
Abstract
Purpose
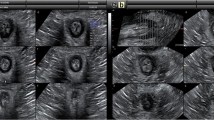
This report describes the advantages of 3D anal endosonography in depicting the normal anatomy of the anal canal in relation to sex and age.
Materials and methods
A retrospective study was performed of 85 patients, 33 men and 52 women, previously examined with 3D anal ultrasound (US) for clinically suspected anorectal disease but found to be negative. The examinations were performed with a Bruel and Kjaer US system with a 2050 transducer, scanning from the anorectal junction to the subcutaneous portion of the external anal sphincter (EAS). The 3D reconstructions provided an estimation of sphincter length in the anterior and posterior planes, and axial 2D images enabled calculation of the thickness of the internal anal sphincter (IAS) and EAS in the anterior, posterior and lateral transverse planes.
Results
Distribution of the sphincter complex is asymmetric in both sexes: the EAS and IAS are significantly shorter in females, especially in the anterior longitudinal plane (p=0.005 and p<0.001, respectively). EAS and IAS thickness increases with age, especially the lateral IAS (R2=0.37, p<0.001) and the posterior EAS (R2=0.29, p=0.01).
Conclusions
A good knowledge of anal-canal anatomy is essential to detect sphincter abnormalities when assessing pelvic floor dysfunction.
Riassunto
Obiettivo
Scopo del presente lavoro è stato documentare la rappresentazione anatomica normale del canale anale attraverso l’ultrasonografia (US) endoanale 3D, in relazione al sesso e all’età.
Materiali e metodi
In uno studio retrospettivo sono stati selezionati 85 soggetti, di cui 33 maschi e 52 femmine, sottoposti precedentemente ad US endoanale 3D per sospetto clinico di patologia dell’ano-retto distale ma risultati essere tutti negativi all’esame ultrasonografico. Gli esami sono stati eseguiti con apparecchio dedicato Bruel e Kjaer, con trasduttore tipo 2050 e scansioni dalla giunzione ano-rettale alla porzione più superficiale dello sfintere anale esterno (SAE). Nell’immediato postprocessing sono stati stimati la lunghezza degli sfinteri nei piani anteriore e posteriore e lo spessore anteriore, laterale e posteriore dello sfintere anale interno (SAI) e del SAE.
Risultati
La distribuzione della muscolatura del canale anale risulta asimmetrica in entrambi i sessi: la lunghezza di SAI e SAE è significativamente più breve nelle donne, specie lungo il piano longitudinale mediano anteriore (p=0,005 e p<0,001, rispettivamente). Inoltre, lo spessore di entrambi gli sfinteri presenta una tendenza all’accrescimento proporzionale all’età del paziente, soprattutto nella porzione laterale per il SAI (R2=0,37, p<0,001) e posteriore per il SAE (R2=0,29, p=0,01).
Conclusioni
La conoscenza precisa delle componenti anatomiche muscolo-legamentose del canale anale è alla base della identificazione delle alterazioni sfinteriali utili alla comprensione dei disturbi del pavimento pelvico.
Similar content being viewed by others


References/Bibliografia
Bogduk N (1996) Issues in anatomy: the external anal sphincter revisited. Aust NZJ Surg 66:626–629
Nielsen MB, Pedersen JF, Hauge C et al (1991) Endosonography of the anal sphincter: findings in healthy volunteers. AJR Am J Roentgenol 157:1199–1202
Brunese L, Amitrano M, Gargano V et al (1996) Anal endosonography: the study technique and the correlations between the normal and echographic anatomy. Radiol Med 91:253–257
Brunese L, Amitrano M, Gargano V et al (1996) Role of anal endosonography in inflammation and trauma of the anal canal. Radiol Med 92:742–747
Bartram CI, Frudinger A (1997) Handbook of anal sonography, 1st edn. Wrightsone Biomedical, Petersfield
Frudinger A, Bartram CI, Halligan S et al (1998) Examination techniques for endosonography of the anal canal. Abdom Imaging 23:301–303
Frudinger A, Halligan S, Bartram CI et al (2002) Female anal sphincter: age-related differences in asymptomatic volunteers with high-frequency endoanal US. Radiology 224:417–423
Pomerri F, Dodi G, Pintacuda G et al (2010) Anal endosonography and fistulography for fistula in ano. Radiol Med 115:771–783
Williams AB, Bartram CI, Halligan S et al (2001) Anal sphincter damage after vaginal delivery using three-dimensional endosonography. Obstet Gynecol 97:770–775
Williams AB, Cheetham MJ, Bartram CI et al (2000) Gender differences in the longitudinal pressure profile of the anal canal related to anatomical structure as demonstrated on three-dimensional anal endosonography. Br J Surg 87:1674–1679
Gold DM, Bartram CI, Halligan S et al (1999) Three-dimensional endoanal sonography in assessing anal canal injury. Br J Surg 86:365–370
Thakar R and Fenner DE (2007) Anatomy of the perineum and the anal sphincter. In: Sultan AH, Thakar R, Fenner D (eds) Perineal and anal sphincter trauma. Springer, London, pp 1–12
Damon H, Henry L, Roman S et al (2003) Influence of rectal prolapse on the asymmetry of the anal sphincter in patients with anal incontinence. BMC Gastroenterology 3:23–30
Santoro GA, Wieczorek AP, Dietz HP et al (2011) State of the art: an integrated approach to pelvic floor ultrasonography. Ultrasound Obstet Gyneco 37:381–396
Bartram CI (2008) Endoanal ultrasound. In: Stoker J, Taylor SA, De Lancey JOL (eds) Pelvic floor disorders. Springer, Berlin, pp 101–113
Santoro GA, Di Falco G (2006) Endosonographic anatomy of the normal anal canal. In: Santoro GA, Di Falco G (eds) Benign anorectal diseases. Diagnosis with endoanal and endorectal ultrasonography and new treatment options. Springer-Verlag, Milan, pp 35–52
Santoro GA, Di Falco G (2010) Endoanal and endorectal ultrasonography: methodology and normal pelvic floor anatomy. In: Santoro GA, Wieczorek AP, Bartram CI (eds) Pelvic floor disorders. Springer, London, pp 91–102
Stoker J, Bartram CI, Halligan S (2002) Imaging of the posterior pelvic floor. Eur Radiol 12:779–788
BK Medical Group (2008) 3D Anorectal ultrasound. Anorectal endosonography. Application Note
Starck M, Bohe M, Fortling B et al (2005) Endosonography of the anal sphincter in women of different ages and parity. Ultrasound Obstet Gynecol 25:169–176
West RL, Felt-Bersma RJF, Hansen BE et al (2005) Volume measurements of the anal sphincter complex in healthy controls and fecal-incontinent patients with a three-dimensional reconstruction of endoanal ultrasonography images. Dis Colon Rectum 48:540–548
Regadas FSP, Regadas SMM, Lima DMR et al (2007) Anal canal anatomy showed by three-dimensional anorectal ultrasonography. Surg Endosc 21:2207–2211
Knowles AM, Knowles CH, Scott SM et al (2008) Effect of age and gender on three-dimensional endoanal ultrasonography measurements: development of normal ranges. Tech Coloproctol 12:323–329
Esclapez-Valero JP and Garcia-Botello S (2005) Current utility of endoanal ultrasound in the diagnosis of benign proctological disease. Cir Esp 78:8–14
Regadas SM, Regadas FS, Rodrigues LV et al (2005) Importance of the three-dimensional ultrasound in the anorectal evaluation. Arq Gastroenterol 42:226–232
Rotondo A, Romano S, D’Andrea A et al (2006) Patologia del perineo posteriore. In: Gugliemi G, Schiavon F, Cammarota T (eds) Radiologia geriatrica. Springer-Verlag Italia, Milano, pp 425–436
Norderval S, Dehli T, Vonen B (2009) Three-dimensional endoanal ultrasonography: intraobserver and interobserver agreement using scoring systems for classification of anal sphincter defects. Ultrasound Obstet Gynecol 33:337–343
Granata V, Mandato Y, Russo A et al (2010) Imaging delle disfunzioni del pavimento pelvico. In: Blandino A, Rotondo A, Danza F, Menchi I, Pozzi Mucelli R (eds) Imaging dell’apparato uro-genitale: patologia non oncologica, Springer-Verlag Italia, Milano, pp 175–191
Reginelli A, Pezzullo MG, Scaglione M et al (2008) Gastrointestinal disorders in elderly patients. Radiol Clin North Am 46:755–771
Regadas FSP, Murad-Regadas SM, Wexner SD et al (2007) Anorectal three-dimensional endononography and anal manometry in assessing anterior rectocele in women a new pathogenesis concept and the basic surgical principle. Colorectal Dis 9:80–85
Bollard RC, Gardiner A, Lindow S et al (2002) Normal female anal sphincter: difficulties in interpretation explained. Dis Colon Rectum 45:171–175
Engin G (2006) Endosonographic imaging of anorectal disease. J Ultrasound Med 25:57–73
Berton F, Gola G, Wilson RS (2007) Sonography of benign conditions of the anal canal: an update. AJR Am J Roentgenol 189:765–773
Gregory WT, Boyles SH, Simmons K et al (2006) External anal sphincter volume measurements using three-dimensional endoanal ultrasound. Am J Obstet Gynecol 194:1243–1248
Santoro GA, Fortling BEE (2006) The advantages of volume rendering in three-dimensional endosonography of the anorectum. Dis Colon Rectum 50:359–368
Saranovic D, Barisic G, Krivokapic Z et al (2007) Endoanal ultrasound evaluation of anorectal diseases and disorders: technique, indications, results and limitations. Eur J Radiol 61:480–489
Savoy-Collet C, Konig E, Dacher JN (2008) Radiologic evaluation of pelvic floor disorders. Gastroenterol Clin N Am 37:553–567
De la Portilla F, Lopez-Alonso M (2009) Endosonography of the anal canal: findings in children. Dis Colon Rectum 52:711–714
Bartram CI and Sultan AH (2007) Imaging of the anal sphincter. In: Sultan AH, Thakar R, Fenner D (eds) Perineal and anal sphincter trauma, diagnosis and clinical management, Springer, London, pp 123–132
Bader FG, Bouchard R, Keller R et al (2008) Progress in diagnostics of anorectal disorders. Part I: anatomic background and clinical and neurologic procedures. Chirurg 79:401–409
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Reginelli, A., Mandato, Y., Cavaliere, C. et al. Three-dimensional anal endosonography in depicting anal-canal anatomy. Radiol med 117, 759–771 (2012). https://doi.org/10.1007/s11547-011-0768-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11547-011-0768-4