Business not as usual: how multisectoral collaboration can promote transformative change for health and sustainable development
BMJ 2018; 363 doi: https://doi.org/10.1136/bmj.k4771 (Published 07 December 2018) Cite this as: BMJ 2018;363:k4771

- Shyama Kuruvilla, senior strategic adviser1,
- Rachael Hinton, technical officer2,
- Ties Boerma, director and professor3,
- Ryan Bunney, intern4,
- Nuria Casamitjana, training and education director5,
- Rafael Cortez, senior economist and team lead6,
- Patrizia Fracassi, senior nutrition analyst and strategy adviser7,
- Jennifer Franz-Vasdeki, independent consultant8,
- Daniel Helldén, research assistant9,
- Joanne McManus, independent consultant10,
- Susan Papp, managing director of policy and advocacy11,
- Kumanan Rasanathan, coordinator health systems12,
- Jennifer Requejo, senior adviser13,
- Karlee L Silver, co-chief executive officer14,
- Petra Tenhoope-Bender, technical adviser15,
- Yael Velleman, senior policy analyst16,
- Mary Nell Wegner, executive director17,
- Corinne E Armstrong, independent consultant18,
- Sarah Barnett, counsultant19,
- Carla Blauvelt, country director20,
- Saidatul Norbaya Buang, public health physician21,
- Louise Bury, independent consultant22,
- Emily A Callahan, consultant23,
- Jai K Das, senior instructor24,
- Vandana Gurnani, joint secretary25,
- Mary White Kaba, independent consultant26,
- Helia Molina Milman, dean of the medical sciences faculty27,
- John Murray, independent consultant28,
- Ilona Renner, research manager29,
- Marion Leslie Roche, senior technical adviser30,
- Victoria Saint, independent consultant31,
- Sarah Simpson, independent consultant32,
- Hasina Subedar, adviser33,
- Daria Ukhova, independent consultant34,
- Claudia Nieves Velásquez, independent consultant35,
- Patricia Young, director36,
- Wendy Graham, professor37,
- PMNCH Multisectoral Collaboration Study Group
- 1World Health Organization, Geneva, Switzerland
- 2Partnership for Maternal, Newborn, and Child Health, Geneva, Switzerland
- 3Countdown to 2030, and University of Manitoba, Manitoba, Canada
- 4World Health Organization, Chicago, USA
- 5ISGlobal, Barcelona Institute for Global Health, University of Barcelona, Spain
- 6World Bank, Washington DC, USA
- 7Scaling up Nutrition Secretariat, Geneva, Switzerland
- 8Seattle, USA
- 9Department of Public Health Sciences, Karolinska Institutet, Stockholm, Sweden
- 10Oxford, UK
- 11Women Deliver, New York, USA
- 12WHO Cambodia, Phnom Penh, Cambodia
- 13UNICEF, New York, USA
- 14Grand Challenges Canada, Toronto, Canada
- 15UNFPA, Geneva, Switzerland
- 16WaterAid, London, UK
- 17Maternal Health Task Force, Harvard University TH Chan School of Public Health, Boston, Massachusetts, USA
- 18London, UK
- 19SB Consultancy World, Bristol, UK
- 20VillageReach, Lilongwe, Malawi
- 21Family Health Development Division, Ministry of Health, Kuala Lumpur, Malaysia
- 22Global Research Consultancy, Ipswich, UK
- 23EAC Health and Nutrition, Washington DC, USA
- 24Division of Women and Child Health, Aga Khan University, Karachi, Pakistan
- 25Ministry of Health and Family Welfare, Government of India, New Delhi, India
- 26Montreal, Canada
- 27University of Santiago, Chile
- 28Iowa City, Iowa, USA
- 29National Centre for Early Prevention, Federal Centre for Health Education, Cologne, Germany
- 30Nutrition International, Adolescents’ and Women’s Health and Nutrition, Ottawa, Ontario, Canada
- 31Berlin, Germany, Council on International Educational Exchange (CIEE), Berlin, Germany
- 32EquiACT 71, Montluel, France
- 33National Department of Health, Pretoria, South Africa
- 34Berlin, Germany
- 35Guatemala City, Guatemala
- 36Child to Child, London, UK
- 37London School of Hygiene and Tropical Medicine, London, UK
- Correspondence to: S Kuruvilla kuruvillas{at}who.int
The 2030 Agenda for Sustainable Development states that if the “interlinkages and integrated nature of the Sustainable Development Goals (SDGs)” are realised, then “the lives of all will be profoundly improved and our world will be transformed for the better.”1
In line with the SDGs, multisectoral action (box 1) is a key action area of the Global Strategy for Women’s, Children’s and Adolescents’ Health.2 It is central to other global health priorities, for example, universal health coverage, the prevention and control of non-communicable diseases, and the “health in all policies” approach.345 A fundamental question arises: could the transformative changes envisioned in the SDGs be achieved by each sector acting independently, or do they require multisectoral collaboration (see box 1 for definitions)?
Definitions
Stakeholders are actors, whether individuals or groups, who can influence or be affected by a particular concern, process, or outcome.6 Stakeholders may include governments, non-governmental organisations (NGOs), civil society, private actors, international organisations, donors, service users, service providers, the media, and other groups.
Sectors comprise an array of actors and institutions linked by their formal, functional roles or area of work. Highlighted here are sectors related to specific policy areas or topics, including those relevant to the 17 SDGs. These sectors can be supported by institutions, which assume cross cutting functions, such as those responsible for budgeting or planning. These sectors and cross cutting institutions can include both public and private entities. The term “sector” also can be used to denote these entities, as in discussions about the “public sector” and the “private sector.”7
Multisectoral action89 can occur in three ways:
Independent action: individual sectors independently undertaking their core business and advancing their own sectors’ goals; in so doing they can also contribute to other sectors’ goals. For example, health sector investments in children’s health could also improve educational performance, and better health and education could contribute to higher productivity and wages in adulthood.
Intentional collaboration: multiple sectors and stakeholders intentionally coming together and collaborating in a managed process to achieve shared outcomes. This is referred to in this paper as multisectoral collaboration. In the context of the SDGs, shared outcomes of multisectoral collaboration could include joint programmes for poverty reduction, better health and wellbeing, high quality education, improved nutrition, gender equality, economic growth, and other outcomes influencing health and sustainable development.
Contextual, ecological interactions: there are individual, social, and environmental factors, beyond the remit of any sector, that intersect with and influence sectoral work. For example, individuals’ biology and behaviours, sociocultural norms, political ideologies, and environmental phenomena. Sectors independently and collaboratively could seek to tackle how these matters influence implementation and impact.
To achieve the SDGs, it is vital to know when multisectoral collaboration will be most effective, how to ensure efficiency, and what factors enable these collaborations to contribute to transformative change—to “business not as usual.”
The series on success factors for women’s and children’s health and other studies found that during the years of the millennium development goals (2000-2015), sectors beyond health contributed to around 50% of the reductions in child and maternal mortality achieved in low and middle income countries.1011 This work also showed that some countries’ health and development outcomes were improved by health and other sectors acting independently, but in others, improvements were achieved by intentional multisectoral collaboration.10
The literature documents how multisectoral collaborations have been planned, implemented, and sustained in various fields of health and in other sectors.89121314 For example, in the field of nutrition, multisectoral collaboration to reduce stunting in children in Peru was achieved when the government required related sectors to work together in “convergence” programming and to align targets and interventions.13 With a focus on improving the wellbeing of First Nations people in Canada, a range of multisectoral determinants were considered with respect to community autonomy and governance, different belief systems, social capital, health and social services, and historical, ecological, and life course considerations.12
Limited evidence is available about how multisectoral collaborations work specifically to improve women’s, children’s, and adolescents’ health, and about best practices and generalisable principles.14 For example, while it is known that policy and context matter for efforts to improve child development and life outcomes,15 there is less understanding of the specific entry points and opportunities for involvement by diverse sectors and stakeholders on these matters.1415
To contribute to the evidence, the Partnership for Maternal, Newborn, and Child Health (PMNCH) supported the development of 12 country case studies. These were selected from responses to a global call for proposals, using weighted selection criteria.
Each country case study relates to one of six thematic priorities on which PMNCH and other Every Woman Every Child (EWEC) partners agreed to focus on for 2018-2020 to support country implementation of the global strategy.16 Since the call for proposals intentionally focused on health and partnership across sectors, all the country case studies related to SDGs 3 and 17; other SDGs were covered based on the context of the multisectoral collaborations (table 1).
Twelve case study countries by Every Woman Every Child theme and focal Sustainable Development Goals
The papers in this series show diversity in the selected case studies—in relation to country income level, the type and number of sectors and stakeholders involved, breadth of scope from sub-national or pilot programmes to those at scale, and the time span. Some, for example, began as non-governmental organisation (NGO) led pilots implemented in remote rural areas and were scaled up to national coverage; others were initiated by a president or prime minister and rolled out nationwide over a matter of months. A few were established more recently and for a finite period to accomplish a specific goal; and several are ongoing and open ended, with the longest running since 2002.
We present a synthesis of the country case study findings, and develop a multisectoral collaboration model to inform further policy, action and research.
How success factors were elucidated
We anticipated that development of an underlying theoretical basis or model would be helpful in informing action and further development in relation to multisectoral collaboration.17 Our model development used a combination of methods, incorporating narrative synthesis17 and a multi-grounded theory approach.18 This combined approach goes beyond summarising findings to synthesise higher level interpretive findings and systematically develop a theoretical model.
Three main steps were employed to synthesise the country case study findings and develop a multisectoral collaboration model in this paper (supplement 1): conducting preliminary analyses of the country case study findings; synthesising higher level, interpretive findings with reference to a theoretical model; and assessing the robustness of the higher level, interpretative findings and the multisectoral collaboration model.
Conducting preliminary analyses of the country case study findings
The literature review that informed the case study methods guide identified key components of multisectoral collaboration.1419 The semi-structured questionnaire in the study series methods guide19 provided a template from which to extract, categorise, and analyse the findings from each country case study.
Synthesising higher level, interpretive findings with reference to a theoretical model
A thematic analysis was conducted to synthesise the recurring and prominent themes arising from the preliminary analysis into higher level, interpretive findings. The interpretive findings across the case studies were then analysed with reference to related best practice and a theoretical model.89121314192021
Best practices in planning, management, research, and other fields tend to follow a common logic, including experiencing a challenge or idea; defining a specific problem or question; developing evidence based solutions and innovations, and deliberating options; implementation and learning; and achieving harmonious resolution.20 This logic also seems to hold true for multisectoral collaborations, as evinced in the literature review for this study89121314192021 and additional references from non-communicable diseases,22 early childhood development,15 and nutrition.1323
This common “logic of inquiry” was elaborated by Dewey in pragmatist philosophy as a systematic way to support societal learning and advancement.20 It was applied in a “transactive rationality model” for public policy and administration,21 and in other contexts including environmental policy assessment24 and strategic crisis management.25
In this paper, we used the transactive rationality model21 to help synthesise the higher level findings across the country case studies. We selected this model because it was comparatively assessed as covering all the key components of multisectoral collaboration identified in the literature review and case study methods guide1419 (supplement 1), and also as it was explicitly framed as a theoretical “hypothesis” for best practice across a range of contexts.2021
To accommodate the specific higher level findings across the country case studies on what works in multisectoral collaboration, we adapted the reference theoretical model (supplement 1, fig 1).

{kind=link}
Assessing the robustness of the higher level, interpretative findings and the multisectoral collaboration model.
To accommodate the specific findings on multisectoral collaboration, the reference model was adapted both thematically and graphically (supplement 1, fig 1). This process continued until “theoretical saturation” was reached: that is, when the components of the new multisectoral collaboration model could accommodate all the case study findings without needing further adjustment.17 Robustness was also assessed by triangulating case study findings from different countries, and by drawing on multidisciplinary perspectives in the literature. The global steering committee and country teams reviewed the model and interpretive findings and confirmed that these reflected their experiences and lessons learnt. Expert peer reviews further confirmed the robustness of the interpretive findings and model, identifying congruence with evidence from health and other sectors, as highlighted in the discussion section below. Supplement 1 includes more details on considerations on the quality of the methods and analysis.
How multisectoral collaboration works: country case study findings
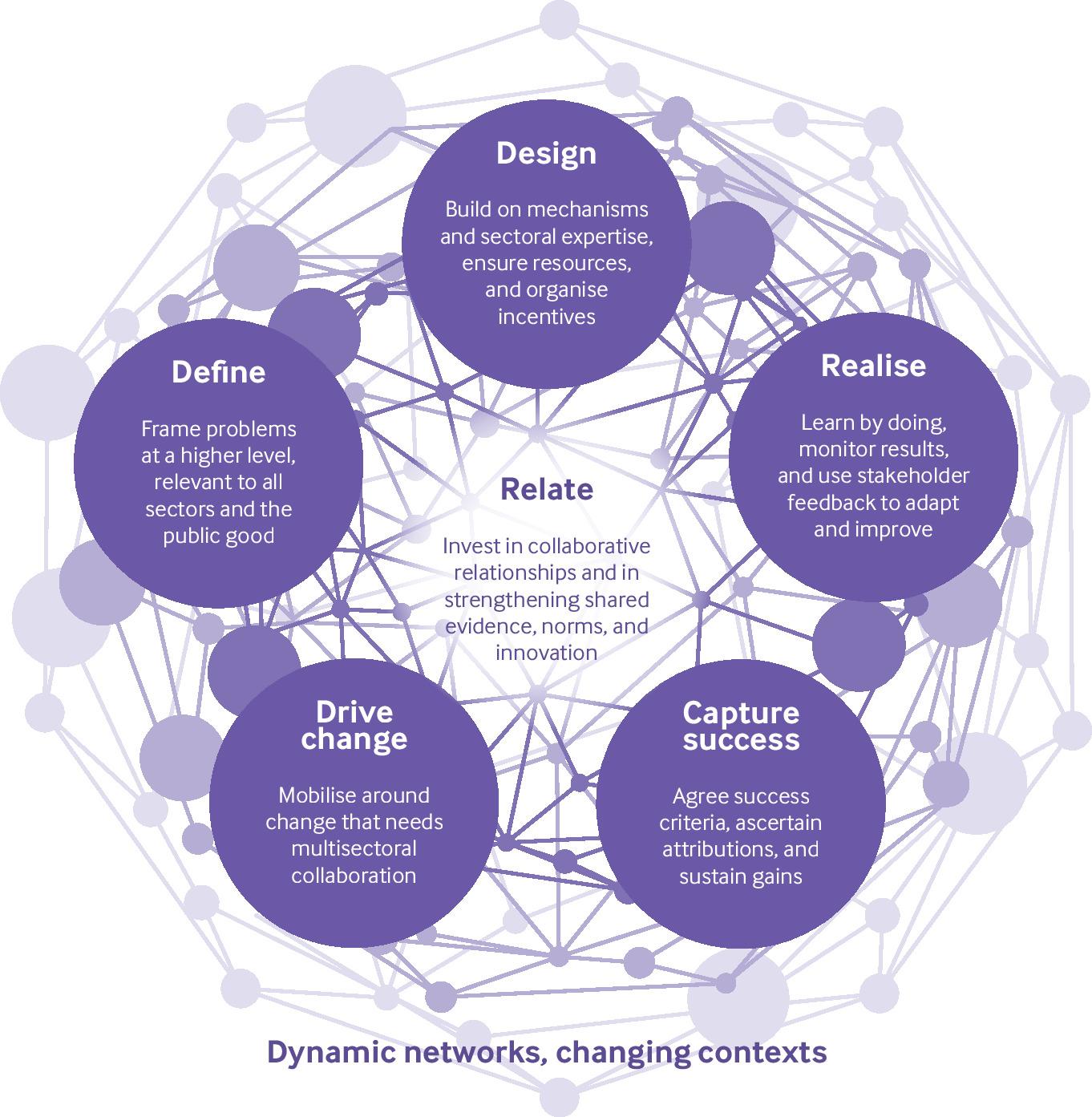
The multisectoral collaboration model (fig 1) synthesises findings across the case studies on what works in multisectoral collaboration.
In the model, “Drive change” includes a range of actors and factors that identify a need for, and initiate, a multisectoral collaboration. “Define,” “design,” and “realise” are deliberate, coordinated actions taken by sectors and stakeholders to tackle the identified need. Multisectoral collaboration is supported by the central component—“relate”—which includes the collaborative relationship as well as the integration of evidence, norms, and innovation in relation to all the different components. “Capture success” refers to how the collaborations define success and measure the results achieved. All six components in the model occur within a broader context of ongoing interactions and changing social and environmental contexts, and create a new force for collective action, learning, and change.
We elaborate on the six components of the multisectoral collaboration model, with higher level interpretive findings and illustrative country examples.
Drive change
All the multisectoral collaborations presented in this series sought to disrupt the status quo positively by instituting “business not as usual.” Across the case studies, drivers of change included a range of challenges or opportunities such as legislative, political, or socioeconomic changes, including the transition from low to middle income country status. In some cases, new data played a role by revealing a problem or gap; in others, scientific advances and innovation brought new possibilities for change. Media coverage and public attention often played an important part in instigating action, as did demands by stakeholders for harmonised policies and programmes to achieve common goals. In some countries, a high level “champion” was willing and able to kick start the collaboration and drive it forward.
Multisectoral collaboration being complex and requiring significant coordination and resources, stakeholders in all cases had to assess whether this was a better way to achieve the desired changes than reliance on action by an individual sector (box 2).
Drive change: country examples
Germany: For more than a decade, Germany has been making a concerted effort to ensure all children grow up healthy and safe.
Germany’s Early Childhood Intervention programme supports nationwide goals of providing equal opportunities for all children to develop to their full potential. The programme includes cross sectoral collaboration as a central component, particularly between the social services sector and the health sector. Efforts contribute to nationwide support for cross sectoral networks supporting early childhood intervention, such as family midwifery and nursing services, and are part of a long term focus to ensure children grow up healthy and safe, particularly for families living in difficult circumstances.
A key driver of this programme is the rising share of children living in a family receiving social benefits, despite overall prosperity and strong economic growth in the country. Burdened families often slip through the social net and are driven towards susceptibility to harmful parental behaviour and in some cases, child maltreatment. High profile cases of child neglect in Germany led the public to demand for urgent action.26
Guatemala: After more than a decade of post-war reconstruction, inequities in the levels of maternal mortality between indigenous and non-indigenous women remained stark, indicating that the health system was not adequately meeting the needs of indigenous women.
One study found that a large portion of ethnic differences in the use of institutional delivery services between indigenous and non-indigenous women was attributable to indigenous women not speaking Spanish. This study and a 2015 health systems assessment for Guatemala indicated additional challenges with availability, accessibility, and quality of services for indigenous women.
In response, Indigenous Women’s Organizations for Reproductive Health, Nutrition, and Education (ALIANMISAR) began working to tackle these problems, including the improvement of the quality and cultural acceptability of healthcare provided to indigenous women. As part of its mission, ALIANMISAR monitors a range of public health services at national, departmental, and municipal levels, in collaboration with other community based organisations, the executive and legislative sectors of the government (such as the Ministry of Health and the Ombudsman for Human Rights) and with international partners. To date, joint monitoring has contributed to important improvements in health policy and legislation, health services and infrastructure for indigenous women.27
India: India’s immunisation programme is the largest in the world, with annual cohorts of around 26.7 million infants and 30 million pregnant women. Despite steady progress, routine childhood vaccination coverage has been slow to rise, with an estimated 38% of children failing to get all basic vaccines in the first year of life in 2016.
In response to low childhood vaccination coverage, India’s Ministry of Health and Family Welfare launched Mission Indradhanush (MI) in 2014 and, based on the programme’s success, the prime minister spearheaded an ambitious plan to accelerate progress further, launching Intensified Mission Indradhanush (IMI) in districts and urban cities with persistently low immunisation coverage with the aim of reaching 90% full coverage. IMI targeted areas with higher rates of unimmunised children and immunisation dropouts. A chain of support was established from the national level through states to districts, with senior staff providing regular reviews of progress and receiving updates on progress.28
RETURN TO TEXTDefine
Once a decision to engage in multisectoral collaboration was taken, the situation was strategically defined and framed so that all sectors and stakeholders could see their role and contribution to a common goal. Attention paid to defining the problem also influenced the type of solutions sought and the measures of success; “a problem well-put is half solved.”20 In most cases the matter was framed in terms of overarching societal goals and values: for example, the human rights of indigenous communities, the agency and power of girls and women, and overcoming inequities in access to health and social services. In some countries the problem was further structured in more technical terms: for example, based on a specific health or sustainable development outcome, a service coverage gap, or the socioeconomic benefits of tackling a challenge (box 3).
Define: country examples
Chile: A survey in 2005 found that 30% of Chilean children under the age of 5 were not reaching developmental milestones, with wide gaps between rich and poor.
Drawing on these survey results, Michelle Bachelet, a paediatrician and the first female president of Chile, set a goal to ensure optimal development for all children, regardless of background, origin, and socioeconomic status, by breaking the intergenerational cycle of poverty and reducing inequity.
The resulting initiative, Chile Grows with You (Chile Crece Contigo), is a comprehensive protection system for children from the prenatal period to 4 years, taking advantage of every encounter between children and health services, and providing coordinated services across different public sectors.29
Malaysia: The government of Malaysia approved funding for a multisectoral effort to support a human papillomavirus (HPV) immunisation programme for girls and significantly reduce the incidence of cervical cancer.
Prior to this, the cervical cancer screening programme had failed to achieve screening targets. There was increased political and public interest in the matter because of media stories about the illness and death from cancer of the prime minister’s wife. There were also concerns that the vaccine could promote sexual promiscuity, be harmful to health, or not meet Islamic requirements.
Through a multisectoral effort, HPV immunisation was presented to stakeholders as a public good whose benefits outweighed its costs. Information from the telephone hotline, social media, and emails provided realistic and dynamic feedback on concerns about, and acceptance of, the vaccination programme. Key messages focused on cancer prevention and avoided sexual connotations, and the National Islamic Religious Authority issued a fatwa that the vaccine was permissible.30
South Africa: The South African government is increasingly concerned about the high rates of new HIV infections among adolescent girls and young women. It recognised that several social and structural factors underpinned this problem: poverty; unmet need for health and social services, including through educational institutions; gender inequality; and alcohol and substance abuse.
She Conquers, a three year national campaign launched by the government in June 2016, aimed to reduce the burden of HIV among women aged 15-24. The campaign moves beyond a focus on disease transmission and associated stigma to a narrative of power for adolescent girls and young women. Through multisectoral collaboration, the campaign expands a range of opportunities for adolescent girls and young women to claim their rights and decide their own futures.31
RETURN TO TEXTDesign
The solutions sought to the problems tackled by multisectoral collaboration were designed to build on existing structures, making innovations and adaptations for specific contexts. This process drew on diverse expertise from different sectors, and on feedback from stakeholders, to enhance relevance and impact. Although the design phase was often led by topic experts, the participation of stakeholders, including service users and the general public, was crucial. The feedback of service users in particular helped ensure the acceptability and perceived value of the designed solution.
Ensuring sufficient resources, for both the programme activities and the management of the multisectoral collaboration itself, was a critical concern. In some countries the coordination of multisectoral collaboration was funded from the outset. Others started with seed funding. Across all the case studies, transitioning a project into an institutionalised programme with predictable (often government) funding was a desired objective. Designing mechanisms for regular, open communication among the multisectoral collaborators was also emphasised in many of the case studies (box 4).
Design: country examples
Indonesia: A schools based iron supplementation project for adolescent girls in Indonesia provided a scalable model for anaemia reduction. The project focused on existing platforms and policy frameworks to catalyse multisectoral collaboration. Political commitment from policy makers within each sector drove the collaboration, as well as commitments from school administrators. Capacity building was needed at all levels, but investments in strengthening individual and institutional relationships across sectors helped foster collaboration. Harmonisation and collaboration on data collection, monitoring systems, as well as joint responsibility for, and ownership of, shared results, outcomes, and goals were key to engagement from all stakeholders.32
Malawi: Chipatala Cha Pa Foni (CCPF)—Chichewa for “health centre by phone”—is a free health and nutrition hotline. Launched in 2011 as a pilot project in one rural district of Malawi, it is now available nationwide to anyone with access to one of two major communications providers in Malawi. CCPF originally focused on pregnancy, antenatal, and postnatal advice, and advice for callers to seek facility care when appropriate. The programme has since expanded to include all standard health topics including water, sanitation, and hygiene; infectious diseases; and nutrition. Youth friendly services were introduced, increasing access to sexual and reproductive health information for young people. The service has the flexibility to handle emergent problems, such as cholera outbreaks. CCPF was developed iteratively by public, private, government, community, donor, and non-governmental stakeholders. CCPF will be one of the first government run nationwide health hotlines in Africa when the handover is completed in 2019.33
Sierra Leone: In May 2014, Sierra Leone reported its first Ebola case in Kailahun, a remote, marginalised, and impoverished district bordering Liberia. The district experienced one of the highest concentrations of Ebola infections during this outbreak, during which over 1600 children were orphaned and gender inequalities were exacerbated. Public health control measures put in place by the Sierra Leonean government included closing all schools, and prohibiting public congregation. While many other educational services ceased operations entirely in Kailahun, the partners involved in Getting Ready for School redesigned the project into a radio education programme called Pikin to Pikin Tok (PtPT), meaning Child to Child Talk in Krio. Over 30 children affected by the Ebola crisis, who had been young facilitators in the original programme, worked alongside PtPT’s field staff to develop the radio programmes, conduct interviews, make recordings for the radio programmes, and ensure the project remained child centred. Children involved in the programme became empowered, gaining experience as journalists and facilitators, and encouraged by listener groups to challenge adults, including parents and government representatives. They critically assessed their circumstances and how to support and protect each other, and openly discussed subjects normally regarded as taboo or difficult, such as sexual abuse.34
RETURN TO TEXTRealise
Implementation involved both doing and learning, sometimes requiring openness to change course to achieve desired results. Regular monitoring and evaluation enabled collaborations to redesign their approach when initial plans failed to achieve results, for example because programmatic barriers were not taken into account. Goals also evolved in response to unplanned effects and emerging political, health, and development priorities or events. “Realise” is therefore a learning process, in which goals and strategies are continually tested and adjusted, rather than an undeviating linear process.21
An enabling factor for collaboration in this phase, particularly when scaling up, was finding the optimal balance between national level standardisation, support, and quality assurance on one hand, and the flexibility to adapt to local needs on the other. For example, national efforts for standardisation and capacity building can support local implementation. Successful local adaptations and initiatives can inform national guidance and support and be shared or scaled up across a country.
The “realise” component is an iterative process, often needing collaboration to redefine or redesign its planned action, or a component of it. This might be because of changes in the sectors or stakeholders involved, whether individuals or organisations. As the case studies show, these changes are sometimes planned, sometimes organic, sometimes initiated by an external or internal factor, and sometimes unanticipated (box 5).
Realise: country examples
Afghanistan: Decades of war and instability had left most people without access to primary health services. In response, Afghanistan’s Basic Package of Health Services (BPHS) was introduced in 2003 at the primary care level and is an example of an innovative multisectoral collaboration implementing, scaling, and iteratively refining health service delivery in a poor, post-conflict crisis setting.
Afghanistan’s distinctive BPHS was rolled out nationwide and the delivery of BPHS services in 31 of Afghanistan’s 34 provinces was the responsibility of NGOs—through a contracting-out mechanism. The entire development of the BPHS reflected the multisectoral collaboration in its design, execution, and oversight. The programme was stewarded and implemented by the Ministry of Public Health with contributions from numerous ministries and is an example of how various stakeholders and sectors collaborate to implement a basic health structure.35
Cambodia: IDPoor is a step in Cambodia’s ongoing evolution towards a comprehensive social protection system and promoting equity. IDPoor’s origin is linked to the health sector and the introduction of the national Health Equity Fund to reduce financial barriers in access to healthcare. With assistance from development partners, the Ministry of Planning formulated a national, cross sectoral poverty identification mechanism to establish an integrated social registry to serve multiple social assistance programmes. The Ministry of Planning assumed an essential coordinating and administrative function, which was qualitatively different from the functions of technical line ministries that oversee service delivery. This cross cutting coordination function was essential to engage with a variety of sectors and stakeholders. Active involvement of relevant ministries at national and sub-national level, communal structures, NGOs, and development partners helped to build a consensus on the national guidelines and contributed to wide acceptance and use of IDPoor.36
USA: The Voices for Healthy Kids initiative launched in February 2013 as a multisectoral, multistakeholder collaboration co-created by the American Heart Association and the Robert Wood Johnson Foundation. The initiative engages, organises, and mobilises advocates to improve health in their communities by helping all children and adolescents achieve a healthy weight. This strategy is based on the premise that policy and environmental changes to improve food and physical activity settings are vital to support and enable people’s healthy weight efforts, and can also promote public health. The initiative aims to build capacity in state and local coalitions by awarding grant funding to advocates of policy changes that make healthy foods and beverages and physical activity more accessible and affordable where children and adolescents live, learn, grow, and play. Voices for Healthy Kids now convenes and coordinates more than 140 stakeholder organisations from the arenas of social justice, physical activity, nutrition, education, transportation, food access, school health, and other sectors to advance policy changes.37
RETURN TO TEXTRelate
Relationship building is central to all multisectoral collaborations. Investment in collaboration mechanisms enables open and regular communication, and facilitates the mutual understanding, trust, and accountability needed to achieve shared goals. Also important are mechanisms for all stakeholders to provide feedback throughout the process, to inform any adaptations needed.
Aligned with a collective logic of inquiry,20 multisectoral collaboration enabled diverse evidence and ideas to be tested, and encouraged innovation to tackle long standing constraints and achieve greater impact. Norms and values were interlinked with evidence as an explicit consideration in the case studies, particularly in terms of respecting positive sociocultural norms, shifting away from harmful norms, or developing and formalising new norms, for example, through standards, guidance, or official agreements.
Multisectoral collaboration is a dynamic process that occurs within wider interactions and networks and changing political, social, and environmental contexts (figure 1). Different stakeholders were more or less strongly engaged at different stages in the collaboration, depending on their roles, which were defined more or less formally. In some cases, a cross cutting coordination function—through, for example, ministries of planning or finance—was helpful to connect specific technical sectors and engage a wide range of stakeholders.
A shared sense of identity in multisectoral collaboration often developed in response to a specific context, including the ability to learn, adapt, and evolve in response to ongoing developments on the ground. Global and regional stakeholders’ contributions were also valued, especially in times of crisis and to tackle shortfalls in technical capacity or resources.
Capture success
The collaborations defined their successes across a spectrum of results (table 2). The country case studies were explicitly selected on the basis of their having described, in responding to the call for proposals, some degree of success relating broadly to health and sustainable development outcomes. The call did not predefine success but left this for applicants to describe. The diversity of interpretations, as manifested in the broad spectrum of successes reported, is a key finding in itself. It indicates that different paradigms and definitions of success are at play here, and that “there is no one truth” about what constitutes success in multisectoral collaboration.2138
Illustrative examples of a spectrum of successes in the country case studies
Nevertheless, across the case studies, three common components of success are evident: a contribution to health and sustainable development goals, including benefits perceived by service users; success within the collaboration in terms of strength of relationships, innovation, and incentives; and the scaling up and sustainability of the effort. These components highlight a common view that multisectoral action is valuable for both the means and the ends achieved.
The positive results reported by the case studies, however, need to be considered with caution. Two critical caveats are the self defined nature of the successes and the extent to which they are directly attributable to multisectoral collaboration (as a standard intervention), given the diversity of contexts and collaborations. For example, the studies did not involve comparison with populations who were not exposed to multisectoral collaboration, and few had pre-post measures. Nonetheless, based on evidence of improvements in processes and intermediary outcomes,1738 plausible assumptions can be made about the potential positive contribution made by the collaborations to health and sustainable development outcomes.
Capturing success also requires learning from failure and adaptation to challenges and change. In some cases, collaborative relationships took longer to establish because the problem was not framed in a way that all sectors and stakeholders could see the benefits of working together. This often required several iterations. The lack of engagement of key stakeholders and experts in relevant programme components reduced the ability to coordinate action and to adapt—for instance to tailor services appropriately for high risk groups and local circumstances. It also led to delays in the transition to scaling up or government ownership of programmes.
The multisectoral collaborations faced a range of ongoing or new challenges which required adaptive and innovative responses, as highlighted in “realise.” Adaptive strategies included raising additional funds to meet financial shortfalls; collaborating with media to increase public awareness of, and support for, the programme; strengthening systems to support multisectoral services; and regularly monitoring and responding constructively to changing political, demographic, and social changes, including emergency situations.
Discussion
Despite the case studies being heterogeneous in terms of their geographic, economic, social, cultural, and historical contexts, strong similarities were identified in how multisectoral collaborations were initiated, managed, and taken to scale (figure 1). These higher level findings and shared lessons allow governments and other implementers to showcase their achievements and learn from real world experiences of how multisectoral collaboration works.
The findings in this paper reflect and supplement those in the literature on multisectoral collaboration, including in the areas of education, nutrition, non-communicable diseases, and early childhood development.12152339 Our findings highlight the need to build on local resources and structures, embed quality assurance mechanisms within implementation, and ensure relevance and adaptability to context, based on service users’ experiences and perspectives. The importance of building a shared understanding of diverse stakeholder interests and contributions, investing in ongoing and open communication, and managing stakeholder relations is also evident.812222340 Finally, the need for continued commitment when pursuing coordinated action is emphasised, with the flexibility to learn from results and to make required changes along the way.4142
We provide new insights into the dynamics and effects of multisectoral collaboration. Multisectoral collaboration is not a constant configuration,23 but a dynamic and evolving process, during which stakeholders and their engagement may change across different components and contexts of the collaboration. The collaborations were intentional new modes of collective action that generated new learning and new ways of working as they evolved, to achieve transformative results. Stakeholders strategically framed a challenge or opportunity that all sectors could relate to and explicitly deliberated on the evidence, norms, and innovation needed to shape all components of the collaboration.
Collaboration across the case studies show three common elements of success: contribution to health and sustainable development goals; collaborative relationships, innovation, and incentives; and scaling up and sustainability of the effort. More studies are needed to further define success for multisectoral collaborations and strengthen measurement.
The case studies’ findings offer plausible associations for the positive results of multisectoral collaboration. These should, however, be interpreted with caution given the limitations in measurement, comparability, and attribution, especially with regards to health and development outcomes. There are challenges in demonstrating and attributing direct impacts of multisectoral collaboration as an intervention. Research and evaluation in this area is needed, however, to develop and test hypotheses about the specific factors that contribute to success, which would also inform investment and practice in this area.
Important areas for further work include the development and standardisation of indicators—such as on the perceived value of collaborative relationships and incentives, or on scaling up and sustainability. The case studies here focus on success stories: future efforts could focus on developing a systematic way to analyse failed collaborations and the lessons to be learned from them.
Specific methods and tools (box 6) could help to apply in practice the six components of the model presented here, and facilitate testing and further development.
Examples of tools and methods to support the application of the multisectoral collaboration model
The multisectoral collaboration model is based on the “logic of inquiry” as an overarching method.20 In addition, there are specific methods and tools to help operationalise the six components of the model.
1 Drive change: set agendas and mobilise a critical mass of stakeholders for change,41 ascertain whether the situation is best tackled by multisectoral collaboration, and optimise linkages across sectors and SDGs5743
2 Define: clarify the situation in a way that improves how problems are assessed, and enables stakeholders to agree on a course of action and develop a well defined project44
3 Design: build on existing mechanisms and sectoral expertise to plan programmes, set up governance for the multisectoral collaboration, and develop innovations that are relevant to stakeholders, contexts, and goals81245
4 Realise: strengthen implementation, monitoring, and evaluation as iterative and adaptive processes that facilitate learning from successes and failures, and adapt to change45
5 Relate: systematically assess and strengthen synergies between sectors,5743 manage multisectoral collaborations,812 and promote multistakeholder dialogue and deliberation46
6 Capture success: use a range of qualitative and quantitative methods to monitor and evaluate results comprehensively and promote learning from both successes and failures,1738 and formulate multisectoral collaboration as an intervention to which health and development outcomes can be attributed.47
Conclusion
This article and the country case studies offer fresh insight into how diverse sectors can intentionally shape new ways of collaborating and learning in order to transform situations and achieve shared goals. The strategies described above contributed to incentives for the sectors involved, and for the public good. The multisectoral collaboration model which has emerged from this paper is relevant for other partnerships and collaborative efforts seeking to work together better and achieve positive transformative change.
Key messages
We present a model of enabling factors for effective multisectoral collaboration, based on findings from country case studies and literature reviews:
Drive change: assess whether the desired change is best achieved by multisectoral collaboration. Drive forward collaboration by mobilising a critical mass of policy and public attention
Define: frame the problem strategically and holistically so that all sectors and stakeholders can see the benefits of collaboration and contribution to the public good
Design: create solutions that are relevant to each context, build on existing mechanisms, and leverage the strengths of diverse sectors for collective impact
Relate: ensure resources for multisectoral collaboration mechanisms, including for open communication and deliberation on evidence, norms, and innovation
Realise: learn by doing, and adapt with regular feedback. Remain open to redefining and redesigning the collaboration to ensure relevance, effectiveness, and responsiveness to change
Capture success: agree early on markers of success. Use qualitative and quantitative methods to monitor results regularly and comprehensively. Learn from failures and successes to inform action and sustain gains.
Acknowledgments
The authors thank all of the broader PMNCH Multisectoral Collaboration Study Group comprising the country teams and stakeholders who contributed to the development of the case studies within this Series, and on which this synthesis paper is based. Many colleagues contributed to the development of the methods and selection of the case studies, including Laura Frost, Beatrice Halpaap, Beth Ann Pratt, expert reviewers of eligible proposals received from the call for proposals, the United Nations H6 Working Group, and members of the PMNCH Secretariat. The authors also appreciate contributions by colleagues who reviewed and provided advice on the paper, including PC Abraham, Philipp Dorstewitz, Nicholas Furtado, Anna Rayne, and John Reeder. The paper greatly benefited from the BMJ peer reviewers, Karen Daniels, Evelyne de Leeuw, and Purnima Menon, who provided valuable direction to finalise the paper and highlighted related findings across sectors, and the BMJ editors, Paul Simpson and Emma Veitch whose guidance throughout the process was invaluable.
Footnotes
See www.bmj.com/multisectoral-collaboration for other articles in the series.
Contributors and sources: SK and WG as co-chairs of the global steering committee, together with RH the project coordinator, and inputs from all authors, conceptualised and coordinated the development of the multisectoral collaboration case studies and synthesis paper. SK, RH, WG, JMM, JFV, RB, and DH conducted the synthesis of case study findings. Other global steering committee members (TB, NC, RC, PF, SP, KR, JR, KLS, PT, YV, MNW, listed alphabetically on the byline), and lead authors and consultants on the 12 country case studies (CEA, SB, CB, SNB, LB, EAC, JD, VG, MWK, HMM, JM, IR, MLR, VS, SS, HS, DU, CNV, PY, also alphabetical on byline) reviewed the findings and contributed to all drafts of the paper, including by writing sections. PMNCH provided funding to support the country case study teams, including to convene multistakeholder dialogues and for consultancy support as required. All other authors, across a range of organisations and as members of PMNCH, contributed their time and inputs to the study processes and journal article. Shyama Kuruvilla is the guarantor of the article on behalf of the PMNCH Multisectoral Collaboration Study Group.
Competing interests: We have read and understood BMJ policy on declaration of interests and have the following interests to declare: RH is employed by PMNCH, which provided funding to support the country case study teams; CEA, SB, CB, SNB, LB, EAC, JKD, JFV, VG, HMM, JM, JM, IR, MLR, VS, SS, HS, DU, CNW, PY received funding from PMNCH for consultancy fees and related costs for undertaking the case study. All other authors contributed in kind to this collective effort with their time and inputs.
Provenance and peer review: Commissioned; externally peer reviewed.
This article is part of a series proposed by the Partnership for Maternal, Newborn, and Child Health (PMNCH) hosted by the World Health Organization and commissioned by The BMJ, which peer reviewed, edited, and made the decision to publish the article. Open access fees for the series are funded by PMNCH.
This is an Open Access article distributed under the terms of the Creative Commons Attribution IGO License (https://creativecommons.org/licenses/by-nc/3.0/igo/), which permits use, distribution, and reproduction for non-commercial purposes in any medium, provided the original work is properly cited.