Incretin based drugs and risk of cholangiocarcinoma among patients with type 2 diabetes: population based cohort study
BMJ 2018; 363 doi: https://doi.org/10.1136/bmj.k4880 (Published 05 December 2018) Cite this as: BMJ 2018;363:k4880Linked editorial
Incretins and cancer of the bile duct in type 2 diabetes

- Devin Abrahami, doctoral student12,
- Antonios Douros, postdoctoral fellow123,
- Hui Yin, statistician1,
- Oriana HY Yu, assistant professor and endocrinologist14,
- Jean-Luc Faillie, assistant professor of pharmacology5,
- François Montastruc, postdoctoral fellow16,
- Robert W Platt, professor of biostatistics12,
- Nathaniel Bouganim, assistant professor and oncologist78,
- Laurent Azoulay, associate professor of epidemiology and oncology128
- 1Centre for Clinical Epidemiology, Lady Davis Institute, Jewish General Hospital, 3755 Cote Sainte-Catherine Road, H425.1, Montreal, QC, H3T 1E2, Canada
- 2Department of Epidemiology, Biostatistics, and Occupational Health, McGill University, Montreal, QC, Canada
- 3Institute of Clinical Pharmacology and Toxicology, Charité University Medicine Berlin, Berlin, Germany
- 4Division of Endocrinology, Jewish General Hospital, Montreal, QC, Canada
- 5Department of Medical Pharmacology and Toxicology, CHU Montpellier; Laboratory of Biostatistics, Epidemiology and Public Health, University of Montpellier, Montpellier, France
- 6Department of Medical and Clinical Pharmacology, Centre of PharmacoVigilance and Pharmacoepidemiology, INSERM UMR 1027, CIC 1426, Toulouse University Hospital, Faculty of Medicine, University of Toulouse, France
- 7Department of Oncology, McGill University Health Centre, Montreal, QC, Canada
- 8Gerald Bronfman Department of Oncology, McGill University, Montreal, QC, Canada
- Correspondence to: L Azoulay laurent.azoulay{at}mcgill.ca (or @laurentazoulay0 on Twitter)
- Accepted 25 October 2018
Abstract
Objective To determine whether use of dipeptidyl peptidase-4 (DPP-4) inhibitors and glucagon-like peptide-1 (GLP-1) receptor agonists are associated with an increased risk of cholangiocarcinoma in adults with type 2 diabetes.
Design Population based cohort study.
Setting General practices contributing data to the UK Clinical Practice Research Datalink.
Participants 154 162 adults newly treated with antidiabetic drugs between 1 January 2007 and 31 March 2017, followed until 31 March 2018.
Main outcome measures Use of DPP-4 inhibitors and GLP-1 receptor agonists was modelled as a time varying variable and compared with use of other second or third line antidiabetic drugs. All exposures were lagged by one year to account for cancer latency and to minimise reverse causality. Cox proportional hazards models were used to estimate hazard ratios and 95% confidence intervals of incident cholangiocarcinoma associated with use of DPP-4 inhibitors and GLP-1 receptor agonists, separately. A post hoc pharmacovigilance analysis was conducted using the World Health Organization’s global individual case safety report database, VigiBase, to estimate reporting odds ratios of cholangiocarcinoma.
Results During 614 274 person years of follow-up, 105 incident cholangiocarcinoma events occurred (rate 17.1 per 100 000 person years). Use of DPP-4 inhibitors was associated with a 77% increased hazard of cholangiocarcinoma (hazard ratio 1.77, 95% confidence interval 1.04 to 3.01). Use of GLP-1 receptor agonists was associated with an increased hazard with a wide confidence interval (hazard ratio 1.97, 0.83 to 4.66). In the pharmacovigilance analysis, the use of DPP-4 inhibitors and GLP-1 receptor agonists were both associated with increased reporting odds ratios for cholangiocarcinoma, compared with use of sulfonylureas or thiazolidinediones (1.63, 1.00 to 2.66, 4.73, 2.95 to 7.58, respectively).
Conclusion Compared with use of other second or third line antidiabetic drugs, use of DPP-4 inhibitors, and possibly GLP-1 receptor agonists, might be associated with an increased risk of cholangiocarcinoma in adults with type 2 diabetes.
Introduction
Dipeptidyl peptidase-4 (DPP-4) inhibitors and glucagon-like peptide-1 (GLP-1) receptor agonists are second or third line drugs commonly used in the management of type 2 diabetes.1 These incretin based drugs work through the effects of GLP-1, a gut derived incretin hormone that stimulates insulin secretion in a glucose dependent fashion.2 GLP-1 receptor agonists directly stimulate the GLP-1 receptor, whereas DPP-4 inhibitors inhibit the degradation of endogenous GLP-1.3
Although incretin based drugs have favourable clinical effects,45 some biological evidence suggests that the incretin system might be involved in the development of cholangiocarcinoma (bile duct cancer), a rare but highly fatal cancer.6 Indeed, the GLP-1 receptor is expressed on cholangiocytes,7 the expression of which was shown to be increased in tumour tissue samples of patients with intrahepatic cholangiocarcinoma.8 Activation of the GLP-1 receptor has also been shown to increase the proliferation rate of cholangiocytes both in vitro and in vivo,7 while lowering the rate of apoptosis.9 To date, only two large trials of incretin based drugs have reported on hepatobiliary cancers, but with conflicting findings.1011 In one of these trials10 more hepatobiliary cancers occurred with use of the GLP-1 receptor agonist liraglutide than with placebo (13 v 8); this included six versus two cases of biliary cancer, respectively (all but one in the liraglutide group were cholangiocarcinomas, as reported by the investigators).12 In contrast, fewer events were reported with use of the DPP-4 inhibitor saxagliptin than with placebo (9 v 12), although this trial did not differentiate between hepatic and biliary cancers.11 Given the conflicting evidence, we carried out a population based cohort study to determine whether use of DPP-4 inhibitors and GLP-1 receptor agonists is associated with an increased risk of cholangiocarcinoma in adults with type 2 diabetes.
Methods
Data source
This study was conducted using the Clinical Practice Research Datalink (CPRD), a large primary care database shown to be representative of the general United Kingdom population.13 The CPRD uses the Read code classification to record medical diagnoses and procedures,14 which have been shown to be of high quality and validity.1516 The database also includes demographic and anthropometric data, laboratory test results, as well as prescription information based on the British National Formulary (BNF). Cancer diagnoses recorded in the CPRD have been previously validated.17181920
Study population
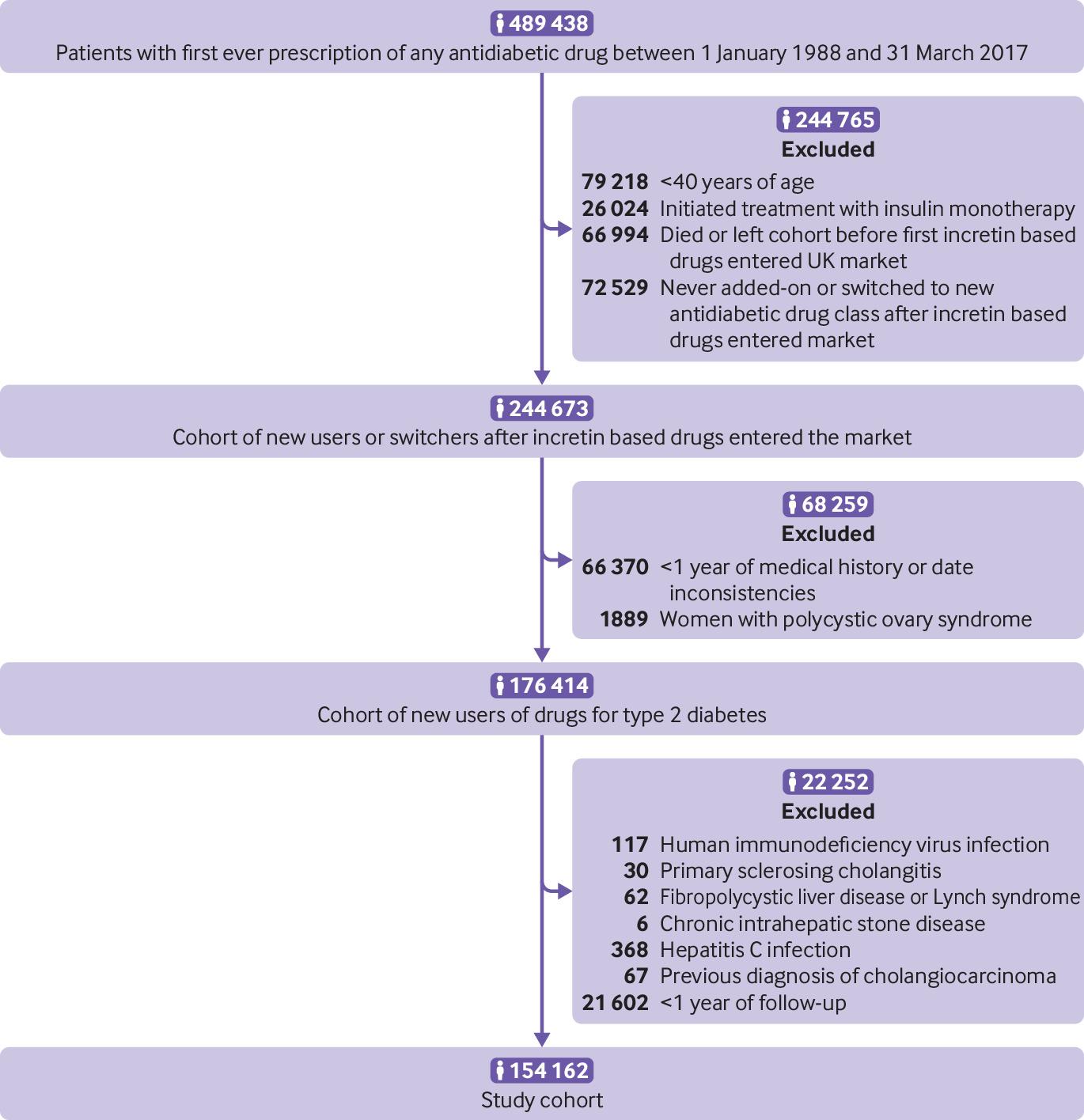
We identified a base cohort of adults newly treated with antidiabetic drugs (metformin, sulfonylureas, meglitinides, thiazolidinediones, acarbose, DPP-4 inhibitors, GLP-1 receptor agonists, sodium-glucose cotransporter-2 inhibitors, and insulin using BNF codes, supplementary table 1) between 1 January 1988 and 31 March 2017. We excluded people aged less than 40 years, as well as those who were prescribed insulin in monotherapy as their first ever antidiabetic prescription, as these might represent people with type 1 diabetes. Using this base cohort, we assembled a cohort of adults who initiated a new antidiabetic drug class in or after 2007, the year the first incretin based drugs entered the UK market.4 This cohort included those initiating their first ever antidiabetic drug, as well as those who switched to or added-on an antidiabetic drug class not previously used. Cohort entry was defined by the date of this new prescription. At this stage, we excluded people with less than one year of medical history in the CPRD before cohort entry and women with a history of polycystic ovary syndrome (as this is another indication for metformin). We also excluded those with a previous diagnosis of cholangiocarcinoma (identified using Read codes; supplementary table 2), as well as those with a previous diagnosis of known, but relatively rare risk factors for this cancer (primary sclerosing cholangitis, fibropolycystic liver disease, chronic intrahepatic stone disease, Lynch syndrome, hepatitis C infection, and human immunodeficiency virus infection) at any time before cohort entry. Finally, we excluded those with less than one year of follow-up after cohort entry, to allow for a sufficient latency period and to minimise reverse causality. Thus, participants were followed starting one year after cohort entry until an incident diagnosis of cholangiocarcinoma (including all subtypes, identified using Read codes; supplementary table 2), or censored on death from any cause, end of registration with the general practice, or end of the study period (31 March 2018), whichever occurred first.
Exposure definition
We used a time varying exposure definition, where we categorised each person day of follow-up into one of four mutually exclusive categories: use of DPP-4 inhibitors (alone or in combination with other antidiabetic drugs, excluding GLP-1 receptor agonists); use of GLP-1 receptor agonists (alone or in combination with other antidiabetic drugs, including previous use of DPP-4 inhibitors, as this is a common treatment strategy); use of other second or third line drugs (defined as initiation of treatment with either thiazolidinediones, prandial glucose regulators, acarbose, sodium-glucose cotransporter-2 inhibitors, insulin, or combination of oral antidiabetic drugs; or switch to or add-on of an antidiabetic drug, including insulin, after failure with metformin or sulfonylurea in monotherapy); and use of first line drugs (defined as use of metformin or sulfonylurea in monotherapy). Exposures were lagged by one year for latency purposes and to minimise reverse causality. As part of this exposure definition, we considered participants switching to or adding-on an incretin based drug to be exposed until the end of follow-up (analogous to an intention-to-treat approach; supplementary figure 1). To minimise potential confounding by indication, we compared use of incretin based drugs (second or third line drugs)1 with use of other second or third line drugs.
We also defined use of incretin based drugs according to cumulative duration of use and time since initiation as secondary time varying exposure definitions. Cumulative duration of use was calculated as the sum of the durations of each prescription from cohort entry until the risk set date (ie, time of the event), and time since initiation was defined as the time from the first prescription of an incretin based drug until the time of the risk set date.
Statistical analysis
For each exposure category we calculated crude incidence rates of cholangiocarcinoma with 95% confidence intervals, based on the Poisson distribution. Time dependent Cox proportional hazards models were used to estimate hazard ratios and 95% confidence intervals of cholangiocarcinoma associated with the use of DPP-4 inhibitors and GLP-1 receptor agonists, separately, when compared with use of other second or third line drugs. The models were adjusted for the potential confounders measured at cohort entry: age, sex, year of cohort entry, obesity (body mass index ≥30), smoking status, alcohol related disorders (alcohol dependency, alcoholic cirrhosis of the liver, alcoholic hepatitis, hepatic failure), Charlson comorbidity index score, inflammatory bowel disease, gallbladder disease (bile duct disease, primary biliary cirrhosis, cholecystectomy), glycated haemoglobin (HbA1c, last laboratory result before cohort entry) level, and duration of diabetes (defined as time between cohort entry and earliest date of type 2 diabetes diagnosis, HbA1c level ≥6.5%, or first prescription for an antidiabetic drug). Variables with missing data (HbA1c, body mass index, and smoking status) were imputed using multiple imputation methods (supplementary methods 1).2122
Secondary analyses
We performed three prespecified secondary analyses. To assess possible duration-response relations, we investigated the association between cumulative duration of use and time since initiation on the risk of cholangiocarcinoma. For these time dependent analyses, we estimated hazard ratios for three (≤1 year, 1.1-2 years, and >2 years) and two (≤2 years and >2 years) predefined duration categories, respectively. We also assessed whether there was an association according to the primary excretory pathway (renal versus biliary) of each drug type.23
Sensitivity analyses
We conducted five sensitivity analyses to assess the robustness of our findings. Firstly, we repeated the analysis by increasing the exposure lag period to two and three years, given the uncertainty related to the optimal length of the latency time window. For these analyses, we excluded participants with less than two years and less than three years of follow-up, respectively. As some cases of cholangiocarcinoma have been reported to occur shortly after drug initiation,24 we also removed the lag period to investigate a potential rapid tumour promoter effect. We did not impose a minimum follow-up time for this analysis. Secondly, we repeated the analysis using the Fine and Gray subdistribution Cox proportional hazards model25 to investigate possible competing risk by death from any cause. Thirdly, we considered a stricter exposure definition, where use of DPP-4 inhibitors and GLP-1 receptor agonists was redefined as participants receiving at least four prescriptions within a 12 month moving window; participants were considered exposed one year after their fourth qualifying prescription. Fourthly, we fit a marginal structural model to investigate the impact of potential time dependent confounding using inverse probability of treatment and censoring weighting (supplementary methods 2). Finally, we conducted a post hoc sensitivity analysis using the Array approach to quantify the effect an unknown or unmeasured confounder would have on our findings.26
Ancillary analyses
To further investigate the potential impact of confounding by disease severity, we conducted two ancillary analyses. In the first analysis, we used insulin as a negative control exposure.27 Insulin is a last line treatment that has not been associated with incidence of cholangiocarcinoma. In keeping with the primary analysis, we compared use of insulin with use of other second or third line drugs (supplementary methods 3). In the second analysis, we matched new users of incretin based drugs to new users of other second or third line drugs on propensity scores (supplementary methods 4 and supplementary figure 2). Cumulative incidence curves of cholangiocarcinoma were plotted for the matched cohort using the Kaplan-Meier method.
To further assess this association, we also conducted a post hoc pharmacovigilance analysis using the World Health Organization’s global individual case safety report database, VigiBase. This database includes more than 16 million individual case safety reports from over 150 countries worldwide.28 Using VigiBase, we conducted disproportionality analyses to estimate reporting odds ratios of cholangiocarcinoma compared with all other adverse drug reactions (supplementary methods 5). In a first analysis, we estimated the reporting odds ratios among users of DPP-4 inhibitors and GLP-1 receptor agonists, separately, compared with users of sulfonylureas or thiazolidinediones (other second or third line drugs). In a second analysis, we assessed the effect of potential confounding by disease severity by repeating the analysis using a negative control exposure consisting of long acting insulin analogues. All analyses were conducted with SAS version 9.4 (SAS institute, Cary, NC) and R (R Foundation for Statistical Computing, Vienna, Austria).
Patient and public involvement
We did not include patients as study participants as our study involved the use of secondary data. Patients were not involved in the design or implementation of the study. We do not plan to involve patients in the dissemination of results, nor will we disseminate results directly to patients, beyond our general media communications plan.
Results
The cohort included 154 162 patients (fig 1) followed for a median of 4.6 years (maximum follow-up 11.2 years) including the one year post cohort entry lag period. The median duration of follow-up for participants using DPP-4 inhibitors, GLP-1 receptor agonists, and other second or third line drugs was 3.4 (maximum follow-up 10.8), 4.4 (10.7), and 3.8 (11.2) years, respectively. During 614 274 person years of follow-up, 105 incident cholangiocarcinoma events occurred, yielding a crude incidence rate of 17.1 (95% confidence interval 14.0 to 20.7) per 100 000 person years. During the study period, 32 731 (21.2%) participants were prescribed DPP-4 inhibitors, 6174 (4.0%) GLP-1 receptor agonists, and 4450 (2.9%) both drugs. The median duration of use of DPP-4 inhibitors, GLP-1 receptor agonists, and other second or third line drugs was 1.9 (maximum duration 10.1), 1.6 (9.8), and 3.1 (11.0) years, respectively.

Study flowchart of participants included in cohort
{kind=link}
Table 1 presents the baseline characteristics for the entire cohort and stratified according to use of DPP-4 inhibitors, GLP-1 receptor agonists, and other second or third line drugs at cohort entry. Overall, users of DPP-4 inhibitors and GLP-1 receptor agonists were similar to users of other second or third line drugs for sex, smoking status, prevalence of inflammatory bowel disease, and history of gallbladder disease. In contrast, DPP-4 inhibitor users and GLP-1 receptor agonist users were more likely to be obese, have longer durations of diabetes, and have a higher Charlson comorbidity index score.
Baseline characteristics of cohort and by antidiabetic treatment at cohort entry. Values are numbers (percentages) unless stated otherwise
Table 2 presents the results of the primary analysis for DPP-4 inhibitors and GLP-1 receptor agonists. Compared with use of other second or third line drugs, use of DPP-4 inhibitors was associated with a 77% increase in the hazards of cholangiocarcinoma (hazard ratio 1.77, 95% confidence interval 1.04 to 3.01). The secondary analyses by cumulative duration of use and time since initiation yielded increased hazard ratios for cumulative durations of one year to two years and with more than two years since treatment initiation, respectively, but the confidence intervals were wide and included the null value (supplementary table 3). When investigating specific DPP-4 inhibitors, those primarily excreted through biliary pathways generated a higher hazard ratio than those excreted through renal pathways (2.25, 95% confidence interval 0.86 to 5.90 and 1.64, 0.92 to 2.90, respectively; supplementary table 3), although both generated wide and overlapping confidence intervals. Compared with use of other second or third line drugs, use of GLP-1 receptor agonists generated an increased association with a wide confidence interval (1.97, 0.83 to 4.66; table 2). The low number of events with GLP-1 receptor agonists (n=7) did not allow for the assessment of duration-response relations or stratification by drug type.
Crude and adjusted hazard ratios for association between use of DPP-4 inhibitors and GLP-1 receptor agonists and risk of cholangiocarcinoma
Sensitivity and ancillary analyses
The sensitivity analyses led to generally consistent results (supplementary tables 4-13), except for the lagged analyses with hazard ratios ranging from 1.31 to 1.62 for DPP-4 inhibitors and 1.42 to 2.38 for GLP-1 receptor agonists. The stricter exposure definition generated hazard ratios that excluded the null for both DPP-4 inhibitors (1.77, 95% confidence interval 1.01 to 3.11) and GLP-1 receptor agonists (2.46, 1.04 to 5.85).
In the ancillary analysis using a negative control exposure, the use of insulin was not associated with an increased risk of cholangiocarcinoma (0.89, 95% confidence interval 0.36 to 2.19) compared with use of other second or third line drugs (supplementary table 10). The propensity score matched analysis (supplementary figure 3) yielded groups that were well balanced on all covariates, with none of the standard differences exceeding 0.02 (supplementary table 11). Compared with other second or third line drugs, DPP-4 inhibitors generated a hazard ratio of similar magnitude to the one generated in the primary analysis (1.71, 0.86 to 3.43), but with a wider confidence interval that included the null value owing to the fewer events in the exposed groups (supplementary table 12). The cumulative incidence curves diverged after two years of use (supplementary figure 4). The analysis of GLP-1 receptor agonists did not generate a stable estimate owing to the low number of events (<5).
Table 3 presents the results of the pharmacovigilance analyses. Compared with use of sulfonylureas or thiazolidinediones, use of DPP-4 inhibitors was associated with an increase in the reporting odds ratio of cholangiocarcinoma (1.63, 95% confidence interval 1.00 to 2.66). A similar increase in the reporting odds ratio was observed with use of GLP-1 receptor agonists (4.73, 2.95 to 7.58). In contrast, the use of long acting insulin analogues was not associated with cholangiocarcinoma (1.24, 0.72 to 2.15).
Reporting odds ratios of cholangiocarcinoma using World Health Organization VigiBase
Discussion
In this study, use of dipeptidyl peptidase-4 (DPP-4) inhibitors was associated with a near doubling of the risk for cholangiocarcinoma. The use of glucagon-like peptide-1 (GLP-1) receptor agonists was also associated with an increased hazard ratio of similar magnitude but generated a wide confidence interval that included the null value. As expected, no association was observed with insulin in an ancillary analysis. Finally, in a post hoc pharmacovigilance analysis, increased reporting odds ratios were observed for both DPP-4 inhibitors and GLP-1 receptor agonists, whereas a reporting odds ratio close to the null value was observed for long acting insulin analogues.
Comparison with previous studies
Several large trials of incretin based drugs have been conducted,101112293031323334353637 but of these, only two have reported on the frequency of hepatobiliary cancers. In the Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results (LEADER) trial of liraglutide, 13 events occurred in the liraglutide group compared with eight in the placebo group (hazard ratio 1.62, 95% confidence interval 0.67 to 3.90).10 A post hoc analysis providing a breakdown of hepatic versus biliary cancers reported six events in the liraglutide group and two in the placebo group.12 As reported by the trial investigators, all of these biliary cancers were cholangiocarcinomas with the exception of one adenocarcinoma of the gallbladder in the liraglutide group.12 In contrast, the imbalance favoured the placebo group in a post hoc analysis of the Saxagliptin Assessment of Vascular Outcomes Recorded in Patients with Diabetes Mellitus (SAVOR)–Thrombolysis in Myocardial Infarction (TIMI) 53 trial, with 12 events in the placebo group compared with nine in the saxagliptin group (hazard ratio 0.75, 95% confidence interval 0.30 to 1.76).11 However, these trials were not designed nor powered to assess cholangiocarcinoma as an outcome (sample sizes of 9340 and 16 942 with relatively short median durations of follow-up of 3.8 and 2.1 years for LEADER and SAVOR-TIMI 53, respectively).1011
An association between incretin based drugs and incidence of cholangiocarcinoma is biologically plausible. One mechanism could involve the increased GLP-1 levels associated with use of both DPP-4 inhibitors and GLP-1 receptor agonists; GLP-1 might promote the development of cholangiocarcinoma through its proliferative and anti-apoptotic effects on cholangiocytes.79 Another mechanism could involve chronic inflammation of the biliary epithelium, bile stasis, and bacterial infections,38 which might be a particular concern with GLP-1 receptor agonists. These drugs have been associated with an increased risk of gallbladder related events (such as cholelithiasis, cholecystitis, cholangitis) in an observational study39 and in the LEADER trial.10 Finally, we observed increased hazard ratios in secondary analyses assessing possible duration-response relations with DPP-4 inhibitors. Specifically, the hazard ratio was particularly increased with cumulative durations ranging between one and two years of use and with more than two years since treatment initiation. Although these relatively rapid effects suggest that these drugs might act as tumour promoters among susceptible people, these secondary analyses were based on few events that generated wide confidence intervals and should thus be interpreted with caution.
Strengths and limitations of this study
Our study has several strengths. Firstly, the cohort was restricted to new users of antidiabetic drugs, thereby eliminating biases associated with the inclusion of prevalent users.40 Secondly, comparing incretin based drugs (primarily used as second or third line drugs)1 with a comparator consisting of other second or third line drugs likely minimised confounding by indication. Thirdly, we used a time varying exposure definition, which eliminated immortal time bias by allowing participants to contribute person time to different exposure categories during the follow-up period.41 Fourthly, our results remained consistent across several sensitivity analyses, including one using a stricter exposure definition where the use of both DPP-4 inhibitors and GLP-1 receptor agonists was associated with an increased risk of cholangiocarcinoma. Finally, the pharmacovigilance analysis, while subject to known limitations such as underreporting,42 yielded results that were generally consistent with those of the cohort study. Although there are some important differences between the two studies, the concordance of the findings is reassuring.
This study has some limitations. Firstly, prescriptions in the Clinical Practice Research Datalink (CPRD) are those issued by general practitioners and not specialists. As type 2 diabetes is managed almost entirely through primary care in the UK,43 we expect such misclassification to be minimal. We also did not have any information on patient adherence to treatment, although this misclassification was likely non-differential between the exposure groups. Secondly, the validity of cholangiocarcinoma has not been previously assessed in the CPRD. However, relatively rare gastrointestinal cancers not under the care of general practitioners, such as pancreatic cancer, have been shown to be well recorded in the CPRD in most,181920 but not all,17 cancer validation studies. While one study reported more than 50% non-concordance of these cancers between the CPRD and other datasets (eg, National Cancer Data Repository and Hospital Episodes Statistics database),17 two other validation studies conducted among people with type 2 diabetes found concordance rates of more than 90% when CPRD was compared with these datasets.1819 Similar findings were observed in a third validation study conducted among the general population.20 However, to tackle the potential impact of misclassification resulting from restricting the outcome definition to CPRD defined diagnoses, we conducted a sensitivity analysis showing the impact of imperfect sensitivity and specificity on the observed point estimate (supplementary table 13). Indeed, the specificity (and not sensitivity) of the outcome definition would need to be less than 60% to substantially bias the point estimate. In our study, we expect high specificity given the rarity of cholangiocarcinoma and general practitioners’ unfamiliarity with this cancer; this is typically the case with rare outcomes.44 Thirdly, we were unable to stratify by cholangiocarcinoma subtype as this level of detail is not consistently recorded in the CPRD. Fourthly, as with all observational studies, residual confounding is possible. We conducted several sensitivity and ancillary analyses specifically designed to assess the potential impact of residual confounding. These included a marginal structural model aimed at investigating the impact of potential time dependent confounding, and a propensity score matched analysis; these analyses yielded hazard ratios of similar magnitude as the one generated in the primary analysis. Furthermore, use of insulin as a negative control exposure yielded a hazard ratio close to the null value. Moreover, the Array approach26 shows that a hypothetical confounder would need to be strongly imbalanced between the exposure groups while also being strongly associated with the outcome to affect the point estimate observed for DPP-4 inhibitors (supplementary figure 5). Fifthly, the median length of follow-up in our study was limited to 4.6 years, including the one year lag period imposed at cohort entry. However, this study was based in part on imbalances of hepatobiliary cancer events observed in trials of even shorter duration.1011 Finally, despite the relatively large sample size of our cohort (n=154 162), cholangiocarcinoma is an extremely rare cancer45 that generated few exposed events; 27 events occurred in the DPP-4 inhibitor group, whereas seven occurred in the GLP-1 receptor agonist group. As such, it was not possible to conduct secondary analyses among users of GLP-1 receptor agonists, and the secondary analyses among users of DPP-4 inhibitors should be interpreted with caution.
Conclusions
The results of this large population based cohort study indicate that use of DPP-4 inhibitors, and possibly GLP-1 receptor agonists, might be associated with an increased risk of cholangiocarcinoma, although the absolute risk is low. Given the high fatality rate of this cancer, post hoc analyses of randomised controlled trials and additional observational studies are needed to corroborate our findings.
What is already known on this topic
The glucagon-like peptide-1 (GLP-1) incretin hormone has been shown to have proliferative and anti-apoptotic effects on cholangiocytes—cells that line the biliary tree
This raises the possibility that the incretin based drugs dipeptidyl peptidase-4 (DPP-4) inhibitors and GLP-1 receptor agonists could increase the risk of cholangiocarcinoma, a rare but highly fatal cancer
Although imbalances in hepatobiliary cancers have been observed in some of the large randomised controlled trials of incretin based drugs, no observational study has investigated this association in the real world setting
What this study adds
Use of DPP-4 inhibitors was associated with a near doubling of the risk of cholangiocarcinoma
An association of similar magnitude was observed with GLP-1 receptor agonists, but this did not reach statistical significance
Incretin based drugs therefore might be associated with an increased risk of cholangiocarcinoma in people with type 2 diabetes
Acknowledgments
We thank the Uppsala Monitoring Centre and the National Pharmacovigilance Centers for providing the pharmacovigilance data for the present study. The information presented in this study does not represent the opinion of the World Health Organization. Access to the WHO global individual case safety report database, VigiBase, is available without fees to FM and J-LF.
DA is the recipient of a doctoral award from the Fonds de recherche du Québec–Santé (FRQS). AD is the recipient of a research fellowship from the German Research Foundation (Deutsche Forschungsgemeinschaft, DFG). OHYY holds a Chercheur-Boursier Clinicien junior 1 award from the FRQS. FM is the recipient of postdoctoral fellowships from La Fondation Pierre Deniker and Toulouse University Hospital (CHU Toulouse). RWP is the Albert Boehringer Chair in Pharmacoepidemiology at McGill University. LA holds a Chercheur-Boursier senior award from the FRQS and is the recipient of a William Dawson Scholar award from McGill University.
Footnotes
Contributors: All authors conceived and designed the study. LA acquired the data. DA, AD, HY, and LA did the statistical analyses. All authors analysed and interpreted the data. DA wrote the manuscript, and all authors critically revised the manuscript. LA supervised the study and is the guarantor. All authors approved the final version of the manuscript and agree to be accountable for the accuracy of the work. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding: This study was funded by a foundation scheme grant from the Canadian Institutes of Health Research (FDN-333744). The sponsor had no influence on the design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review, or approval of the manuscript.
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: this study was funded by the Canadian Institutes of Health Research. RWP received consulting fees for work unrelated to this project from Amgen, Eli Lilly, Merck, and Pfizer. All other authors have no conflicts to disclose, and have no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Ethical approval: The study protocol was approved by the independent scientific advisory committee of the Clinical Practice Research Datalink (protocol No 17_271RMn2A) and by the research ethics board of Jewish General Hospital, Montreal, Quebec, Canada.
Data sharing: No additional data available.
Transparency: The guarantor (LA) affirms that this manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.