Infectious diseases in children and adolescents in China: analysis of national surveillance data from 2008 to 2017
BMJ 2020; 369 doi: https://doi.org/10.1136/bmj.m1043 (Published 02 April 2020) Cite this as: BMJ 2020;369:m1043
- Yanhui Dong, doctoral student1,
- Liping Wang, research fellow2,
- David P Burgner, professor3 4,
- Jessica E Miller, postdoctoral researcher3 4,
- Yi Song, associate professor1,
- Xiang Ren, assistant research fellow2,
- Zhongjie Li, research fellow2,
- Yi Xing, associate professor1,
- Jun Ma, professor1,
- Susan M Sawyer, professor3 4 5,
- George C Patton, professor3 4 5
- 1Institute of Child and Adolescent Health, School of Public Health, Peking University; National Health Commission Key Laboratory of Reproductive Health, Haidian District, Beijing 100191, China
- 2Division of Infectious Disease Control and Prevention, Key Laboratory of Surveillance and Early Warning on Infectious Disease, Chinese Centre for Disease Control and Prevention, Beijing, China
- 3Murdoch Children’s Research Institute, Parkville, Victoria, Australia
- 4Department of Paediatrics, the University of Melbourne, Parkville, Victoria, Australia
- 5Centre for Adolescent Health, Royal Children’s Hospital, Parkville, Victoria, Australia
- Correspondence to: J Ma majunt{at}bjmu.edu.cn
- Accepted 12 March 2020
Abstract
Objectives To outline which infectious diseases in the pre-covid-19 era persist in children and adolescents in China and to describe recent trends and variations by age, sex, season, and province.
Design National surveillance studies, 2008-17.
Setting 31 provinces in mainland China.
Participants 4 959 790 Chinese students aged 6 to 22 years with a diagnosis of any of 44 notifiable infectious diseases. The diseases were categorised into seven groups: quarantinable; vaccine preventable; gastrointestinal and enteroviral; vectorborne; zoonotic; bacterial; and sexually transmitted and bloodborne.
Main outcome measures Diagnosis of, and deaths from, 44 notifiable infectious diseases.
Results From 2008 to 2017, 44 notifiable infectious diseases were diagnosed in 4 959 790 participants (3 045 905 males, 1 913 885 females) and there were 2532 deaths (1663 males, 869 females). The leading causes of death among infectious diseases shifted from rabies and tuberculosis to HIV/AIDS, particularly in males. Mortality from infectious diseases decreased steadily from 0.21 per 100 000 population in 2008 to 0.07 per 100 000 in 2017. Quarantinable conditions with high mortality have effectively disappeared. The incidence of notifiable infectious diseases in children and adolescents decreased from 280 per 100 000 in 2008 to 162 per 100 000 in 2015, but rose again to 242 per 100 000 in 2017, largely related to mumps and seasonal influenza. Excluding mumps and influenza, the incidence of vaccine preventable diseases fell from 96 per 100 000 in 2008 to 7 per 100 000 in 2017. The incidence of gastrointestinal and enterovirus diseases remained constant, but typhoid, paratyphoid, and dysentery continued to decline. Vectorborne diseases all declined, with a particularly noticeable reduction in malaria. Zoonotic infections remained at low incidence, but there were still unpredictable outbreaks, such as pandemic A/H1N1 2009 influenza. Tuberculosis remained the most common bacterial infection, although cases of scarlet fever doubled between 2008 and 2017. Sexually transmitted diseases and bloodborne infections increased significantly, particularly from 2011 to 2017, among which HIV/AIDS increased fivefold, particularly in males. Difference was noticeable between regions, with children and adolescents in western China continuing to carry a disproportionate burden from infectious diseases.
Conclusions China’s success in infectious disease control in the pre-covid-19 era was notable, with deaths due to infectious diseases in children and adolescents aged 6-22 years becoming rare. Many challenges remain around reducing regional inequalities, scaling-up of vaccination, prevention of further escalation of HIV/AIDS, renewed efforts for persisting diseases, and undertaking early and effective response to highly transmissible seasonal and unpredictable diseases such as that caused by the novel SARS-CoV-2 virus.
Introduction
China has undergone a rapid epidemiological transition, with major reductions in infectious diseases contributing to an increasing life expectancy from 35 years at birth in 1949 to 76.7 years in 2017.12 The country successfully eliminated 11 infectious diseases, including smallpox, in the early 1960s, and a further 10 more recently, including poliomyelitis.3 An additional 13 diseases, including measles, seem now to be at low endemic levels,4 and the goal of a national malaria elimination programme that was launched in 2010 is nationwide elimination by 2020.5 China’s success has greatly contributed to worldwide reductions in infectious diseases.67
In the context of rapid reductions in many infectious diseases, questions remain about whether current priorities deal with contemporary needs. The epidemics of severe acute respiratory syndrome (SARS) in 2003 and the sudden emergence of the new coronavirus disease in 2019(covid-19), highlight new threats and the need for effective surveillance.891011 Further global outbreaks over the past decade, including H1N1, H5N1, and H7N9 influenza, Zika virus, yellow fever, chikungunya, dengue, and Ebola, reinforce this need.1213141516 After the SARS outbreak in 2003, China overhauled its national China Information System for Disease Control and Prevention (CISDCP), the world’s largest internet based notifiable disease reporting system, introducing web based reporting in real time.1 This was accompanied by a major national infectious disease control initiative, with a particular focus on expanded immunisation.17
Children and adolescents in China have benefited greatly from overall reductions in infectious diseases during the past several decades, but rapid demographic, epidemiological, and nutritional transitions have brought a pressing need to track infectious diseases in children and adolescents.1618 Children and adolescents remain the most susceptible age group to most infectious diseases, which makes them a priority for Chinese public health policy. Yet there has been no systematic study of the changing patterns of infectious diseases in China. With the objective of highlighting public health policy priorities, we analysed recent trends across time and by age, sex, season, and province for 44 notifiable infectious diseases in children and adolescents using web based surveillance CISDCP data from 2008 to 2017.
Methods
Data collection
Data were drawn from CISDCP. After the SARS outbreak in 2003, China updated and established the web based CISDCP to rapidly identify new cases and respond to outbreaks. Since 2008 all case based data on notifiable infectious diseases are transmitted electronically to the China Centre for Disease Control (CDC) through direct online reporting. The system covers national notifiable infectious diseases for all 31 provinces in mainland China. We analysed data for the decade from 2008 to 2017. All types of health facilities in China are covered in the CISDCP, including hospitals, Centers for Disease Control (CDCs) at each level, community health centres, township health centres, and village clinics. Supplementary figures S1 and S2 present the national coverage rates of CISDCP network reporting and its geographical variations by year from 2008 to 2017 for township level and for county level and above. The national average coverage rates of CISDCP remained stable during this decade, ranging from 85.1% to 95.4%. In 2017, web based reporting covered 87.2% national health facilities. The national coverage rates for health facilities at county level and above were higher than that at the township level (ie, in 2017, county level and above was 95.8% and township level was 85.5%). Coverage was also higher in the eastern regions than in the western regions in each year (ie, in 2017, coverage in the eastern region was 95.1%, central region was 94.5%, and western region was 81.6%).
Classification
A total of 44 notifiable infectious diseases were included in this study. We adapted and revised Zhang and Wilson’s 2012 classification of 44 CISDCP notifiable infectious diseases into seven major categories reflecting disease causes, characteristics, and policy responses.3 The main revisions were the inclusion of hepatitis A, B, and D as vaccine preventable diseases. Hepatitis C was classified within an extended category of sexually transmitted diseases and bloodborne infections and hepatitis E similarly for zoonotic infections. The revised categories were quarantinable; vaccine preventable; gastrointestinal and enteroviral; vectorborne; zoonotic; bacterial; and sexually transmitted and bloodborne (see table 1). Medical staff confirmed all patients with a clinical diagnosis by clinical standards and laboratory tests based on national uniform standards (see supplementary appendix). Since 2014, H1N1 has been included in the seasonal influenza category.19 Case information recorded in CISDCP included time and place of onset and death, diagnosed disease, age, sex, and occupation. Case identification information (eg, name, address) is not recorded to ensure confidentiality of data.
Changes in number of cases, number of deaths, incidence (per 100 000), and mortality (per 100 000) for 44 notifiable infectious diseases in China, 2008-17
Inclusion and exclusion criteria
Children and adolescents were included in the analysis if they were a student aged 6 to 22 years with verified records of any of the 44 notifiable infectious diseases, from 31 provinces in mainland China. According to Chinese law, “the free nine-year compulsory education system” law, introduced in 2006,20 school enrolment is mandatory for children from age 6 years—that is, parents or other legal guardians must send the children to school during these years. Under the education system in China, most 22 year olds have completed undergraduate education. People were excluded from our analysis if they met any of the following conditions1: were resident in Hong Kong, Macao, Taiwan of China, or other countries2; had occupations other than student in primary school to university3; were suspected of having one of the notifiable diseases and were pathogen carriers4; and had a recorded repeat diagnosis, misdiagnosis, and other unverified records (see flowchart in supplementary figure S3).
Estimates of indicators and population
We calculated incidence (per 100 000) as the number of annual incident cases divided by the population size, and overall mortality (per 100 000) as the number of annual deaths divided by the population size. Population size was estimated from the sum of national and provincial populations of students of each year, age, and sex from 2008 to 2017 using data from the Ministry of Education.21
Statistical analysis
Descriptive analyses were used to present trends in incidence and number of cases of, and deaths from, 44 notifiable infectious diseases from 2008 to 2017. Incidence and mortality were the core indicators. Pie graphs were used to analyse the trends and the characteristics of distribution of each infectious disease for incidence, number of cases, and deaths. Stacked plots were used to analyse the trends in proportions of all the infectious diseases by categories. We compared the ranks and proportions of each notifiable infectious disease for incidence, number of cases, and deaths in each year and changes over the study period. Age and province specific disease in each survey year and the seasonal variation of each disease by month were also analysed. To identify the features of major infectious diseases we extracted the top infectious disease for each age and province. We compared the characteristics of trends from 2008 to 2017 in the leading infectious diseases by age from 6 to 22 years. The χ2 test was used to compare the incidence by sex and inter-regional differences in disease categories.
Joinpoint regression models22 were used to examine trends in incidence for each infectious disease from 2008 to 2017 and to estimate annual percentage changes (APCs). The same models were used to test the differences across regions and sex-age subgroups. Joinpoint regression analysis identifies time points in which trends significantly change (ie, joinpoints), using calendar year as the timescale.2324 To determine the location of the joinpoints, we used the grid search method. This creates a grid of all possible locations for joinpoints at each survey year and tests the sum of squared errors for each point to find the best fit.2225 Joinpoint regression assumes normal distribution of disease incidence. If this assumption does not hold, data transformation is recommended. In our data, some infectious diseases had Poisson distributions and required a logarithmic transformation to approximate a normal distribution. The resulting log-linear models were easier to interpret in the joinpoint regression analysis. Under a log-linear model, rates change at a constant percentage each year, calculated in our study as a fixed APC, whereas in a linear model, the rates change at a constant amount each year. When comparing trends in different categories or for specific infectious diseases or across provinces, the rates are different. The advantage of a log-linear model is that the APC can be compared across widely different scales. For example, rare and common infectious diseases might change at the same annual percentage each year, but it is unlikely that they would change at the same fixed amount each year. With this approach, infectious diseases were assumed to change at a constant percentage of the rate of the previous year. For example, if the APC was 1% and the rate was 50 per 100 000 in 2007, then in 2008 the rate was 50×1.01=50.5, and in 2009 the rate was 50.5×1.01=51.005. Rates that change at a constant percentage every year change linearly on a log scale. The P value for a two sided test that the true APC is zero was calculated based on a t distribution. If the APC was non-significant (P≥0.05), we regarded trends as stable, otherwise, it increased or decreased for each infectious disease from 2008 to 2017.
Descriptive analyses were performed using Stata V.15 software (College Station, TX). The joinpoint regression analyses were carried out using the joinpoint regression program version 4.7.0.0 provided by the surveillance, epidemiology, and end results programme (National Cancer Institute; https://surveillance.cancer.gov/joinpoint/).26
Patient and public involvement
The outcome was the diagnosed disease for each participant recorded in the system, including the time and place of onset and death, age, sex, and occupation. This research used personal health information that is not accessible to patients or the public. No members of the public were directly involved in the study design, outcome measures, analysis of data, or interpretation of study results.
Results
Overall trends in infectious diseases
From 2008 to 2017, 44 notifiable infectious diseases were diagnosed in 4 959 790 children and adolescents (3 045 905 males, 1 913 885 females) aged 6-22 years in China (see supplementary figure S3). The joinpoint regression models identified that 2015 was the turning point in the trend across 2008-17, generating two different linear trends in the overall incidence (fig 1). The total incidence of notifiable infectious diseases decreased significantly, from 279.7 per 100 000 population in 2008 to 161.6 per 100 000 in 2015, with an APC reduction of −8.1% (95% confidence interval −12.5% to −3.6%, P=0.007) of all infectious diseases, which then increased to 241.9 per 100 000 in 2017, with a relative APC of 16.7% (−21.1% to 72.7%, P=0.36). The overall mortality from the 44 notifiable infectious diseases decreased steadily, from 0.21 per 100 000 in 2008 to 0.07 per 100 000 in 2017, an overall relative reduction in mortality of 66.7% during the 10 years, and with a significant APC of −11.7% (−14.3% to −9.1%, P<0.001; see supplementary table S1). The total number of deaths from infectious diseases similarly decreased, from 467 per 100 000 in 2008 to 146 per 100 000 in 2017, an overall relative reduction of 68.7% (see supplementary table S2). Of the seven categories, vaccine preventable diseases, gastrointestinal and enterovirus diseases, and bacterial infections accounted for most of the notifiable infectious diseases (fig 2).

Trends in incidence of and mortality from 44 notifiable infectious diseases and joinpoints, 2008-17. *Statistically significant trends. APC=annual percentage change
{kind=link}

Trends in incidence and proportions of 44 notifiable infectious diseases by categories, 2008-17. Top panels are based on seven categories of infectious diseases. Bottom panels are based on all 44 current notifiable infectious diseases. TB=tuberculosis; ID=infectious diarrhoea diseases; HFMD=hand, foot, and mouth disease; SI=seasonal influenza; SF=scarlet fever; AHC=acute haemorrhagic conjunctivitis; T/P=typhoid and paratyphoid; JE=Japanese encephalitis; HF=haemorrhagic fever; MM=meningococcal meningitis; HD=hydatid diseases; H5N=avian influenza H5N1; H7N9=avian influenza H7N9; H1N1=influenza A H1N1; SARS=severe acute respiratory syndrome
{kind=link}
Trends by infectious disease category
Table 1 and figure 3 show 10 year trends in incidence of, and deaths from, each notifiable infectious disease by disease category, as well as the relative ranking (see fig 4 and supplementary figures S4-S6). Overall, three categories—vaccine preventable diseases, gastrointestinal and enterovirus diseases, and bacterial infections—still had high endemic levels. Among the other four categories with relatively low levels, sexually transmitted diseases and bloodborne infections increased noticeably.
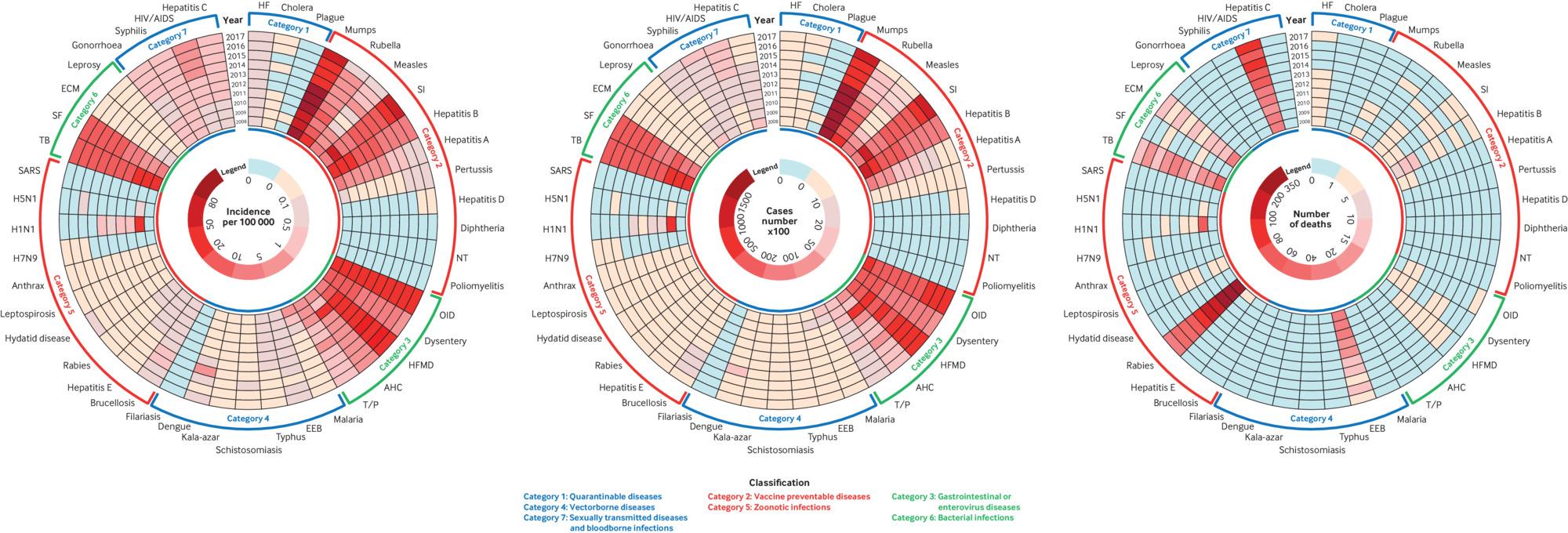
10 year trends in (a) incidence, (b) number of cases, and (c) number of deaths for 44 notifiable infectious diseases, arranged by seven categories, by year from 2008 to 2017. Each concentric circle represents one year starting from 2008 in the centre to 2017, and each vertical row represents one infectious disease. Different colours represent the extent of incidence, number of cases, and number of deaths. Pale blue boxes represent zero for each infectious disease
{kind=link}

Ranking of incidence of each of the 44 notifiable infectious diseases by year, from 2008 to 2017. Annual percentage change (APC) in incidence of each infectious disease is listed with 95% confidence intervals. In the APC column, arrows pointing upwards (red) represent overall increased trends, arrows pointing downwards (green) represent decreased trends, whereas arrows pointing to the right (purple) represent stable trends for incidence of each infectious disease from 2008 to 2017
{kind=link}
Quarantinable diseases—among the three quarantinable diseases, cholera and plague had virtually disappeared. Haemorrhagic fever maintained a low but stable incidence (P=0.68).
Vaccine preventable diseases—the incidence of most vaccine preventable diseases decreased to low levels over the study period, particularly for rubella, measles, hepatitis A, and hepatitis B. For example, rubella dropped from third ranking to 17th and measles from eighth to 18th, and measles showed a 62.4% annual average decline from 2008 to 2011 (P=0.004 from 2008 to 2011), remaining low (P=0.61 from 2011 to 2017). The incidence of hepatitis A decreased from 6.1 to 0.4 per 100 000 and hepatitis B from 47.4 to 5.81 per 100 000, with 26.0% and 21.9% annual average declines, respectively (P<0.001). Pertussis incidence remained at a low level, and one joinpoint was identified in 2012. The incidence of pertussis decreased noticeably, with −21.5% APC (P=0.02) before 2012, but increased sharply from 2012 to 2017 with 36.1% APC (P<0.001). The incidence of mumps and seasonal influenza remained high, making these the most common vaccine preventable diseases in 2017. The relative increase of mumps and seasonal influenza accounted for 79.8% of the overall rebound between 2015 and 2017, especially for seasonal influenza, which showed 77.2% annual average increases across these two years (P=0.04). During 10 years, the incidence of seasonal influenza increased nearly 10-fold, from 6.3 per 100 000 in 2008 to 58.3 per 100 000 in 2017, an average annual 31.7% relative increase (P<0.001). No cases of diphtheria, neonatal tetanus, and poliomyelitis were recorded, and the mortality from vaccine preventable diseases was low.
Gastrointestinal and enterovirus diseases—a steady decline occurred in gastrointestinal and enterovirus diseases, including dysentery, acute haemorrhagic conjunctivitis, and typhoid and paratyphoid, with annual average declines of 13.4% (P<0.001), 33.9% (P=0.06), and 10.1% (P=0.001), respectively. However, noticeable relative increases occurred in incident cases of hand, foot, and mouth disease and infectious diarrhoea. The incidence of hand, foot, and mouth disease increased from 9.4 to 29.5 per 100 000, with an 8.6% annual average relative increase (P=0.04). A stable trend for infectious diarrhoea was observed from 2008 to 2014 (P=0.88), but a significant increase in incidence was found over the following four years, from 22.2 per 100 000 in 2014 to 34.0 per 100 000 in 2017 (APC=14.5%, P=0.03).
Vectorborne diseases—vectorborne diseases generally declined, with a particularly noticeable relative reduction in malaria, from 1.4 per 100 000 in 2008 to 0.012 per 100 000 in 2017 (APC=−40.6%, P=0.003, with a fall in ranking from 13th to 28th across the 10 year period). Sharp declines occurred across the first six years (APC=−63.4%, P<0.001), remaining stable until 2017 (P=0.83). The incidence of Japanese encephalitis, typhus, and Kala-azar steadily declined from 2008 to 2017 (APC=13.7%, P=0.001; 13.1%, P<0.001; and 16.0%, P<0.001, respectively). Among all the vectorborne diseases, Japanese encephalitis had the highest mortality, but it also showed a steady decline. Excluding the influence of a small outbreak in 2015, the incidence of schistosomiasis steadily declined across the 10 years (APC=−32.1%, P<0.001). The incidence of dengue increased from 0.009 per 100 000 in 2008 to 0.19 per 100 000 in 2017, a 20-fold relative increase across the decade, despite a small outbreak in 2014, with an incidence of 1.6 per 100 000.
Zoonotic infections—the incidence of all zoonotic infections was low. Rabies remained the second most common infectious cause of death overall, despite a decline in incidence of around 90% and annual average declines of 20.0% over the past decade (P<0.001). Steady declines were observed in hepatitis E and leptospirosis (P=0.001 and P<0.001, respectively), but brucellosis showed a significant increase, with annual average changes of 7.5% from 2008 to 2017 (P=0.04). Hydatid disease and anthrax maintained stable trends across the decade (P=0.33 and P=0.25, respectively), although a joinpoint year was identified in 2014 for hydatid disease in males, after which its incidence increased noticeably to 2017 (APC=38.1%, P=0.05). Hydatid disease remained stable in females. Similarly, a joinpoint year was identified in 2011 for anthrax, with a significant reduction from 2008 to 2011 (APC=−33.4%, P=0.05), followed by a stable trend to 2017 (P=0.27). An outbreak of H1N1 occurred in 2009, and an occasional emergence of other avian influenza across the decade, including H7N9 and H5N1.
Bacterial infections—overall, 2010 was identified as a turning point in trend for bacterial infections. The total incidence of bacterial infections decreased from 34.7 per 100 000 in 2008 to 24.6 per 100 000 in 2010 (APC=−14.3%, P=0.29), but then increased to 31.3 per 100 000 in 2017 (relative APC=2.1%, P=0.31, 2010-17). Significant declines were shown for tuberculosis, from 28.9 to 18.9 per 100 000, and for meningococcal meningitis, from 0.2 to 0.03 per 100 000, with relative APC reductions of 5.1% and 20.5%, respectively (P<0.001). Although the incidence of leprosy also showed a large decline, from 0.017 to 0.008 per 100 000, the APC of 7.3% was statistically insignificant. In contrast, the incidence of scarlet fever more than doubled, increasing from 5.6 to 12.4 per 100 000 across the 10 years, which increased its ranking from 11th in 2008 to sixth in 2017 (APC=10.1%, P=0.02).
Sexually transmitted diseases and bloodborne infections—2011 was identified as the turning point in trend for sexually transmitted disease and bloodborne infections over the decade. Total incidence decreased from 2.8 per 100 000 in 2008 to 2.3 per 100 000 in 2011 (APC=−5.4%, P=0.19), but then increased relatively to 3.7 per 100 000 in 2017, with a relative APC of 7.3% (P=0.002, 2011-17). Among four sexually transmitted diseases and bloodborne infections, the incidence of hepatitis C declined by about 63% over the study period, from 0.89 per 100 000 in 2008 to 0.33 per 100 000 in 2017 (APC=−11.8%, P<0.001). Cases of HIV/AIDS increased fivefold, from 0.27 per 100 000 in 2008 to 1.49 per 100 000 in 2017, with a large significant APC increase during the study period (APC=21.9%, P<0.001). HIV/AIDS incidence increased rapidly between 2008 and 2015 (APC=29.2%, P<0.001), with stable incidence reported from 2015 to 2017 (P=0.94). HIV/AIDS is now the major cause of death from infectious diseases in children and adolescents, having surpassed rabies in 2014. The incidence of syphilis steadily increased from 0.65 per 100 000 in 2008 to 0.99 per 100 000 in 2017, with a significant relative APC of 3.8% (P=0.004). Although the incidence of gonorrhoea was stable across the study period, one joinpoint was identified in 2012, with a large annual average decline of 22.4% from 2008 to 2012 (P=0.002). This was followed by a significant increase in the relative APC to 2017 (18.9%, P=0.004), with the incidence in 2017 (0.93 per 100 000) returning to 2008 levels (0.96 per 100 000).
Variation by age, sex, and season
Incidence of infectious diseases differed by age (fig 5). For quarantinable diseases, haemorrhagic fever was the leading disease in each age group in each year. Among 11 vaccine preventable diseases, mumps dominated in children aged less than 13 years in 2017, but was surpassed by hepatitis B and seasonal influenza in those older than 13 years. Within gastrointestinal and enterovirus diseases, the leading disease was hand, foot, and mouth disease in children aged less than 11 years, but infectious diarrhoea was the most common infection in those older than 12 years. For vectorborne diseases, Japanese encephalitis was the leading diagnosis in children aged less than 10 years. Before 2011, malaria was most common in those older than 11 years, whereas dengue became most common from 2011 onwards. For zoonotic infections, brucellosis was the most common infection in each age group, apart from an outbreak of influenza A H1N1 from 2009 to 2013. For bacterial infections, scarlet fever predominated in children aged 6 to 11 years, whereas tuberculosis was the leading disease in adolescents older than 11 years. Sexually transmitted diseases and bloodborne infections, gonorrhoea, syphilis, and hepatitis C were the most common diseases in all ages, whereas HIV/AIDS increased from 2011, particularly in those older than 18 years.

Infectious diseases with greatest incidence and mortality by age, 2008-17
{kind=link}
A noticeable association was observed between age and some infectious diseases. The most common infections in early childhood included vaccine preventable diseases and gastrointestinal and enterovirus diseases. Those that largely affected older adolescents included sexually transmitted diseases and bloodborne infections, whereas other infections such as zoonoses had a U-shaped age distribution. In terms of sex differences, one of the noticeable features of almost all the infections, except for pertussis, Kala-azar, and dengue in a particular year, was that many more cases and a higher incidence was observed in males than females during the 10 years (P<0.05), particularly for gonorrhoea, HIV/AIDS, and hepatitis C among those older than 14 years (see supplementary figs S7 and S8).
Seasonal variation was observed in most infectious diseases in 2017 (see supplementary fig S9). Among the quarantinable diseases, the incidence of haemorrhagic fever peaked in winter. Similarly, among the vaccine preventable diseases, consistent peaks occurred in winter (December) for seasonal influenza, whereas the incidence of rubella and measles peaked in spring (March). Almost all the gastrointestinal and enterovirus diseases, most vectorborne diseases, and zoonotic infections, as well as hepatitis C in sexually transmitted diseases and bloodborne infections had consistent peaks in summer and leading into autumn.
Regional variations
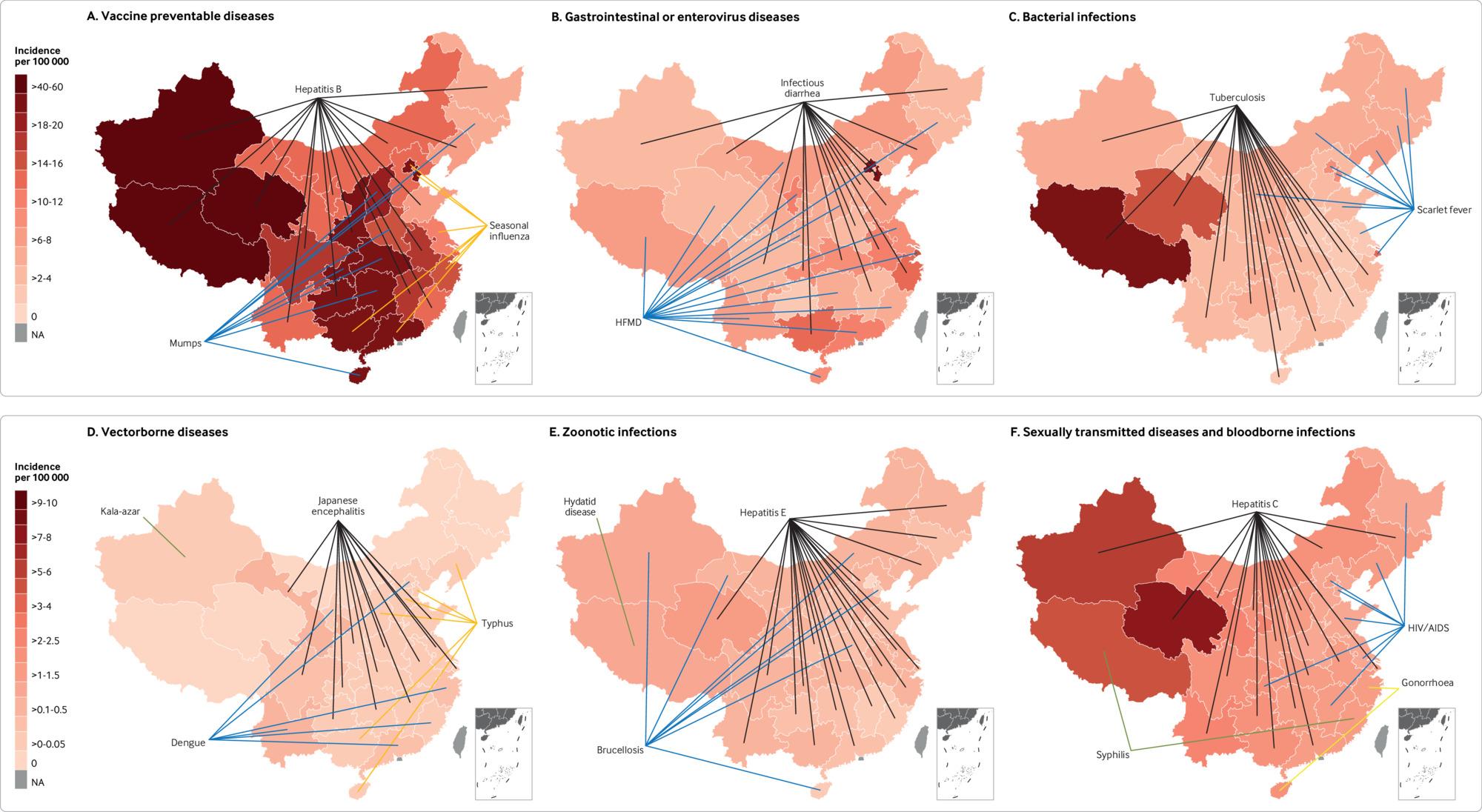
In 2017, distinct region specific patterns were observed in incidence of the infectious diseases (fig 6 and supplementary fig S10). Among the vaccine preventable diseases, hepatitis B was the most common disease in 16 provinces located in the western and eastern regions of China—for example, Qinghai, Tibet, and Xinjiang had the highest incidence. Seasonal influenza was mostly prevalent in the eastern regions, such as Beijing and Tianjin. Mumps was the most common disease in the central regions, such as Hunan and Hubei province. Gastrointestinal and enterovirus disease was common throughout the country, particularly infectious diarrhoea and hand, foot, and mouth disease. Beijing and Tianjin had the highest incidence of infectious diarrhoea. Vectorborne diseases were relatively rare but still predominant in western China. Japanese encephalitis remained the leading vectorborne disease in most provinces, followed by typhus and dengue. For the zoonotic infections, western China was also a high incidence area. Hepatitis E and brucellosis were dominant in most provinces, whereas hydatid disease was only endemic in Tibet. For bacterial infections, although scarlet fever was highly prevalent in some provinces in the eastern regions, such as Beijing, Tianjin, and Shanghai, tuberculosis remained the leading bacterial disease in most provinces, particularly Tibet and Qinghai. Among sexually transmitted diseases and bloodborne infections, hepatitis C predominated in most provinces, with the highest incidence in Qinghai and Xinjiang. HIV/AIDS was the most common sexually transmitted disease and bloodborne infection in some eastern provinces, such as Chongqing and Beijing. Syphilis dominated in Tibet and Fujian, whereas gonorrhoea was highest in Zhejiang and Hainan. Overall, China’s western regions had a disproportionate and continuing burden from many categories of infectious diseases. For example, compared with eastern regions, several western provinces, such as Qinghai, Tibet, and Xinjiang, had a higher incidence of vaccine preventable diseases, sexually transmitted diseases and bloodborne infections, bacterial infections, and zoonotic infections.

Subnational distribution of 44 notifiable infectious diseases in 2017, according to seven categories but excluding quarantinable diseases. The keys vary owing to large difference in incidence of 44 notifiable infectious diseases by category. Quarantinable diseases are not presented because haemorrhagic fever dominated all the provinces without regional variations. Lines indicate the leading infectious disease in each province
{kind=link}
Discussion
From 2008 to 2017 China has had remarkable progress in infectious disease control in children and adolescents aged 6-22 years. Mortality from infectious diseases decreased sharply, and HIV/AIDS has replaced rabies and tuberculosis as the leading cause of death, particularly among adolescent boys older than about 14 years. The incidence of most vaccine preventable diseases is now at low levels, but seasonal variation in mumps, rubella, measles, and influenza suggests these diseases should remain a priority for public policy. Quarantinable diseases with high mortality have effectively disappeared, and vectorborne diseases have declined. The increase in incidence of HIV/AIDS together with gonorrhoea and syphilis suggests that sexually transmitted diseases have become a priority. Although typhoid, paratyphoid, and dysentery continued to decline, the incidence of other gastrointestinal and enterovirus diseases remained constant. Tuberculosis continued to be the most common bacterial infection, and cases of scarlet fever doubled during the past decade. Noticeable regional variation in trends in infectious diseases was observed, with western China generally carrying a disproportionate burden.
Of the vaccine preventable diseases, hepatitis B, mumps, and seasonal influenza remained prominent.27 Although the incidence of hepatitis B declined from 2008 to 2017, it remained the leading reportable infection in children and adolescents in most provinces. China’s childhood hepatitis vaccination programme and improved sanitation have contributed to the decrease in incidence of hepatitis A and B, contrasting with an increasing incidence in Chinese adults.28 Both hepatitis A and B vaccines were included in the national immunisation programme (in 2008 and 2001, respectively) and a vaccine against hepatitis E virus is now licensed in China.29 The implementation of mumps into the expanded programme for immunisation in mainland China in 2008 would have contributed to its decreasing incidence,30 but in the past two years its incidence has increased so that it is now the most common infection in children and adolescents aged 10-22 years. The reasons for this rebound remain unclear but raise questions around vaccine coverage, notwithstanding that other vaccine preventable diseases such as measles, rubella, pertussis, diphtheria, poliomyelitis, and neonatal tetanus have shown continuing declines. The number of rabies cases has also declined, reflecting comprehensive preventive measures, including vaccination of dogs and post-exposure prophylaxis.31
Tuberculosis and scarlet fever were the most common bacterial infections. Tuberculosis is the 11th leading cause of death worldwide and was the leading cause of death from infectious disease in Chinese children and adolescents in 2017.32 Globally, the incidence of tuberculosis has declined, with a 19% fall between 2000 and 2016.33 While the incidence of tuberculosis among Chinese children and adolescents aged 6-22 years decreased, with an annual average decline of 5.1% from 2008 to 2017, its overall ranking remained unchanged. Incidence was higher in children and adolescents aged between 12 and 22 years compared with younger children aged between 6 and 11 years, consistent with previously documented age trends.34 China’s scaling-up of its national tuberculosis control programme to cover half the population during the 1990s and the entire population from 2000 seems likely to have contributed to this decline.35 Multidrug resistant tuberculosis is emerging as a challenge in tuberculosis control in China.36 In 2017, around 3.5% of new cases of tuberculosis in both children and adults were multidrug resistant, with an 18% prevalence of multidrug resistant tuberculosis among those previously treated.3637
An increase in the incidence of scarlet fever has also been observed in other countries recently.383940 The marked increase in Chinese children and adolescents since 2011 coincides with its resurgence in England38 and South Korea.39 This re-emergence of scarlet fever has led to the adoption of symptom surveillance and early warning systems, followed if necessary by enforced absenteeism from school. Similar measures have also been recommended for childhood gastrointestinal and enterovirus diseases (infectious diarrhoea; dysentery; hand, foot, and mouth disease; typhoid and paratyphoid; and acute haemorrhagic conjunctivitis),40 but the effectiveness of these interventions is unknown. Scarlet fever had the highest incidence of any infectious disease in the eastern and northern regions and in 6 to 11 year olds, but tuberculosis dominated the rest of China and in those aged 12 to 22 years. Such variation suggests a need for age and region specific control measures.
The incidence and number of cases of HIV/AIDS in Chinese adolescent males aged from 14 to 22 years have rapidly increased from 2008 to 2017, with HIV/AIDS now the leading notifiable infectious cause of death in Chinese children and adolescents, particularly males. The increasing incidence of HIV seems to be related to high risk sexual behaviours and poor awareness of HIV/AIDS prevention.41 By the end of 2018, 149 000 people with newly diagnosed HIV/AIDS had been reported, 95% of which were sexually transmitted. Of these, 16 000 new HIV/AIDS cases were reported among 15-24 year olds. College and university students accounted for more than 3000 cases, with more than 80% in men who had sex with men.42 China’s latest national survey shows that by 2019 the transmission of HIV through blood transfusion effectively no longer occurred, and transmission through intravenous drug misuse and mother-to-child transmission had been curbed. Globally, one sixth of AIDS related deaths and one seventh of new HIV infections are in children younger than 15 years, with 90% caused by mother-to-child transmission.43 A meta-analysis of 57 studies that covered all provinces in China showed that the rate of mother-to-child transmission in China was 4.4% (95% confidence interval 3.2% to 5.5%), substantially higher than in the US and Europe (<1%), but lower than in some low and middle income countries in sub-Saharan Africa (11%).44
Sexual transmission, notably in men who have sex with men, has become the main transmission route, especially among college students.4245 There have been a range of other contributing factors, including a lack of access to appropriate sex education in secondary schools, a heteronormative approach to the content of sex education, a permissive attitude towards casual sex in university students, and ready access to sex, facilitated by social media.41 In 2015, the Chinese government introduced initiatives targeting HIV in adolescents and young adults age from 15 to 49 years,46 with the health and education ministries jointly establishing an epidemic notification system tied with stronger school based HIV prevention and control measures47; strategies that coincide with a decrease in incidence. However, the global campaign for comprehensive sex education launched by UNESCO in 2018 should be promoted further in China to provide children and adolescents with an evidence based understanding of their sexual and reproductive health, and with the skills to talk with their peers, families, and communities about safe and consensual sexual relationships.48 There is also a pressing need for other school and university based interventions, including network peer education, psychological counselling and education, and access to rapid testing for sexually transmitted infections.49 In addition to the lower incidence of sexually transmitted diseases and bloodborne infections in young children, the major causes of such diseases are likely to differ.
Achievements and challenges
Overall, China has made great advances in the prevention and control of infectious diseases in children and adolescents. After the SARS outbreak in 2003, a substantial investment was made in capacity building for laboratory testing, surveillance system enhancement, national intervention programmes for specific diseases, and collaboration with international partners.115 The major Special National Science And Technology Project On Preventing And Controlling Infectious Diseases that began in 2008 has received a total investment of about $2.25bn (£1.77bn; €2.00bn).50 This project has led to expanded and enhanced screening for infectious diseases, reductions in treatment costs, and increased access to treatment. Furthermore, the national immunisation programme for children in China was expanded in 2008, which is thought to have contributed to the marked reduction in the overall number of cases of vaccine preventable diseases found in the current study.5152
Beyond immunisation programmes, multisectoral collaboration also underpins efforts to control infectious diseases. In China, some parasitic diseases (eg, schistosomiasis) have reached or are approaching elimination status; the result of collaboration between the departments of health, agriculture, and the environment.53 Our findings are consistent with filariasis being eliminated during the study period, as certified by the World Health Organization in 2007.15 Schistosomiasis in adolescents in China is also close to elimination, and malaria has steadily declined from 3221 cases in 2008 to only 25 cases in 2017, consistent with the goal of nationwide elimination by 2020.54
China still, however, faces challenges in responding to infectious diseases in children and adolescents. Firstly, rapid urbanisation and industrialisation and changing patterns of interactions between people and pathogens have altered the pattern of infectious diseases,15 a feature of the covid-2019 outbreak. Geographical disparities raise questions around access to healthcare, other medical and educational resources, public health programmes, and infrastructure in rural and remote areas. Not surprisingly, the western regions of China with poor resources and a special geographical environment and culture face a burden from multiple infectious diseases, with Qinghai, Tibet, and Xinjiang having higher incidence of vaccine preventable diseases, bacterial infections, and sexually transmitted diseases and bloodborne infections. However, the epidemiological characteristics of infectious diseases are also affected by densely populated urban regions,55 which might contribute to higher rates of sexually transmitted diseases and viral gastrointestinal infections, at least in Beijing, Tianjin, and Shanghai. Different factors apply in rural and remote areas, where livestock based lifestyles increase the risk of zoonotic infections and where climate might be an additional factor, particularly for vectorborne diseases. Seasonal variation in infectious diseases, with the example of peaks of influenza and rubella, measles, and scarlet fever in winter and spring suggests the high vulnerability of Chinese children to infections transmitted by aerosol droplets. Furthermore, the rapid increase in HIV/AIDS, especially in adolescent males, requires a much wider set of social and educational responses than for less sensitive behaviours and stigmatised diseases. The resurgence of some diseases that were previously under control (eg, scarlet fever, mumps, syphilis, and brucellosis) and imported cases (eg, Zika virus infection, Rift Valley fever, yellow fever, and Ebola) have put greater pressure on the public health system, as has been seen with the current covid-2019 outbreak that began in Hubei province, China. Although in most cases of covid-19, mortality appears to be higher in older people,10 although the immediate impact of this on children and adolescents is nonetheless immense. A global pandemic of covid-19 could bring about multiple impacts, such as economic recession, food crisis, price fluctuations, constraints on resources, which will have immediate or indirect negative effects on children in the near or long term. In addition, the exact impact has not yet been determined in further studies, but there could be physical and psychological effects on children who have been deprived of concentrated effort of care as a result of the guardian’s illness, which need further studies post-covid-19.
Strengths and limitations of this study
In this study of infectious diseases in Chinese children and adolescents, we used systematic, long term, and comprehensive assessment coupled with high diagnostic accuracy. Under regulations from the China Centers for Disease Control’s (CDC) China Information System for Disease Control and Prevention (CISDCP), health facilities are required to report all cases of notifiable infectious diseases through the web based system, with the validity of the surveillance system being continuously monitored. In terms of system coverage, although CISDCP has not yet reached all health facilities in China, all types of health facilities are covered, including hospitals, CDCs, community health centres, township health centres, and village clinics. Total coverage is at least 85% throughout the country with more than 95% coverage of county level and above facilities each year (see supplementary fig S1). Among 69 881 facilities with reported case information in 2014, the participation levels were 3597 CDCs (100%), 13 764 hospitals (97%), and 37 494 township level clinics (89%).56 Despite this, the national coverage of CISDCP remains biased to some extent. The coverage within some provinces, particularly in the less developed provinces in western China, such as Tibet (18.6%), Qinghai (66.8%), and inner Mongolia (58.5%), was lower than in eastern more developed regions (95.1%). Furthermore, coverage of township level health facilities in rural areas remained less than that in urban cities with facilities above county level. It is therefore likely that we have underestimated infectious diseases in western less developed regions, and in remote towns and rural areas of China (see supplementary fig S2).
A second consideration is the validity of the surveillance system and accuracy of diagnosis. Generally, although suspected cases, pathogen carriers, and confirmed cases are all entered into CISDCP, in the present study we only analysed patients with a diagnosis confirmed by both uniform clinical standards and laboratory tests (ie, examination of, for example, pathogen, serology, imaging; see supplementary table S5 and the appendix). Decisions about diagnosis are overseen by professional trained specialists from the CISDCP, which ensures a high level of accuracy within this sample. For example, the diagnosis of HIV/AIDS is based on laboratory serum testing for HIV antibody and the detection of pathogens, combined with clinical symptoms and epidemiological data. However, under-reporting will be variable, most likely for people with subclinical and asymptomatic infections being managed at home, especially for seasonal influenza; hand, foot, and mouth disease; and infectious diarrhoea, particularly in remote areas. In contrast, serious infections that are highly contagious and might result in outbreaks or epidemics (categories A and B in China’s domestic notifiable infectious diseases classification; see supplementary table S4) will have high sensitivity and specificity. This includes the plague, cholera, HIV/AIDS, hepatitis A, tuberculosis, dysentery, and measles. It is possible that variable clinical expertise and technical expertise influences the number of confirmed cases in any setting. However, all 44 notifiable diseases in CISDCP have well established case definitions and diagnostic pathways, incorporating clinical features identification, laboratory confirmation, reporting procedures, and determination of specific pathogens. Nearly all of the 44 notifiable diseases had consistent case definitions and diagnostic criteria across the decade. Considering the consistent geographical variations in CISDCP coverage and the definitions and diagnostic criteria, and the stability of pathogenicity of most pathogenic agents, the likelihood of variation over time for subclinical and asymptomatic cases in the 44 notifiable diseases over the past decade is unlikely to have affected the trend analyses reported here. We note that estimates of the burden of death might vary between countries for mortality from seasonal influenza. For example, in China the use of estimates from death certificates that specifically list influenza will underestimate the burden of influenza, whereas the mathematical model to estimate the number of influenza deaths such as used in the United States could result in overestimation.57 Clearly, new challenges for the surveillance system are posed by emerging infectious diseases with an unclear disease course, such as covid-2019.
One further limitation of our study is that the study population were Chinese students. As we excluded children and adolescents who were not studying, we are unable to comment on the epidemiology of infectious diseases in preschool children.58 Given the free nine year compulsory education system in China, it is likely that the data for the younger student population will be broadly representative of this age group. The estimate bias in our study is likely to be higher with age (see supplementary fig S11), which might lead to underestimation of the actual burden of infectious diseases in adolescents, particularly for HIV/AIDS and other sexually transmitted diseases and bloodborne infections. Because of the social stigma around some sexually transmitted diseases, and lack of health service use for milder gastrointestinal infections, we could have underestimated the burden from these diseases.59 Although more males than females in each age group were not included in the analysis, the percentage of girls not included was larger (17.0% v 19.8%). As a result, although we underestimated the number of boys with notifiable infectious diseases nationally, the rates of underestimation were probably higher among girls who completed school early after nine year compulsory education (see supplementary fig S12). Both the number and the rates of underestimation of infectious disease burdens among children and adolescents of all occupations in this age group could be high in several provinces with large populations and high floating or mobile populations and low educational participation, such as Guangdong (non-students rates of 22.6%), Henan (24.9%), and Sichuan (20.0%; see supplementary fig S13).
Conclusion and policy implications
From 2008 to 2017, China achieved impressive reductions in the burden from infectious diseases in children and adolescents aged 6 to 22 years. This complements the reduction in mortality from infectious diseases in under 5s—a longstanding focus of the Millennium Development Goals, and will contribute to reductions in the overall burden from infectious diseases in China.1660 However, China’s rapid success poses challenges for policy makers as priorities for infectious disease control continue to evolve. Beyond maintaining the gains, the priorities for the coming decade include reducing regional inequalities; scaling-up vaccination for mumps, seasonal influenza, and hepatitis B; preventing further escalation of HIV/AIDS and other sexually transmitted diseases; and redoubling efforts around persisting diseases, including tuberculosis, rabies, and scarlet fever. Different responses will be needed by region and by age across childhood and adolescence, while the newer emerging disease epidemics will require rapid and targeted responses. Seasonal variation in respiratory infections and in gastrointestinal and enterovirus diseases reflect the high vulnerability of children and adolescents. A comprehensive national surveillance system remains an integral part of infectious disease control in these age groups to maintain the gains of recent decades and respond effectively to new epidemics.
What is already known on this topic
Even though China has made remarkable progress in the control of infectious diseases, the susceptibility of children and adolescents has made them a focus for many infectious disease strategies, including immunisation and enhanced surveillance
No study has yet reported on recent trends in infectious diseases among children and adolescents in China
What this study adds
The incidence of, and deaths from, infectious diseases in children and adolescents in China continues to decrease
Quarantinable diseases with high lethality have virtually disappeared, sexually transmitted diseases and bloodborne infections pose an increasing problem, and HIV is now the leading cause of death
The incidence of zoonotic infections and vectorborne diseases has been low since the epidemic of severe acute respiratory syndrome, but there is potential for major outbreaks
Acknowledgments
We thank the team members and health staff involved in China Information System for Disease Control and Prevention for their support.
Footnotes
Contributors: JM (majunt@bjmu.edu.cn) and YX (cyrss@126.com) contributed equally to the manuscript as corresponding authors and are the guarantors. They contributed to the conceptualisation and design of the study; supervised the data collection, statistical analyses, and initial drafting of the manuscript; and reviewed and revised the manuscript. YD and LW contributed equally to the manuscript as joint first authors. They conceptualised and designed the study, completed the statistical analyses, drafted the initial manuscript, and reviewed and revised the manuscript. GCP and SMS were senior authors and critically reviewed and revised the manuscript from preliminary draft to submission. DPB, JEM, and YS assisted with the data interpretation and reviewed and revised the manuscript. XR and ZL reviewed the manuscript. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding: This study was supported by the China Ministry of Science and Technology (grant 2018ZX10713001 to LW), National Natural Science Foundation of China (grant 91846302 to LW and YX, and grant 81673192 to JM, and China Scholarship Council to YD (201806010592) as well as Innovation Fund for Outstanding Doctoral Candidates of Peking University Health Science Centre to YD. The funder of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report.
Competing interests: All authors have completed the ICMJE uniform disclosure form at http://www.icmje.org/coi_disclosure.pdf and declare: support from the China Ministry of Science and Technology, National Natural Science Foundation of China, China Scholarship Council, and Peking University Health Science Centre for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Ethical approval: Not required as the deidentified data are publicly available.
Data sharing: The authors from Peking University and China CDC had full access to the data in the study. Data from the notifiable infectious disease report database are also open and available from the public health science data centre of the Chinese Center for Disease Control and Prevention and the official website of National Health and Family Planning Commission during the study period (http://www.phsciencedata.cn/Share/index.jsp; http://www.nhc.gov.cn/jkj/s3578/201802/de926bdb046749abb7b0a8e23d929104.shtml).
The manuscript’s guarantors (JM and YX) affirm that the manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as originally planned (and, if relevant, registered) have been explained.
Dissemination to participants and related patient and public communities: No members of the public were directly involved in the study design, outcome measures, analysis of data, or interpretation of study results. The results of this study will be reported through the media centre of the authors’ institutions under authors’ supervision. No plans exist to involve members of the public in dissemination.
Publisher’s note: Published maps are provided without any warranty of any kind, either express or implied. BMJ remains neutral with regard to jurisdictional claims in published maps.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.