Electrical injury
BMJ 2017; 357 doi: https://doi.org/10.1136/bmj.j1418 (Published 12 April 2017) Cite this as: BMJ 2017;357:j1418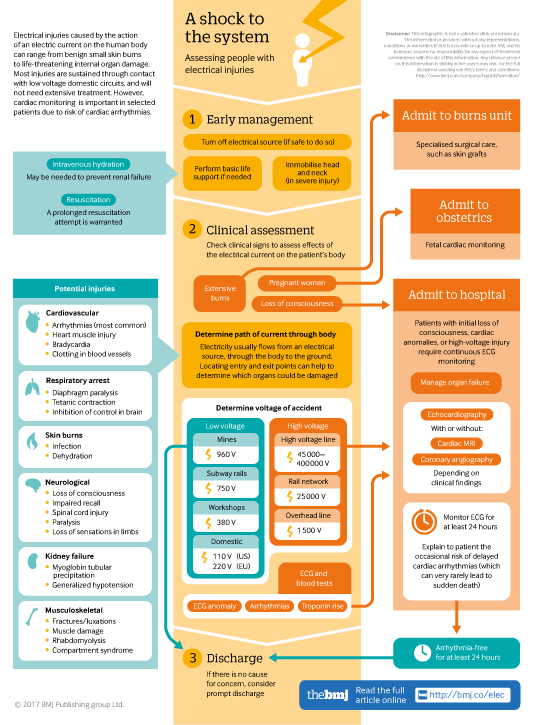
Infographic available
Click here for a visual overview of assessment for people with electrical injuries, including when to admit, and when people at low risk of complications can safely be discharged.

All rapid responses
Rapid responses are electronic comments to the editor. They enable our users to debate issues raised in articles published on bmj.com. A rapid response is first posted online. If you need the URL (web address) of an individual response, simply click on the response headline and copy the URL from the browser window. A proportion of responses will, after editing, be published online and in the print journal as letters, which are indexed in PubMed. Rapid responses are not indexed in PubMed and they are not journal articles. The BMJ reserves the right to remove responses which are being wilfully misrepresented as published articles or when it is brought to our attention that a response spreads misinformation.
From March 2022, the word limit for rapid responses will be 600 words not including references and author details. We will no longer post responses that exceed this limit.
The word limit for letters selected from posted responses remains 300 words.
On initial publication, a number of references in this Clinical Update were published with incorrect volume numbers. These references have now been amended and all references now show correct volume numbers.
Competing interests: No competing interests
Why contradict the evidence?
The authors of this article recommend a period of 24 hours cardiac monitoring after low voltage injuries as the most commonly adopted approach. However the evidence they themselves quote clearly shows that cases of low voltage injuries without any loss of consciousness, cardiac arrest or ECG abnormality, are low risk injuries and occurrence of serious arrhythmias is very low or absent. There is no evidence to support the 24hours monitoring period for this group.
Our practice based on our experience in Queen Victoria Hospital is to discharge patients with low risk injuries after the initial assessment and investigations are clear. We have not experienced any morbidity or complications requiring re-admission for these low risk group patients in the last 10 years since adopting this evidence based approach. We would encourage the authors and the readership to be guided by the evidence rather than common practice. This approach is not only cost effective it also avoids unnecessary inconvenience for both patients and hospitals.
Competing interests: None to be declared.
Nada Ibrahim; MBBS, MRCSed, PG Cert Medical Research.
Baljit Dheansa; Consultant Buns and Plastic Surgery, QVH.
Competing interests: No competing interests
We thank Drs Mahaffey and Sharma et al. for their interest in our article and appreciate the excellent commentary provided by them on the crucial importance of burn management and debridement surgery. We acknowledge that advanced surgical expertise as well as adequate fluid resuscitation to avoid renal shutdown are key and it is indeed not our intention to downplay the importance of these aspects. However, the main aim of this brief update was to provide an overview of the broad implications of an electrical injury for the generalist and to a certain extent for the lay reader and hence we did not delve into details of specific care. We have attempted to summarize the major organ-specific effects and provide an algorithm to approach management which is presented in a graphic fashion for ease. A comprehensive essay on the assessment and management of the multiple aspects of an electrical injury would require a more elaborate review and was beyond the purview of the current update.
Competing interests: No competing interests
Dear Sir/ Madam
We read with interest the article ‘Electrical Injury’ in the Clinical Update section of the BMJ (1). We note that there has been no mention of the ocular manifestations of electrical injury in this article. Electrical injury can be devastating to the visual system: in addition to direct thermocoagulative injury to the eye itself, other sequelae include cataracts, uveitis, retinal and optic nerve injury (2, 3). A patient with an electrical injury must be assessed by an ophthalmologist as some of these manifestations such as cataract and uveitis can be treated, although damage to the optic nerve and retina is often irreversible.
References
1. Electrical injury. Waldmann V, Narayanan K, Combes N, Marijon E. BMJ 2017;357:j1418
2. Al Rabiah SM, Archer DB, Millar R, Collins AD, Shepherd WF. Electrical injury of the eye. Int Ophthalmol. 1987 Oct;11(1):31-40.
3. Korn BS, Kikkawa DO. Images in clinical medicine. Ocular manifestation of electrical burn. N Engl J Med. 2014 Jan 23;370(4):e6. doi:10.1056/NEJMicm1213581.
Dr Dipak N Parmar
Dr Bhavini Kaviya
Competing interests: No competing interests
Dear Sir,
We read with interest the Cover Features article on Electrical Injury by Waldmann et al in this month's BMJ. As Plastic and Reconstructive surgeons that have dealt with spectrum of electrical burns in adult and paediatric patients, we feel the article, although wide in scope, under emphasises the potential serious surgical consequences of these injuries.
Firstly, it makes no reference to standardised emergency management of these patients as per Advanced Trauma Life Support (ATLS) and Emergency Management of Severe Burns (EMSB) precepts, crucial for the correct management of these potentially critically ill patients. This is widely practised by Emergency Department physicians, Trauma Surgeons as well as Burns and Plastic Surgeons around the world, daily. Also, quiet simply electrical injuries are burn injuries.
Secondly, only a token image (Fig 2) and part of a cartoon (Fig 3) is dedicated to the actual burn injury itself, which although small in terms of total body surface area, can be limb threatening due to the circulatory compromise in the upper and lower limbs requiring emergent escharotomies and fasciotomies under general anaesthetic. Furthermore, early tangential excision, debridement and skin grafting under general anaesthetic along with multiple dressing changes in theatre and on the ward, may be required to ensure correct healing of the burn. Importantly, modern Burns Units provide total patient care with HDU/ICU beds and staff and have identical means of invasive cardio-respiratory and circulatory support as most Level 3 Critical Care Units. They are not merely a debridement and grafting service.
Thirdly, there is no comment on fluid resuscitation and the need to maintain a high urine output of more than 1.5ml/kg/hr to abrogate the effects of rhabdomyolysis and acute kidney injury due to release of myoglobin from muscle damaged by the electrical injury. Rhabdomyolysis also affects cardiac as well as skeletal muscle and there is the potential for continuous damage to deeper tissues and bone due to the dynamic nature of the electrical burn injury.
We feel the above points add further important information that was missing from the original article,
Yours sincerely
Competing interests: No competing interests
This article, featured on the front cover of the BMJ as 'Managing Electrical Injury', hardly does what it says on the tin. Whilst the authors provide a hint of the potential complexity of the problems associated with the passage of electrical injury injury through the human body, they virtually dismiss the management as "mainly symptomatic". That is to ignore a whole host of problems which should be dealt with not by awaiting symptoms, but by the experienced clinician anticipating problems.
For example, a problem not often appreciated in the case of the "finger skin burns" illustrated at fig. 2A, is that such burns may be far more than skin only, with a deep underlying column of injured tissue which if not addressed will persist and often become infected over many weeks. Or that the 'severe foot burn' seen in fig 2B may represent the exit/entry burn of a high tension current which has also caused un-appreciated bone and muscle heating leading to very severe secondary effects such as haemolysis, rhabdomyolysis, and compartment syndrome with secondary circulatory occlusion to the extremity. These must all be dealt with ahead of symptoms by protecting renal circulation, fasciotomies and possibly massive tissue debridement.
Setting aside the fact that it is quite simply unfair on readers to suggest that the management of electrical injuries can be usefully covered in three pages, the generalist will rightly ask questions such as "when can I allow a patient to be unsupervised after suffering an electric shock?", "when might there be complications ahead?", "what is the difference between low and high tension electrical injury", and "when should I involve a specialist?". These questions are neither asked nor answered in the article and to perfectly fair to the authors, perhaps the BMJ should instead have entitled the piece as "A brief review of the possible effects of electric shock" to avoid encouraging readers into thinking they might pick up practical management points in this field.
Competing interests: No competing interests
Re: Electrical injury
I am an electric shock survivor with the misfortune of contacting two 11,500v lines in Dec. 2009. I appreciate the attempt to offer a standard post-electrocution flowchart because the EMS & emergency room care I received were very lacking, and I appreciate the other professionals offering advise from their expertise. All of this adds to the body of knowledge needed to help future patients.
In the aftermath of my incident, I became my own advocate and researched everything I could find to try and grasp the immediate and long-term effects I might be facing. My doctors were not very helpful with this part of it, citing lack of data most often.
I found the most helpful information through a survivors group, LS&ESSI Lightning Strike & Electric Shock Survivors International.
Thank you for attempting to share what you have learned and improve patient outcomes. I am happy to discuss my experiences for professional purposes in the same spirit of learning.
Competing interests: No competing interests