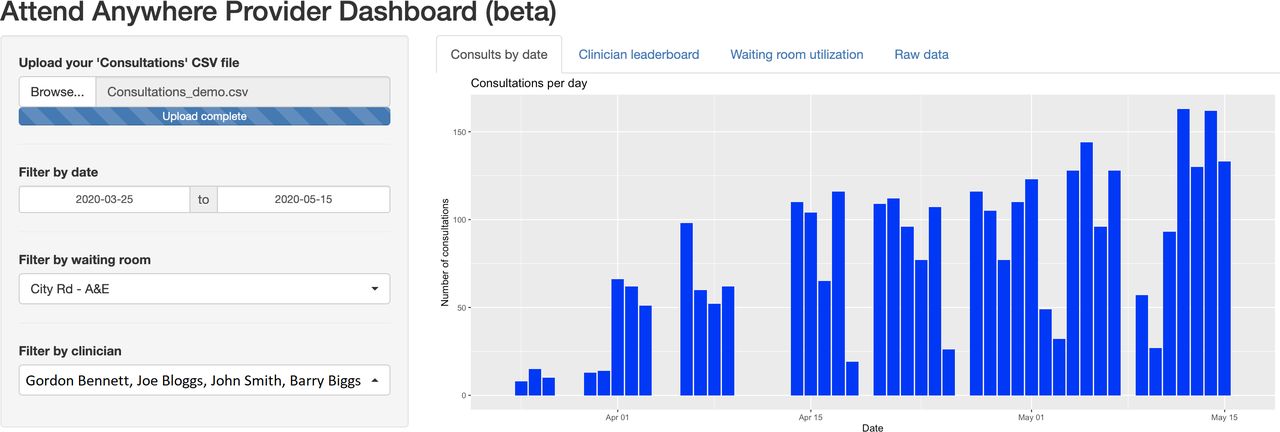{kind=link}
Growth of the Moorfields’ virtual A&E service following launch on 25 March 2020 until 15 May 2020, visualised in the bespoke R/Shiny app. A&E, accident and emergency department.
Following video consultation, 21.4% of patients (n=71) were determined to need hospital review. Their presenting complaints are summarised in table 1. Most patients did not require referral; the most common presentations for this cohort are summarised in table 2, and the management plans for these patients are summarised in table 3.
Common presentations in a cohort of patients referred to A&E for face-to-face review
Common presentations in a cohort of patients not requiring referral to A&E for face-to-face review
Management actions for patients not requiring referral to A&E for a face-to-face review
The team received positive feedback from patients, via the SMS feedback service, and social media sites. Table 4 summarises the patient rating for the service and feedback comments for lower ratings. The most common compliments of the service were regarding time efficiency and local management. Internet connectivity was the most common complaint. We now offer all patients the opportunity to fill in a feedback form online at the termination of their video consultation.
Patient service rating and feedback comments
Discussion
In recent years, virtual consultations have gained popularity, both within the NHS and commercially. A study by GPs in 2019 found that video consultations appeared suitable for simple presentations.3 Patients were more confident using virtual methods if the consultation was a follow-up and if they had received a diagnosis previously.4
Virtual clinics in ophthalmology are not new; in 2018, 50.0% of UK hospital eye service units in NHS Trusts were using glaucoma virtual clinics, with a further 21.4% planning to introduce such a service.5 A recent innovation at MEH has focused on allowing store-and-forward methodologies pioneered in these hospital-based virtual clinics to extend to community optometry data collection.6
Owing to the dependence on in-person examination using slit-lamp biomicroscopy, however, video consultations have traditionally been thought of as a niche technology in ophthalmology. The ongoing COVID-19 outbreak has provided a unique opportunity to challenge these preconceptions. The service described here shows clear application both in supporting social distancing during the current crisis (by dramatically reducing the number of hospital visits) and in managing simple patients at home or signposting to more appropriate services when normality is restored. We have also deployed video consultations to other services and have recently published our initial experience in scheduled oculoplastic clinics7 where we find similar levels of patient satisfaction (92% of patients indicating they would recommend the service to others). It will be important to benchmark video consultations in each clinical domain to determine the most appropriate case mix and management algorithms.
Strengths
The benefits of the emergency video consultation service go beyond the obvious reduction in viral transmission for both staff and patients. Patients spend significantly less time waiting for their consultation and forgo the time usually spent travelling (though some will have to visit the hospital if the clinician feels this is necessary following video consultation). The service allowed staff members with underlying health conditions, pregnant and those who were self-isolating to continue clinical work in a safe environment, reducing the burden on their non-isolating colleagues.
Clear communication established between IT, clinical informatics services, clinicians and senior management was a key facilitator in the rapid pace at which video consultations were implemented and scaled. Robust clinical processes ensured safe and effective running of the service and parallel administrative processes enabled tracking of service use, audit and supported accurate Trust payment.
Digital accessibility of the platform was demonstrated in this study with a wide variation in the age of patients using the platform (0–92 years; paediatric attendees were accompanied by a parent). Very few patients experienced difficulty managing the technological aspect of video consultation though we recognise that the use of such services produces bias due to a self-selecting population. There were, however, a few examples of poor internet connectivity—in these cases, the consultation was converted to a telephone consultation.
Accessibility and public awareness of the service were further enhanced with robust patient signposting on the MEH website and through multiple social media and communication channels. Following COVID-19 lockdown, Moorfields eye casualty attendances reduced from approximately 250 patients per day to an average of 64. Meanwhile, an average of 38 patients were seen daily via video consultation in the first 12 days, increasing to around 150 daily at the time of writing. A typical A&E attendance would earn the trust approximately £180, whereas a video consultation earns £73 at lower overhead costs to the Trust. The advantage of the low cost of video consultation platforms and their ability to support flexible working without utilising hospital estate may make them an attractive option for longer-term service planning. During the COVID-19 crisis, a block contract is in place to cover clinical activity—a favourable arrangement for video consultations. It is currently unclear how video consultations will be funded post-COVID-19 crisis, but anticipated changes in hospital reimbursement systems should support their continued use.
Weaknesses
In a health service built around traditional face-to-face consultations, a move to virtual consultations presents several challenges. During the COVID-19 crisis, the reduction in routine outpatient activity across the trust made adequate staffing available to support a rapidly growing service. Following the resumption of routine services, sufficient staffing will need to be ensured through modification of duty rosters and longer-term job planning.
From a clinical management perspective, a significant challenge was encountered in getting medications to patients who were not physically on-site. Where possible, local GPs were contacted and the prescription sent to the patient’s local pharmacy for collection. There were occasional delays, resulting in multiple consultations with the same patient throughout the day. Following these, liaison with the MEH pharmacy team resulted in the development of a service to post medications to patients. Although most patients utilising the service were London-based, there were calls from other areas in the UK. There will be a need in the future to identify those calling from out-of-area to advise them to contact local eye units.
Naturally, it was made clear to patients that the video consultation is not an examination tool. However, lid and periorbital signs could be assessed to some extent, and several ocular surface and anterior segment (front of the eye) signs could be detected (eg, presence of hypopyon, and bilaterality, type and severity of conjunctival hyperaemia). Crude estimates of visual acuity could also be reached. Those presenting with features of intraocular inflammation, raised intraocular pressure or those with posterior segment symptoms had to be referred in for formal ophthalmic examination. Devices and smartphone-attached optics, for example, could allow a more capable objective examination of a patient’s eye via video consultation in the future. Home vision monitoring apps show promise in allowing a remote and objective assessment of patient vision, either during a video consultation or asynchronously.
Much remains unknown about video consultations in routine teleophthalmology practice Acknowledging this, we have embedded formal monitoring of activity in our video consultation services. Operationally, we have rolled out an internal dashboard to track video consultation activity across all services. Clinically, services are undertaking audits to describe the safety and clinical outcomes of video consultations. In A&E, for example, we are actively monitoring patients with an unplanned return following a video consultation. This work will inform the clinical scenarios within which video consultations are indicated, triggers for clinical escalation and the clinical safety case for the platform. Finally, patient satisfaction is now continuously monitored using surveys presented at the end of a consultation. It will be important to continue these processes as NHS services return to normal. The current COVID-19 lockdown produces a host of potentially confounding variables that could affect video consultation use and suitability, including changes in patient desire to avoid hospital visits; clinicians’ risk assessment; available clinician time for video consultations; availability of in-person services; and the reopening of high street optometry.
Conclusion
The COVID-19 crisis has created the opportunity to rethink traditional beliefs about the usefulness of digital health technologies. The Moorfields Virtual A&E service is an excellent example; although video consultations are often written off as unsuitable for most ophthalmological care, the service described here has proven successful in reducing unnecessary hospital visits and has done so in a manner that is cost-effective and time-efficient for both patients and doctors.
Implementation of similar projects requires a partnership between the host clinical service and a hospital’s digital transformation unit. Buy-in from senior clinicians, management and local champions is critical in demonstrating the capabilities of novel digital services and in reframing the argument away from ‘what is not possible’ using a new approach towards ‘what is possible?’. Challenges that arise are solvable by early involvement of relevant stakeholders, for example, in rapidly scaling the number of clinicians able to access hospital systems from home to support the service.
At Moorfields, we are now launching or scaling up video consultation services across a range of our routine outpatient services. With effective change management, a service born of necessity during the COVID-19 pandemic can become a sustainable model that offers more efficient and accessible care closer to home for our patients into the future.
Footnotes
CLK and AAT are joint first authors.
Twitter @KilduffCaroline, @AliceTh29651183, @clairerobo84, @dawnasim, @gordonrhay_md, @pbmthomas
Contributors All authors contributed to implementation of the service described and to the writing or review of the paper. CK and AT are joint first authors and contributed equally to all aspects of this work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. Video consultation data is available via the forthcoming NHSE&I national dashboard. Summary video consultation data relevant to the cohort described in this paper can be provided upon request.