Effect of exercise training for five years on all cause mortality in older adults—the Generation 100 study: randomised controlled trial
BMJ 2020; 371 doi: https://doi.org/10.1136/bmj.m3485 (Published 07 October 2020) Cite this as: BMJ 2020;371:m3485Linked Opinion
It’s never too late for older adults to start exercising

- Dorthe Stensvold, professor1,
- Hallgeir Viken, researcher1,
- Sigurd L Steinshamn, professor12,
- Håvard Dalen, professor134,
- Asbjørn Støylen, professor14,
- Jan P Loennechen, professor14,
- Line S Reitlo, postdoctoral student1,
- Nina Zisko, researcher1,
- Fredrik H Bækkerud, doctoral student1,
- Atefe R Tari, doctoral student1,
- Silvana B Sandbakk, researcher1,
- Trude Carlsen, doctoral student1,
- Jan E Ingebrigtsen, associate professor5,
- Stian Lydersen, professor6,
- Erney Mattsson, professor1,
- Sigmund A Anderssen, professor7,
- Maria A Fiatarone Singh, professor8,
- Jeff S Coombes, professor9,
- Eirik Skogvoll, professor110,
- Lars J Vatten, professor11,
- Jorunn L Helbostad, professor12,
- Øivind Rognmo, associate professor1,
- Ulrik Wisløff, professor19
- 1Department of Circulation and Medical Imaging, Faculty of Medicine and Health Sciences, NTNU-Norwegian University of Science and Technology, Post Box 8905, 7491 Trondheim, Norway
- 2Department of Thoracic Medicine, Clinic of Thoracic and Occupational Medicine, St Olavs University Hospital, Trondheim, Norway
- 3Levanger Hospital, Nord-Trøndelag Hospital Trust, Levanger, Norway
- 4Department of Cardiology, St Olavs University Hospital, Trondheim, Norway
- 5Department of Sociology and Political Science, Faculty of Social Sciences and Technology Management, NTNU-Norwegian University of Science and Technology, Trondheim, Norway
- 6Regional Centre for Child and Youth Mental Health and Child Welfare, NTNU-Norwegian University of Science and Technology, Trondheim, Norway
- 7Department of Sports Medicine, The Norwegian School of Sport Sciences, Oslo, Norway
- 8Exercise Health and Performance Faculty Research Group, Faculty of Health Sciences, The University of Sydney, Lidcombe, Australia
- 9School of Human Movement and Nutrition Science, University of Queensland, Queensland, Australia
- 10Department of Anaesthesia and Intensive Care Medicine, St Olavs University Hospital, Trondheim, Norway
- 11Department of Public Health and General Practice, Faculty of Medicine, NTNU-Norwegian University of Science and Technology, Trondheim, Norway
- 12Department of Neuromedicine and Movement Science, Faculty of Medicine and Health Sciences, NTNU-Norwegian University of Science and Technology, Trondheim, Norway
- Correspondence to: U Wisløff ulrik.wisloff{at}ntnu.no (or @uwisloff on Twitter)
- Accepted 24 August 2020
Abstract
Objective To evaluate the effect of five years of supervised exercise training compared with recommendations for physical activity on mortality in older adults (70-77 years).
Design Randomised controlled trial.
Setting General population of older adults in Trondheim, Norway.
Participants 1567 of 6966 individuals born between 1936 and 1942.
Intervention Participants were randomised to two sessions weekly of high intensity interval training at about 90% of peak heart rate (HIIT, n=400), moderate intensity continuous training at about 70% of peak heart rate (MICT, n=387), or to follow the national guidelines for physical activity (n=780; control group); all for five years.
Main outcome measure All cause mortality. An exploratory hypothesis was that HIIT lowers mortality more than MICT.
Results Mean age of the 1567 participants (790 women) was 72.8 (SD 2.1) years. Overall, 87.5% of participants reported to have overall good health, with 80% reporting medium or high physical activity levels at baseline. All cause mortality did not differ between the control group and combined MICT and HIIT group. When MICT and HIIT were analysed separately, with the control group as reference (observed mortality of 4.7%), an absolute risk reduction of 1.7 percentage points was observed after HIIT (hazard ratio 0.63, 95% confidence interval 0.33 to 1.20) and an absolute increased risk of 1.2 percentage points after MICT (1.24, 0.73 to 2.10). When HIIT was compared with MICT as reference group an absolute risk reduction of 2.9 percentage points was observed (0.51, 0.25 to 1.02) for all cause mortality. Control participants chose to perform more of their physical activity as HIIT than the physical activity undertaken by participants in the MICT group. This meant that the controls achieved an exercise dose at an intensity between the MICT and HIIT groups.
Conclusion This study suggests that combined MICT and HIIT has no effect on all cause mortality compared with recommended physical activity levels. However, we observed a lower all cause mortality trend after HIIT compared with controls and MICT.
Trial registration ClinicalTrials.gov NCT01666340.

{kind=link}
Introduction
The physical activity guidelines state that being physically active is one of the most important measures individuals of all ages can take to improve their health.1 The multiple benefits of exercise on physical function and physical performance are well known,2 and short term randomised controlled trials have shown that exercise training improves traditional risk factors for lifestyle related diseases and premature death.34 In line with this, observational studies suggest that exercise has a statistically significant preventive effect on premature all cause mortality,567 with active individuals showing up to a 72% lower risk of premature mortality from all causes compared with inactive individuals.8 The guidelines for physical activity are relatively consistent worldwide.9 The benefits of exercise on mortality and morbidity, however, have not been assessed in the setting of a randomised controlled trial. Nor have the effects of different intensities of physical activity been reported on hard endpoints, despite high intensity exercise being shown to induce greater effects on health measures than moderate intensity exercise.31011 Sceptics of the benefits from physical activity have argued that the guideline recommendations lack the high quality evidence provided by randomised clinical trials.2 Real life randomised exercise trials with sufficient statistical power covering adults of most ages is challenging because a large sample size and long and costly follow-up is needed as death is relatively rare in young and middle aged people. The rapidly aging population and higher death rates among older adults make this population particularly interesting for testing whether a causal relation exists between the current advice on physical activity levels and longevity.2 In a general population of older adults aged 70-77 years in Norway, we tested the primary hypothesis that systematic exercise training lowers all cause mortality compared with giving advice to follow the national guidelines for physical activity. We also examined an exploratory hypothesis that high intensity interval training lowers mortality more than moderate intensity continuous training.
Methods
Study design
Generation 100 is a randomised controlled trial conducted in Trondheim, Norway. Participants were randomised 2:1:1, stratified by sex and cohabitation status (living with someone versus alone) to either following the national guidelines for physical activity (control group, n=780), moderate intensity continuous training (MICT, n=387), or high intensity interval training (HIIT, n=400).12 To ensure impartiality in allocation, the Unit for Applied Clinical Research at the Norwegian University of Science and Technology performed the randomisation.
Participants
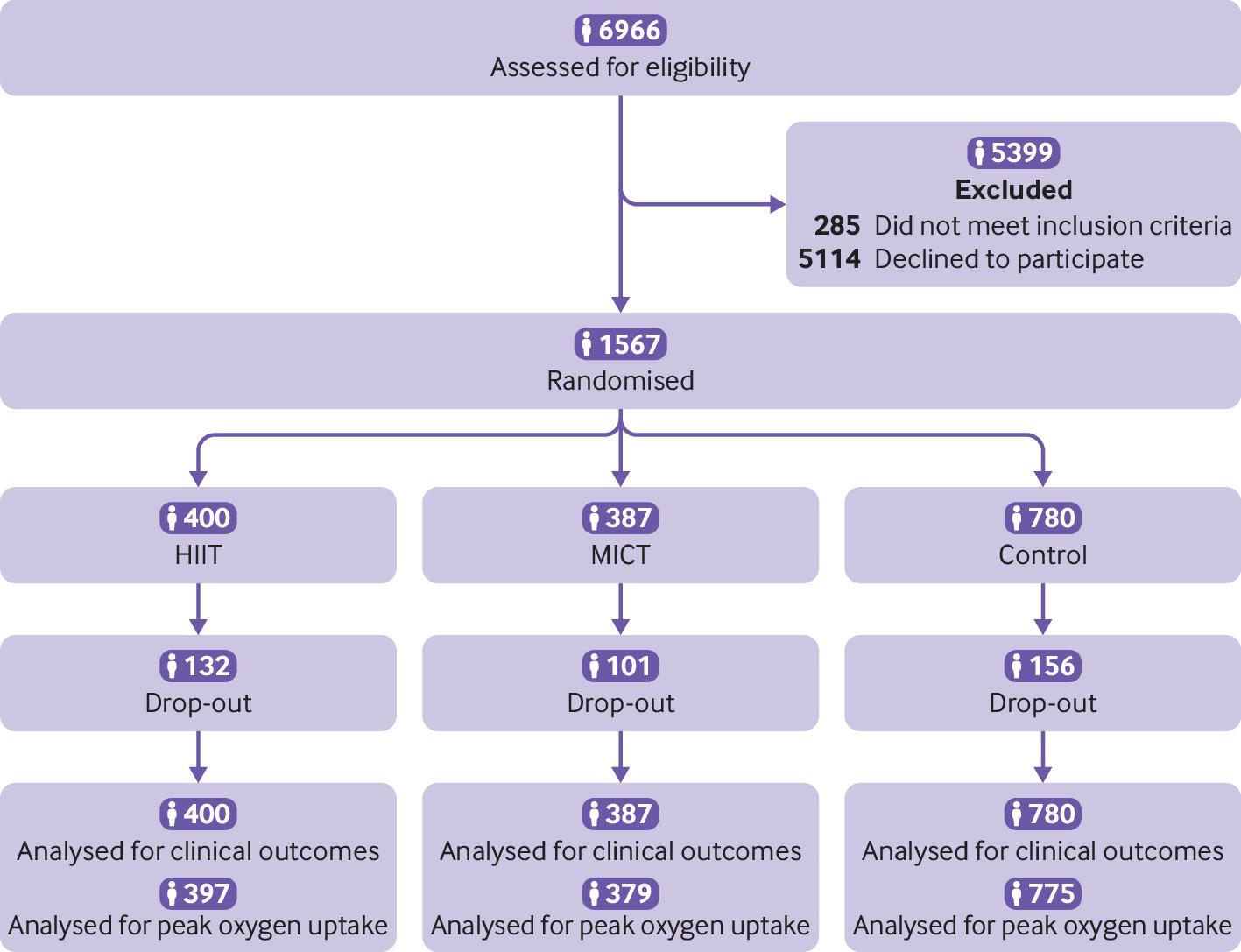
In 2012, we invited all inhabitants of Trondheim, Norway, aged 70-77 years (born 1 January 1936 to 31 December 1942, n=6966) to participate in the study. Exclusion criteria before and during the study were uncontrolled hypertension (untreated systolic blood pressure >220 mm Hg, or diastolic blood pressure >110 mm Hg); symptomatic valvular disease; hypertrophic cardiomyopathy; unstable angina pectoris; primary pulmonary hypertension; heart failure; severe arrhythmia; diagnosed dementia; cancer that made participation impossible; chronic communicable infectious diseases, illness, or disabilities that precluded exercise; or participation in other exercise trials. In total, 1567 (790 women) older adults were included at baseline screening (fig 1) and invited for follow-up screening after one, three, and five years.12

Flowchart of study cohort. HIIT=high intensity interval training; MICT=moderate intensity continuous training
{kind=link}
Primary and secondary outcomes
The primary aim of this study was to investigate the effect of exercise on mortality. This study includes several secondary outcomes (see study protocol in supplementary appendix), most of which will be presented in separate papers. Here we report the secondary outcomes of disease specific mortality (cardiovascular disease and cancer) as well as cardiorespiratory fitness and health related quality of life. Cardiorespiratory fitness, measured as maximal oxygen uptake, is currently regarded as the single best predictor of longevity and health and is the best measure to evaluate the training effect of the exercise regimens used in the current study. Also, we chose to report health related quality of life as it is of major interest in clinical trials.
Intervention and adherence to exercise
Participants allocated to the control group were asked to follow the Norwegian physical activity guidelines for 2012, which state 30 minutes of moderate level physical activity almost every day.13 No further supervision was given. Participants randomised to HIIT and MICT were asked to exchange two of the five 30 minute moderate intensity physical activity sessions each week (as recommended by Norwegian health authorities) with two HIIT sessions (10 minute warm-up followed by 4×4 minute intervals at about 90% of peak heart rate corresponding to rating of perceived exertion of about 16 on the Borg scale; from 6 for no exertion to 20 for maximum exertion) or two isocaloric4 MICT sessions (50 minutes of continuous work at about 70% of peak heart rate corresponding to rating of perceived exertion of about 13) for five years, respectively. Every sixth week both groups met separately for supervised spinning sessions (ergometer cycling) with an exercise physiologist, where they exercised with heart rate monitors to ensure recommended exercise intensities were being achieved. Supervised training with exercise physiologists present was also offered twice a week in different outdoor areas. Exercise intensity was evaluated by heart rate monitors and rating of perceived exertion during the supervised sessions. Adherence to the prescribed exercise programme was obtained from a validated questionnaire14 at one, three, and five years follow-up (supplementary appendix, table S3). Non-adherence was defined as having performed less than 50% of the prescribed training sessions over the five years.12
Follow-up and clinical outcomes
An endpoint committee of two physician specialists evaluated outcomes blinded to group allocation. Number and causes of death were provided by the Norwegian Cause of Death Registry and Norwegian Population Registry. We identified clinical outcomes from diagnoses or procedures in the patient archives of the community hospitals (supplementary appendix). Diagnoses and procedure codes were reported according to ICD-9 and ICD-10 (international classification of diseases, ninth and 10th revisions, respectively). All cardiovascular diseases were identified, in addition to the subcategories of acute myocardial infarction, unstable angina pectoris, coronary revascularisation, stroke, atrial fibrillation, atrial flutter, supraventricular or ventricular tachycardia, cardiac arrest, heart failure, peripheral artery disease treated by endovascular or surgical methods, and dissection or rupture in the vasculature. We defined cardiovascular events as a valid diagnosis of, or death from, cardiovascular disease, whichever came first. In addition to recording a diagnoses of breast cancer, prostatic cancer, cancer of the gastrointestinal tract, and cancer of the respiratory system, we also recorded all cancer diagnosis. We defined cancer events as a valid diagnosis of, or death from, cancer, whichever came first (supplementary appendix). Data on prescription drugs were retrieved from the Norwegian Prescription Database (supplementary appendix).
Peak oxygen uptake and health related quality of life
Ergospirometry was used to measure peak oxygen uptake at baseline and after one, three, and five years and is described in detail elsewhere.15 As 41% of the participants did not meet the criteria for maximal oxygen uptake, we used the term peak oxygen uptake. We defined peak heart rate as five beats over the highest observed heart rate (Polar Electro, Finland) during the ergospirometry test and used this to determine exercise intensity.
Health related quality of life was measured at the one, three, and five year follow-up using the generic questionnaire SF-8, which is a short form of the SF-36.16 The SF-8 is sensitive to changes and is therefore a valuable tool when looking for a shift in overall health related to an intervention.17 We present the overall score of the physical component summary and mental component summary scores.
Safety
An independent safety manager reviewed mortality data after one, two, three, and four years. Exercise instructors reported any severe events during supervised exercise training to the medical director who determined whether further medical care was needed. Severe events included onset or worsening of cardiovascular disease or cardiovascular disease events, injuries and fractures, or any of these that led to further medical care.
Statistical analysis
We followed a predefined statistical plan (supplementary appendix). The primary outcome was all cause mortality. According to Statistics Norway, the yearly mortality rate in people aged 70-75 years was 2% in 2012. For the main analysis we combined the supervised exercise groups, MICT and HIIT, into one group and compared this group with the control group.12 With an expected 10% mortality rate after five years, we determined that 600 participants would be needed in the combined MICT and HIIT group and control group to detect a 50% reduction in mortality (from 10% to 5%),518 with power 90%. We also evaluated the relation between exercise intensities (HIIT versus MICT versus control) and clinical outcomes. Baseline characteristics are presented as means and standard deviations or percentages and numbers. We performed intention-to-treat analyses; thus, all participants were included in the analysis. Hazard ratios and 95% confidence intervals were obtained using Cox proportional hazard models, adjusted for the stratification variables sex, cohabitation status, and age at study entry. Survival was assessed by Kaplan-Meier survival analysis. We used linear mixed models to analyse changes in peak oxygen uptake and SF-8, with peak oxygen uptake or physical and mental component scores as dependent variables, person as random effect, and sex, cohabitation status, and age at baseline as covariates. Normality of residuals was confirmed by visual inspection of Q-Q (quantile-quantile) plots. Sixteen participants lacked information on peak oxygen uptake at all examinations and were excluded from this analysis. We considered a P value of <0.05 to be statistically significant. The statistical analyses were performed with the IBM SPSS statistics 25.0 program.
Patient and public involvement
Participant representatives were invited to discuss the study about six months before applying to the regional ethical committee for approval. Also, participants from the Norwegian Directorate of Health took part in the planning of the project at that stage. The lead authors (DS, ØR, and UW) conceived the study and formed the initial research questions, which were discussed first with a steering committee (see supplementary appendix for details) before presenting it to user representatives and public bodies (Norwegian Directorate of Health). Research questions remained the same after discussion with participants, but we adapted the exercise training. For instance, the participants wanted to receive instruction on how to perform the training and regular meeting points where they could exercise with their peers. We therefore offered training sessions in-house every six weeks in addition to two weekly sessions in different outdoor areas in Trondheim all year round for the study period. We presented our ideas to a large group of older adults in Trondheim and asked for initial inputs. Thereafter, we had smaller group meetings with some of the representatives who gave specific inputs on behalf of the group. Participants were not involved in the recruitment of the study. However, we had yearly interactive meetings with the participants to evaluate the process of the study—for example, we stopped requiring daily training diaries after one year as several participants found them a burden to complete and this affected their motivation to participate. We also established a webpage with weekly information for participants and a contact who could be reached eight hours a day by email or phone.
Results
Participants
Of the 1567 participants included in the study, 387 were assigned to MICT, 400 to HIIT, and 780 to follow the Norwegian guidelines for physical activity (control group). Table 1 presents the baseline characteristics of the participants. Overall mean age was 72.8 (SD 2.1) years and body mass index was 26.0 (SD 3.6). The overall prevalence of cardiovascular disease was 17.4% (n=273), and 16.7% (n=263) had previously received a diagnosis of cancer. In total, 87.5% of participants reported overall good health. No group differences were observed at baseline.
Baseline characteristics of participants assigned to three types of physical activity. Values are percentages (numbers) unless stated otherwise
Follow-up
The overall number of drop-outs (death, withdrawal, and exclusion) was 389 (24.8%), but all participants were included for statistical analysis of the primary outcome (intention-to-treat approach). The numbers of drop-outs after one, three, and five years of follow-up were 76 (19%), 104 (26%), and 132 (33%) in the HIIT group, 58 (15%), 76 (20%) and 101 (26%) in the MICT group, and 61 (8%), 95 (12%), and 156 (20%) in the control group.
Clinical outcomes
The observed mortality rate after five years was 4.6% (n=72), with 4.7% (n=37) in the control group, 4.5% (n=35) in the combined MICT and HIIT group, 5.9% (n=23) in the MICT group, and 3.0% (n=12) in the HIIT group (table 2). No difference was observed in all cause mortality between the control group and combined MICT and HIIT group (table 3, fig 2). When MICT and HIIT were analysed separately, with the control group as reference, with an all cause mortality of 4.7%, an absolute risk reduction trend of 1.7 percentage points was observed after HIIT (hazard ratio 0.63, 95% confidence interval 0.33 to 1.20) and 1.2 percentage points increase after MICT (1.24, 0.73 to 2.10; table 3, fig 2). When HIIT was compared with MICT as reference group an absolute risk reduction of 2.9 percentage points was observed (0.51, 0.25 to 1.02; table 3, fig 2) for all cause mortality.
Clinical events during five years of follow-up in participants assigned to three types of physical activity. Values are percentages (numbers)
Person years, events, rates, and hazard ratios for all cause mortality in participants assigned to three types of physical activity

Kaplan-Meier curves for all cause mortality. (A) Control group (followed Norwegian guidelines for physical activity) versus combined moderate intensity continuous training (MICT) and high intensity interval training (HIIT) group. (B) Control group versus MICT and HIIT groups
{kind=link}
No differences were observed in cardiovascular disease, cancer, or related events between the control group and the combined MICT and HIIT group, or any effect of exercise intensity (table 2, supplementary appendix, tables S1 and S2). The total proportion of participants with cardiovascular disease after five years was 15.6%, with 16.0% (n=125) in the control group, 15.0% (n=58) in the MICT group, and 15.3% (n=61) in the HIIT group (table 2). The total proportion of participants with cancer after five years was 12.2%, with 12.8% (n=100) in the control group, 11.1% (n=43) in the MICT group, and 12.0% (n=48) in the HIIT group (table 2). Of the 263 participants with a history of cancer at baseline, 21 died during follow-up, all from cancer. Of the 273 with a history of cardiovascular disease at baseline, 16 died during follow-up: two from cardiovascular disease, nine from cancer, and five from other causes.
The overall numbers of participants taking prescribed drugs for cardiovascular disease in the control group at baseline and at one, three, and five years were 320 (41%), 359 (46%), 421 (54%), and 476 (61%), respectively. The corresponding numbers in the MICT group were 178 (46%), 197 (51%), 221 (57%), and 267 (69%), and in the HIIT group were 172 (43%), 192 (48%), 224 (56%), and 260 (65%).
Peak oxygen uptake
Peak oxygen uptake after one, three, and five years was 0.8 (P=0.02), 0.7 (P=0.04), and 0.3 mL/kg/min (P=0.17) higher in the combined MICT and HIIT group compared with the control group. Peak oxygen uptake was 0.7 mL/kg/min higher in the HIIT group compared with control (P=0.02) and MICT group (P=0.04) (supplementary appendix, fig S1) after five years.
Training intensity and adherence
Average exercise intensity during supervised HIIT and MICT was 90% and 72% of peak heart rate, corresponding to ratings of perceived exertion of 16.9 and 13.8 on the Borg scale, respectively. At baseline, 273 (35%) of participants in the control group, 155 (40%) in the MICT group, and 148 (37%) in the HIIT group followed national guidelines for physical activity.
Adherence to prescribed exercise after one, three, and five years was, respectively, 201 (50%), 196 (49%), and 187 (47%) of participants in the HIIT group and 244 (63%), 213 (55%), and 197 (51%) in the MICT group. Physical activity levels in the control group were stable throughout the study, with 608 (78%), 546 (70%), and 538 (69%) of participants fulfilling the national guidelines for physical activity after one, three, and five years, respectively. A crossover occurred between the interventions, particularly in the control group, with 179 (23%), 172 (22%), and 140 (18%) changing to HIIT after one, three, and five years, respectively. The corresponding numbers in the MICT group (changing to HIIT) were 46 (12%), 54 (14%), and 43 (11%) (supplementary appendix, table S3). Supplementary appendix, tables S3-S5 provide a more detailed description of the activity patterns.
Health related quality of life and safety
After five years, the HIIT group had a significantly higher physical component continuous summary score than the control group (P=0.01) and MICT group (P=0.04). In addition, the mental component continuous summary score was significantly higher in the HIIT group compared with control group (P=0.04) and MICT group (P=0.04) after five years (supplementary table S6).
Three participants (two in MICT group, one in HIIT group) experienced fracture injuries while exercising on a slippery surface during outdoor training. No cardiovascular disease related events occurred during supervised exercise sessions.
Discussion
The Generation 100 study is a long and large randomised controlled trial of exercise in a general population of older adults (70-77 years). This study found no differences in all cause mortality between a combined exercise group (MICT and HIIT) and a group that followed Norwegian guidelines for physical activity (control group). We observed a non-significant 1.7% absolute risk reduction in all cause mortality in the HIIT group compared with control group, and a non-significant 2.9% absolute risk reduction in all cause mortality in the HIIT group compared with MICT group. Furthermore, physical activity levels in the control group were stable throughout the study, with control participants performing more activities as HIIT compared with MICT participants, suggesting a physical activity level in control participants between that of MICT and HIIT.
Strengths and limitations of this study
This study has several limitations. Firstly, participants in the control group had a high level of activity throughout the study, and many exercised using HIIT. This might have affected the study’s ability to detect statistically significant differences between groups. Secondly, only 50% of participants in the HIIT group were able to follow the strict criteria for fulfilling the HIIT protocol. Thirdly, selection bias might have influenced our results, as participants were more active and had better overall health than non-included participants.12 The healthy volunteer bias might have moderated the effects of exercise on the outcomes.19 Fourthly, the null results from this study do not refute a causal association between physical activity and longevity. Since our population was healthier than expected, with 80% reporting a medium or high level of physical activity at baseline, the potential to increase physical activity levels further might have been limited, and this could have led to a ceiling effect for reduced mortality in this population.
Furthermore, although non-significant, the increase in hazard ratio for all cause mortality in the MICT group compared with control group likely contributed to the non-significant overall effect. Combined, our data for all cause mortality indicate that a balance between high and moderate intensity physical activity is beneficial. The optimal combination remains to be determined but it seems like a HIIT dose somewhere between the HIIT in controls and that performed in the HIIT group is required. This is currently speculative, however, and needs to be tested in future studies. Our study was conducted in real life settings; therefore, it was a challenge to accurately track adherence to the exercise intervention. Generally, objective measurements of physical activity, by using accelerometers, are considered more accurate than questionnaires.20 Accelerometers do, however, have major weaknesses, with reduced reliability and validity in real life settings. Furthermore, accelerometers are not suitable for measuring activities such as cycling and swimming, and the accelerometer thresholds for moderate and vigorous intensity activity levels are problematic in older adults.2122 Importantly, in numerous studies523 the present physical activity questions have shown sensitivity to predict current and future cardiovascular health. Thus, in the present study, questionnaires seem to be suitable tools to assess moderate and high intensities of physical activity. A main strength of our study is the large number of well described older adults, with about half women. Another strength is the long intervention and that monitoring can be used throughout the study.
Comparison with other studies
Other studies on the effect of exercise on morbidity and mortality include combined lifestyle interventions24 and populations with diseases2526 and have fewer monitored and relatively short periods of supervised exercise.2627
All cause mortality
No other randomised controlled trials in a general population exist with which to compare our results. However, lack of effect of exercise training on all cause mortality corresponds to findings in the Heart Failure: A Controlled Trial Investigating Outcomes of Exercise Training (HF-ACTION) among patients with chronic heart failure undertaking MICT.25 The absence of significant differences in mortality between the control group and the combined MICT and HIIT group in the present study is likely attributed to the high physical activity level in the controls and the healthy volunteer bias. Also, mortality in the control group was less than half compared with the 10% death rate in the general population of older adults in Norway over the five year study period.28 The participants agreed to take part on the understanding that they could be randomised to the high intensity arm, so this indicated they were compliant about performing exercise. Participants in the control group did not receive supervised exercise yet exercised at relatively high levels throughout the five years, which could be because they knew they would be invited to a regular standardised health check (one, three, and five years). Another potential contamination factor could have been the increased focus on the health benefits of HIIT in the media over the past decade, which might have motivated the control group to perform this form of exercise. It is also easy for people in Trondheim to participate in HIIT, as this type of exercise is offered by different organisations throughout the city (eg, fitness centres, private groups). Although selection bias might play a role, and we cannot fully rule out that the low mortality rate was due to selection, not the intervention, our results indicate that all three interventions had an effect and reduced the risk of premature death.
In line with our study, HF-ACTION observed a high and systematic exercise training pattern in the control group, which probably reduced the study’s ability to detect statistically significant effects of exercise training on primary outcomes. Thus, our study and the other large randomised exercise trial, HF-ACTION, reveal serious challenges about a suitable control group. New concepts or study designs are needed to avoid the Hawthorne effect in future studies.29
Despite no associated effect on all cause mortality in the exercise groups combined, the findings that HIIT was associated with a reduced risk of mortality compared with MICT suggest that performing high intensity physical activity should have a key role in physical activity prevention programmes.
Exercise effects on cardiovascular disease and cancer
Observational studies suggest that exercise plays an important role in preventing cardiovascular disease and cancer,3031 the two major causes of death among older adults. Randomised controlled trials on the effect of exercise and exercise intensity on these outcomes are, however, lacking. One study in patients with heart failure with reduced ejection fraction observed no difference in cardiovascular disease events between HIIT and MICT groups after 52 weeks of follow-up.26 However, only 20% of the HIIT group in that study exercised at the prescribed intensity, making it difficult to draw firm conclusions. Several things could explain the lack of significant findings in our study. The highly active participants in the control group could have hampered finding differences between the exercise group and control group. Also, by pooling different conditions of cardiovascular disease and cancer, we might have missed the possible effect of exercise or exercise intensity, or both on the pathophysiology related to the specific condition. For instance, it has recently been shown that HIIT reduces the burden of atrial fibrillation in people with non-permanent atrial fibrillation,32 whereas it has been shown that strenuous physical exercise can trigger the onset of acute myocardial infarction both in sedentary33 and in highly active34 people. Thus, a more nuanced approach could add additional information in future studies. In the present study we observed that of the 273 individuals with established cardiovascular disease, only two of the 16 deaths were due to cardiovascular disease; the rest were from cancer (n=9) and other causes (n=5). Whereas of the 263 individuals with cancer, 21 died, and all from cancer. These observations might indicate that regular exercise training is more protective against cardiovascular disease related mortality compared with cancer in populations with disease present and warrants future studies.
Peak oxygen uptake
Based on longitudinal3536 and cross sectional studies,37 we expected an age dependent decline in peak oxygen uptake of at least 3.5 mL/kg/min over the five year period. We observed no decline in peak oxygen uptake in any group, showing that both MICT and HIIT as well the recommended physical activity levels (control group) prevented the expected age dependent decline. Observational studies have shown that even a 1 mL/kg/min increase in peak oxygen uptake has been associated with a substantial impact on survival23383940 and incidence of fatal and non-fatal coronary heart disease.41 Thus, although the absolute difference in peak oxygen uptake between the groups was low (0.7 mL/kg/min after five years), higher peak oxygen uptake after HIIT might have contributed to a reduced risk of all cause mortality compared with the other groups.
Adherence and safety
Although high intensity training, which HIIT represents, has now been incorporated in most public health recommendations, the long term effect, feasibility, and safety have recently been questioned.264243 Although HIIT might be challenging to perform, as indicated by lower adherence to the prescribed exercise intensity and slightly higher drop-out rate, our study shows that long term HIIT is feasible and safe for older adults. Compared to other studies,2526 the drop-out rate over the five years study period was low, and the adherence to prescribed exercise was relatively high. In a real life setting, the control group in our study was observed to adhere to the recommendations given at the start of the study period for five years. The fact that the health status of participants in the control group was assessed as often as that in the other two groups is a likely motivational factor for not dropping out. This observation also warrants future studies because a yearly standardised health check-up could encourage adherence to public physical activity recommendations and could be a beneficial socioeconomical and individual tool to reduce healthcare costs and improve the health quality of billions of people worldwide.
Health related quality of life
Observational studies have shown that older adults who are physically active have a higher health related quality of life than those who are less physically active.44 Randomised controlled trials have also shown that moderate intensity aerobic exercise for 12 months can increase health related quality of life compared with controls in initially inactive older adults.45 Our study evaluated the long term effect of different exercise intensities on health related quality of life in older adults. It has been reported that improvements of more than 3.77 in mental health component scores and of more than 3.29 in physical component scores should be considered clinically relevant in people (average age 46 years) with low back pain.46 The clinically meaningful differences in a general population of older adults remain unclear. Nevertheless, our data show that HIIT was better than recommended physical activity guidelines and moderate intensity exercise at maintaining both physical component summary and mental component summary scores in older adults.
Unanswered questions and future research
Our observations indicate that regular exercise training is more protective against cardiovascular disease related mortality than against cancer related mortality in populations with pre-existing disease and this finding warrants further investigation. Furthermore, in 2012, when the current study was initiated, it was not common to use smartphones and eHealth tools to monitor and motivate older adults to become and stay physically active, and so these methods should be included in future studies. Finally, new concepts or study designs are needed to avoid the Hawthorne effect of a suitable control group in future studies.
Policy implications
Most countries have experienced a large demographic change, with a substantial increase in the proportion of older adults alongside an increase in preventable, non-communicable diseases, which now account for more than 60% of all global deaths. Increased life expectancy, if not accompanied by good health, could lead to loss of independence and increased disability and morbidity, resulting in substantially higher healthcare costs and premature mortality. Cardiorespiratory fitness (peak or maximal oxygen uptake) is now regarded as a clinical vital sign,47 and physical activity guidelines have been developed as a non-expensive health promoting strategy in public healthcare to maintain or improve cardiorespiratory fitness, overall wellbeing and to combat the growing burden of non-communicable diseases worldwide. Today’s physical activity recommendations around the world are relatively consistent and advise adults (including older adults) to exercise at moderate intensity for 150 minutes a week or at vigorous intensity for 75 minutes a week. The recommendations also state that they can be reached by combining moderate and vigorous activity provided that a certain total volume of energy expenditure is satisfied (at least 4184 kJ a week). The central implication is that either shorter duration vigorous physical activity or longer duration moderate physical activity or a combination of the two, that amount to the same amount of work each week, will have the same favourable health outcomes, with vigorous physical activity being the time efficient alternative. However, the physical activity guidelines have not been tested in large long term prospective randomised clinical trials, and information about their effect in older adults is lacking. In our study we found larger health benefits in those who undertook mainly high intensity exercise compared with those who undertook mainly moderate intensity exercise. We suggest that future guidelines for physical activity, at least for older adults, should be more specific in requiring that at least part of the physical activity should be performed at high intensity.
Conclusion
Compared with the Norwegian recommended guidelines for physical activity, supervised exercise (HIIT and MICT combined) showed no effect on all cause mortality, cardiovascular disease events, or cancer events in older adults. Our data do, however, suggest that HIIT lowers the risk of premature death compared with recommended guidelines and MICT.
What is already known on this topic
Physical activity has been highlighted as one of the most important actions people of all ages can engage in to improve health
Data from observational studies show that premature mortality is statistically significantly reduced in physically active compared with inactive individuals
High quality evidence on a potential causal relation between current advice on physical activity levels and longevity is lacking from randomised clinical trials
What this study adds
All cause mortality did not differ between the combined high and moderate intensity exercise group and the group following recommended physical activity guidelines
Larger health benefits were found in those who mainly undertook high intensity rather than moderate intensity exercise
The findings suggest that future guidelines for physical activity, at least for older adults, should be more specific in requiring that at least part of the physical activity should be performed at high intensity
Acknowledgments
We thank the participants of the Generation 100 study for their contribution.
Footnotes
Contributors: DS and UW had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analyses. DS, UW, SAA, AS, JPL, JLH, SLS, LJV, OR, HV, ES, JEI, and NZ conceived and designed the study. DS, ART, HV, HD, JPL, TC, SBS, FHB, LSR, and NZ acquired the data. DS, UW, OR, HD, MAFS, JSC, SL, ES, EM, SAA, LJV, JLH, AS, HV, SLS, and JSC analysed and interpreted the data. DS, OR, and UW drafted the manuscript. All authors critically revised the manuscript for intellectual content. DS, OR, and UW supervised the study and obtained funding. UW and DS are the manuscript’s guarantors. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding: This work was supported by the Research Council of Norway; The K.G. Jebsen Foundation for Medical Research, Norway; Norwegian University of Science and Technology (NTNU); Central Norway Regional Health Authority; St Olavs hospital, Trondheim, Norway; and the National Association for Public Health, Norway. The funding organisations had no role in the design and conduct of the study; in the collection, analysis, and interpretation of the data; or in the preparation, review, or approval of the manuscript.
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: support from the Research Council of Norway; The K.G. Jebsen Foundation for Medical Research, Norway; Norwegian University of Science and Technology (NTNU); Central Norway Regional Health Authority; St Olavs hospital, Trondheim, Norway; and the National Association for Public Health, Norway; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Ethical approval: The study was approved by the Regional Committee for Medical Research Ethics (REC South East B; REK 2012/381 B).
Data sharing: We are not permitted to share individual data from the current trial, but we are open to collaborative research with researchers worldwide, who can have access to analysed data from our university. We have also established a biobank of blood and genetic material that we plan to share with researchers worldwide, but individual data must be analysed within our university only.
The lead authors (DS and UW) affirm that this manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
Dissemination to participants and related patient and public communities: We plan to disseminate all the results to study participants and patient organisations as soon as the study is published.
Provenance and peer review: Not commissioned; externally peer reviewed.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.