Intended for healthcare professionals
Rapid response to:
Practice
Uncertainties
What is the best method for managing early miscarriage?
BMJ 2020; 368 doi: https://doi.org/10.1136/bmj.l6438 (Published 20 January 2020) Cite this as: BMJ 2020;368:l6438
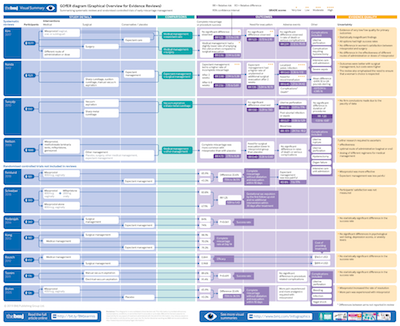
Visual summary available
See a full size version of this paper's GOfER diagram (Graphical Overview for Evidence Reviews)
Linked Opinion
Aftercare shouldn’t be an afterthought
Linked Opinion
Being more open might have helped me feel less isolated after a miscarriage
Rapid Response:
Serious omission of long term risk.
Dear Editor,
Regarding ‘What is the best method for managing early Miscarriage?’ we note serious omission of evaluation of the risk of subsequent premature birth with each method of management, in deciding what is best for the mother.
Shared decision making between clinician and patient is at the heart of good medical practice, and Chu et al make the point that women experiencing a miscarriage may have preferences about how they want the miscarriage to be managed or have concerns about surgery and risks to future fertility. Mothers may also have concerns about other future reproductive outcomes eg subsequent risk of premature birth or another miscarriage. The question ‘What is the best method for managing early miscarriage?’ needs to take into account longer term reproductive risks for the mother as well as short term ones heeded by the clinician.
Miscarriage has been shown in a meta-analysis by Swingle et al(1) to be associated with an increased risk of future preterm birth (PTB) with the risk of PTB increasing with the number of miscarriages. Adjusted odds ratios of 1.70 (1.51-1.92) for PTB after one miscarriage were reported by Basso in Denmark;(2) 1.6 (1.0-2.3) by El-Bastawissi in Seattle;(3) 1.31 (1.18-1.45) by Smith in Scotland;(4) 1.6 (1.2-2.0) by Bhattacharya in Aberdeen;(5) 1.12 (1.08-1.16) by Oliver-Williams in a later Scottish study(6) and 1.33 (1.04-1.70) by Omani-Samani in Iran.(7)
These risks are not negligible and increase after two miscarriages, with adjusted odds ratios of 2.13 (1.79-2.53);(2) (2.2 (0.7-2.0);(3) 1.50 (1.22-1.84);(4) 1.36 (1.25-1.47);(6) and 1.78 (1.15-2.74).(7) The Swingle meta-analysis reported an adjusted OR of 1.43 (1.05-1.66) after one miscarriage and 2.27 (1.98-2.81) after two or more miscarriages.(1)
Perhaps most worrying to a mother is the risk of extremely PTB which increases with several previous miscarriages.
Adjusted odds ratios for extreme PTB have been reported from Scotland of 2.81 (1.47-5.38)(4) after two or more miscarriages and 3.87 (2.85-5.26) after three or more miscarriages.(6) In Sweden Buchmayer reported an adjusted OR of 4.0 (2.3-7.1) after two or more miscarriages;(8) and Omani-Samani in Iran reported 4.10 (2.08-8.08) after three or more miscarriages.(7) These risks are significant.
It has been suggested that medical compared with surgical management of miscarriage in Scotland may reduce the risk of preterm birth in a subsequent pregnancy.(6) Inspection of the three Cochrane reviews cited showed no reference to differential risk of preterm birth (or other reproductive outcomes eg another miscarriage) after medical versus surgical management of miscarriage. Although the association between miscarriage and preterm birth in Scotland may have become weaker over time (possibly due to the adoption of medical methods of management) the risk is not zero. The incidence of preterm birth in Scotland is now at an all-time high.(9)
Chu et al make the point that expectant management of miscarriage has a higher frequency of subsequent surgical evacuation. Does this itself pose an additional risk of future preterm birth for the mother?
A few research units in the UK have set up the longitudinal studies required to investigate the longer term, rather than short-term effects of different types of management of miscarriage, using Scottish data. This data has been researched with the outcome of PTB in mind by Smith,(4) Bhattacharya,(5) Oliver-Williams,(6) and Pickering and Deeks(10) since the early 90’s.
Miscarriage has a high incidence in the UK and the risks of subsequent preterm birth carry potentially serious consequences to both the mother and the NHS, if ignored. The lack of consideration of available evidence about this outcome by the authors and Cochrane reviewers regarding risks of future preterm birth whilst managing miscarriage (either expectantly or by other means) is a serious omission of this paper and questions their stated goal of shared decision making. We hope future research will include and quantify these other important longer term, non-negligible risks for a mother.
1. Swingle HM, Colaizy TT, Zimmerman MB, Morriss FH, Jr. Abortion and the risk of subsequent preterm birth: a systematic review with meta-analyses. J Reprod Med 2009;54(2):95-108.
2. Basso O, Olsen J, Christensen K. Risk of preterm delivery, low birthweight and growth retardation following spontaneous abortion: a registry-based study in Denmark. Int J Epidemiol 1998;27(4):642-6.
3. El-Bastawissi AY, Sorensen TK, Akafomo CK, Frederick IO, Xiao R, Williams MA. History of fetal loss and other adverse pregnancy outcomes in relation to subsequent risk of preterm delivery. Matern Child Health J 2003;7(1):53-8.
4. Smith GC, Shah I, White IR, Pell JP, Crossley JA, Dobbie R. Maternal and biochemical predictors of spontaneous preterm birth among nulliparous women: a systematic analysis in relation to the degree of prematurity. Int J Epidemiol 2006;35(5):1169-77.
5. Bhattacharya S, Townend J, Shetty A, Campbell D, Bhattacharya S. Does miscarriage in an initial pregnancy lead to adverse obstetric and perinatal outcomes in the next continuing pregnancy? Bjog 2008;115(13):1623-9.
6. Oliver-Williams C, Fleming M, Wood AM, Smith G. Previous miscarriage and the subsequent risk of preterm birth in Scotland, 1980-2008: a historical cohort study. Bjog 2015;122(11):1525-34.
7. Omani-Samani R, Mansournia MA, Sepidarkish M, Almasi-Hashiani A, Safiri S, Vesali S, et al. Cross-sectional study of associations between prior spontaneous abortions and preterm delivery. Int J Gynaecol Obstet 2018;140(1):81-86.
8. Buchmayer SM, Sparen P, Cnattingius S. Previous pregnancy loss: risks related to severity of preterm delivery. Am J Obstet Gynecol 2004;191(4):1225-31.
9. Births in Scottish Hospitals Year ending 31st March 2019. In: Information Services Division Scotland; 2019.
10. Pickering RM, Deeks JJ. Risks of delivery during the 20th to the 36th week of gestation. Int J Epidemiol 1991;20(2):456-66.
Competing interests: No competing interests