Intended for healthcare professionals
Rapid response to:
Practice
Practice Pointer

Exploring thoughts of suicide
BMJ 2017; 356 doi: https://doi.org/10.1136/bmj.j1128 (Published 30 March 2017) Cite this as: BMJ 2017;356:j1128
Infographic available
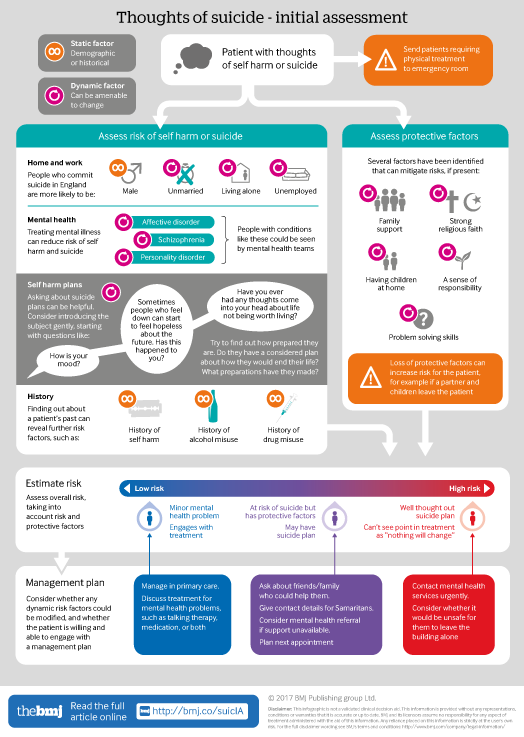
Click here for a visual overview of initial assessment for patients having suicidal thoughts. Includes risk and protective factors that need to be balanced to determine a patient's overall risk of suicide.
Rapid Response:
Exploring thoughts of suicide
The association between use of antidepressants and incidence of suicide has yielded inconsistent results and is subject to considerable controversy, with incongruity between the wide use of and the weak evidence base for the efficacy and safety of antidepressants. A meta-analysis of Sharma and colleagues [1] demonstrated the complex problems of clinical trials, unpublished studies and of meta-analysis.
The problems of FDA antidepressants' black-box warning in children and young adults are at least 15 years old [2]. In 2009 Stone et al. [3] said that the risk of suicidality associated with use of antidepressants is strongly age dependent, The risk for suicidality and suicidal behavior among adults under 25 approaches that seen in children and adolescents. In adults the risk of suicidal behaviour (completed suicide, attempted suicide, or preparatory acts) and suicidal ideation [4] is much more complex, the problems are known (poor qualitity of intransparent data, difficulties in interpreting meta-analyses, influence of pharmaceutical industry). The rapid response of Gøtzsche [5] to the paper of Sharma [1] shows the fatal consequences. Gøtzsche wrote that “researchers noted that the companies had underreported the suicide risk in their trials, and they also found that non-fatal self-harm and suicidality were seriously underreported compared to the reported suicides. There are many other reasons why the FDA seriously underreported suicides”. Gøtzsche concluded that it should be forbidden to use antidepressants in children and younger patients.
I think that clinicians need to keep in mind that suicidality has a high incidence in depressive disorders. It is time for a balanced view of the individual risk-benefit ratio under the aspects of risk factors of patients like age, previous suicide attempts or comorbidity and antidepressant treatment, especially after starting the medication, increase of dosage or co medication,. Suicide risk assessment is imperfect, indeed (6), but there are some means of deciding who benefits most or needs psychiatric intervention. Risk assessment is a part of individualized medicine. There are no alternatives to antidepressants, other psychiatric interventions and trying to enhance cooperation between GP, psychiatrist and other medical professions/organisations.
References
1) Sharma T.et al. Suicidality and aggression during antidepressant treatment: systematic review and meta-analyses based on clinical study reports. BMJ 2016;352:i652)
2) Friedman RA .Antidepressants' black-box warning--10 years later. N Engl J Med. 2014 Oct 30;371(18):1666-8. doi: 10.1056/NEJMp1408480.
3)Stone M.et al. Risk of suicidality in clinical trials of antidepressants in adults: analysis of proprietary data submitted to US Food and Drug Administration. BMJ. 2009 Aug 11;339:b2880. doi: 10.1136/bmj.b2880.
4) Stübner S et al. Suicidality as rare adverse event of antidepressant medication: a report from the AMSP multicenter drug safety surveillance project .J Clin Psychiatry 2010; 71(10):1293-307
5) BMJ 2016;352:i65
6) Sinclair LI, Authors' Reply, BMJ 2016;352:i652)
Competing interests: No competing interests