Statin use and risk of community acquired pneumonia in older people: population based case-control study
BMJ 2009; 338 doi: https://doi.org/10.1136/bmj.b2137 (Published 16 June 2009) Cite this as: BMJ 2009;338:b2137
- Sascha Dublin, assistant investigator12,
- Michael L Jackson, EIS officer1,
- Jennifer C Nelson, associate investigator13,
- Noel S Weiss, professor2,
- Eric B Larson, executive director and senior investigator145,
- Lisa A Jackson, senior investigator12
- 1Group Health Center for Health Studies, 1730 Minor Avenue, Suite 1600, Seattle WA 98101-1448, USA
- 2Department of Epidemiology, University of Washington, Seattle, WA 98195
- 3Department of Biostatistics, University of Washington
- 4Department of Medicine, University of Washington
- 5Department of Health Services, University of Washington
- Correspondence to: S Dublin dublin.s{at}ghc.org
- Accepted 31 January 2009
Abstract
Objective To test the hypothesis that hydroxymethyl glutaryl coenzyme A reductase inhibitors (statins) may decrease the risk of community acquired pneumonia.
Design Population based case-control study.
Setting Group Health, a large integrated healthcare delivery system.
Population Immunocompetent, community dwelling Group Health members aged 65 to 94; two matched controls for each case with pneumonia. Information on comorbid illnesses and functional and cognitive status, potential confounders of the association between statin use and risk of pneumonia, came from medical record review and computerised pharmacy data.
Main outcome measure Adjusted estimates of risk of pneumonia in relation to current statin use.
Results 1125 validated cases of pneumonia and 2235 matched controls were identified. Compared with controls, cases were more likely to have chronic lung and heart disease, especially severe disease, and functional or cognitive impairment. Current statin use was present in 16.1% (181/1125) of cases and 14.6% (327/2235) of controls (adjusted odds ratio 1.26, 95% confidence interval 1.01 to 1.56). Among cases admitted to hospital and matched controls, current statin use was present in 17.2% (68/395) of cases and 14.2% (112/788) of controls (adjusted odds ratio 1.61, 1.08 to 2.39, compared with non-use). In people in whom statins were indicated for secondary prevention, the adjusted odds ratio for risk of pneumonia in relation to current statin use was 1.25 (0.94 to 1.67); in those with no such indication, it was 0.81 (0.46 to 1.42).
Conclusions Statin use was not associated with decreased risk of pneumonia among immunocompetent, community dwelling older people. Findings of previous studies may reflect “healthy user” bias.
Introduction
Hydroxymethyl glutaryl coenzyme A reductase inhibitors, or statins, are widely used to prevent and treat cardiovascular disease. Interest in their potential to decrease morbidity and mortality from infection has grown recently. Such a benefit could arise from statins’ many effects on the inflammatory response and on immune function,1 2 including decreased production of inflammatory cytokines and interference with neutrophil migration and chemotaxis.3 4 5 In 2000 Ando et al published the first study examining statins and sepsis in a mouse model, reporting that pretreatment with cerivastatin improved survival and decreased production of cytokines and nitric oxide.6 In 2001 Liappis et al published the first observational study of statins and infectious outcomes in humans, reporting that among people admitted to hospital with bacteraemia, mortality was lower in those receiving statins than in others.7 Since then, many observational studies have reported associations between use of statins and decreased risk of infectious outcomes including pneumonia, bacteraemia, sepsis, and mortality from infection,8 9 10 11 12 13 14 15 16 17 18 19 20 and additional studies have reported decreased mortality associated with statin treatment in animal models of sepsis.21 22 23
However, reasons exist to be cautious in interpreting results from epidemiological studies of statins and infectious outcomes. The dramatic negative associations reported in many of these studies could reflect bias—for instance, because of underuse of statins in frail elderly people and in those with more severe comorbidity,24 25 who are at higher risk of infection. Observational studies of statins may be subject to strong “healthy user” effects, as people receiving statins tend to have less severe comorbidity and better functional status than others and are more likely to practise other healthy behaviours.24 25 26 Although previous studies attempted to adjust for comorbidity, this adjustment has often had substantial limitations, the most important of which is reliance on administrative data that may have low sensitivity for the presence of comorbid illness.27 28 Other important limitations include adjustment for only a few comorbid conditions; categorising comorbid illnesses very broadly, which may lead to inadequate adjustment29; and lack of data about functional and cognitive status. When studying the effectiveness of treatment, adjustment for functional and cognitive status may yield more valid results than controlling for comorbidity alone.24 29 In one study of people admitted to hospital for pneumonia, the initial association between statin use and decreased risk of adverse outcomes (mortality or admission to intensive care unit) became null with more thorough adjustment, particularly for factors typically not available in administrative databases such as measures of functional status and health behaviours.25
We had the opportunity to use data from a study of community acquired pneumonia to examine the potential benefit of statins in infection. Together with influenza, pneumonia is the seventh leading cause of death in people aged 65 and older,30 and more than 900 000 cases of community acquired pneumonia occur each year among older people in the United States.31 Pneumonia provides an excellent model for studying healthy user bias, because increased risk is associated with comorbid illness and functional and cognitive impairment,31 32 33 34 35 characteristics that are also associated with decreased use of preventive drugs such as statins.24 36 37 Two previous observational studies examined the association between statin use and risk of pneumonia in large administrative databases and reported a 30% to 50% lower risk of pneumonia in statin users compared with non-users.10 11
We analysed data from a case-control study in immunocompetent, community dwelling older people to test the hypothesis that current use of statins is associated with decreased risk of community acquired pneumonia. Our goal was to examine whether statin use is associated with decreased risk of pneumonia in older people after control for carefully defined health and functional status, identified through detailed review of medical records.
Methods
Setting
The study took place at Group Health, a large, integrated healthcare delivery system in Washington State.
Study design and population
These analyses used data from a previous population based case-control study of risk of pneumonia in relation to influenza vaccination among immunocompetent, community dwelling older people.34 The source population was community dwelling Group Health members aged 65 to 94 with at least two years of continuous membership as of 1 September 2000, 2001, or 2002. We excluded people who were immunocompromised, defined as having a history of serious cancer, recent treatment for cancer (receiving radiation or chemotherapy in the previous three months), or chronic renal failure (creatinine >3 mg/dl, dialysis, or a diagnosis of chronic kidney disease); or receiving prescriptions for certain immunosuppressive drugs (methotrexate, azathioprine, ciclosporin, or muromonab-CD3) or drugs used to treat HIV infection during the two years before 1 September. We determined eligibility for the study from computerised pharmacy, laboratory, and encounter data and confirmed it by review of medical records.
Identification of cases and controls
The methods used to identify and validate pneumonia cases have been described in detail.38 Briefly, we identified presumptive cases by using ICD-9 (international classification of diseases, ninth revision) codes from inpatient and outpatient encounters (pneumonia codes: 480 to 487.0 or 507.0) and validated them through review of chest radiograph reports and hospital records. We excluded cases of nosocomial pneumonia or massive aspiration. Because the original study focused on influenza vaccination and pneumonia risk, it included pneumonia cases occurring from 1 September until the end of the influenza season in each study year (2000-1, 2001-2, and 2002-3). For people with multiple episodes of pneumonia, we included only the first episode. Figure 1⇓ shows the flow of potential participants through the study.
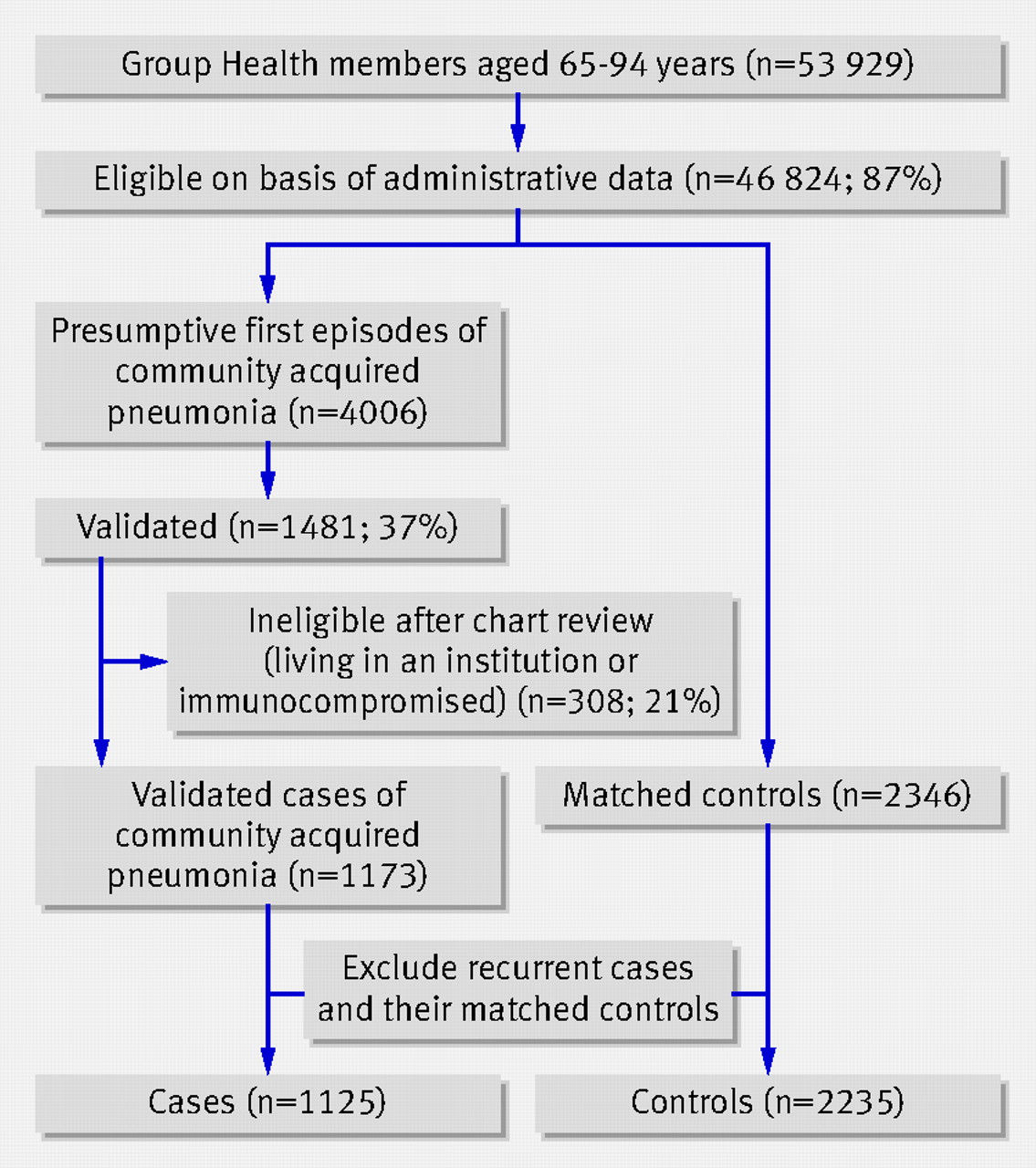
Fig 1 Selection of cases and controls for inclusion in study
{kind=link}
We selected two controls for each case from the eligible source population, matched on age (±1 year), sex, calendar year, and duration of pneumonia-free follow-up (incidence density sampling). Pneumonia cases were not eligible to be subsequently resampled as controls.
Power calculations indicated that, for a sample size of 1125 cases and 2235 controls, we would have at least 85% power to detect odds ratios of 0.67 or more extreme if the prevalence of statin use was 10% and at least 95% power if the prevalence was 15% or greater.
Data collection and variable creation
Trained abstractors reviewed medical records to verify eligibility and to collect information about comorbid illnesses, lifestyle and demographic factors, healthcare utilisation, and functional and cognitive status. Medical records were reviewed in the same way for cases and controls. The medical record review focused on the two year period before 1 September of each year (defined hereafter as the baseline period) and included detailed assessment of the presence and severity of various health conditions, focusing on those hypothesised to be associated with risk of pneumonia. Measures of functional status included documentation in the chart of need for assistance with ambulation or bathing, use of home health services, and whether a person was ever described as frail by medical personnel. The measure of cognitive status was the presence of a physician’s diagnosis of dementia in the chart. Information on previous cholesterol concentrations came from computerised laboratory data.
Information about drug use came from a computerised pharmacy database. In previous studies, 98% of Group Health members in this age group have reported filling all or almost all of their prescriptions at Group Health pharmacies.39 We obtained data about prescriptions for a wide variety of drugs used to treat chronic heart and lung disease, as these conditions are associated with increased risk of pneumonia and we hypothesised that use of these drugs might be an indicator for severity of heart or lung disease. We also obtained information about other drugs hypothesised to influence risk of pneumonia, such as H2 receptor blockers and proton pump inhibitors.
Definition of current statin use
To determine whether people were current users of statins at the time of diagnosis of pneumonia, we defined an “index date” for each case as the date of diagnosis of pneumonia, which was defined as the date of the first positive chest radiograph or, for cases admitted to hospital with no radiology report available, the date of admission. Controls were assigned the same index date as their matched case. We defined current statin use as receipt of least two prescriptions for a statin within the 180 days before the index date.
Statistical analyses
To examine characteristics associated with pneumonia, we calculated proportions for categorical variables and medians and interquartile ranges for continuous variables according to pneumonia status. We did similar analyses to identify characteristics associated with current statin use among control participants. We then used conditional logistic regression to estimate the risk of pneumonia associated with current statin use, with robust standard errors to account for possible repeated sampling of controls. Partially adjusted models included only the matching variables (age, sex, and calendar year), and fully adjusted multivariable models also included comorbid illnesses, lifestyle and demographic characteristics, and functional and cognitive status. We selected covariates for inclusion in the final models as follows. We generated a list of potential confounding factors on the basis of clinical plausibility and review of the literature. We examined these in descriptive analyses and selected for our final models those that seemed to be substantially associated with either risk of pneumonia or use of statin (no set P value was needed, as we thought that this was overly arbitrary). Certain characteristics were not included in the final models because their prevalence in the population was extremely low. For analyses in which admission to hospital for community acquired pneumonia was the outcome, we selected confounders for inclusion if they were associated with statin use or admission to hospital for pneumonia. Missing values were a concern for only two variables included in the final models—smoking status and cholesterol—and we treated them as a separate category, using indicator variables. We used SAS version 9.1 for analyses.
Sensitivity analyses
To assess whether our definition of statin use affected the results, we did two additional analyses. Firstly, we repeated the primary analysis with a stricter definition of non-use, in which we excluded “possible” statin users from the non-use (referent) group but included them in the model as a separate category. We defined “possible users” as those who had at least one prescription for a statin in the year before the index date but did not meet the definition of current statin use. Secondly, we repeated the primary analysis with current statin users redefined as people whose most recent prescription for a statin would be expected to last at least until the index date, on the basis of the days’ supply dispensed and assuming 80% compliance. To assess the impact of covariate selection on our results, we created a parsimonious model that adjusted only for matching factors and those covariates which, when included in models, altered the statin-pneumonia odds ratio by 10% or more. In addition, we repeated our primary analyses in subgroups defined by the presence of indications for statin use. The “secondary prevention” subgroup included people with congestive heart failure, stroke, diabetes, history of myocardial infarction or coronary revascularisation, or other heart disease, and the “primary prevention” subgroup included people lacking these conditions. Because of the matched study design, only cases and controls concordant for primary versus secondary prevention could be included in these analyses.
Finally, we attempted to examine the impact of several aspects of our study design, including validation of pneumonia cases and restriction of the cohort, in analyses using only administrative and pharmacy data. Within the entire source cohort, we identified presumptive pneumonia cases from ICD-9 codes and did Cox proportional hazards regression modelling to estimate the association between current statin use and risk of pneumonia. We did crude analyses without any restriction or adjustment. We then did analyses including both restriction and adjustment. Using administrative and pharmacy data, we excluded people with chronic renal disease, cancer or cancer treatment, moderate or severe liver disease, hospice care, nursing home residence, or use of immunosuppressive drugs. We adjusted for covariates including age, sex, number of outpatient visits, drug use (for example, bronchodilators, furosemide, inhaled or oral corticosteroids), and comorbid illnesses.40 We attempted to mirror the primary analyses used in the case-control study as closely as possible given the limitations of the administrative and pharmacy data.
Results
Study population
We found 53 929 people aged 65 to 94 who were Group Health members as of 1 September in one of the study years, including 46 824 (87%) who met eligibility criteria on the basis of electronic data sources and thus made up the source cohorts. Within this group, 4006 first episodes of presumptive community acquired pneumonia occurred during follow-up, of which 1481 (37%) were validated. Of these, 308 (21%) were ineligible on the basis of chart review, leaving 1173 cases, for whom we selected 2346 matched controls. For these analyses, we did not allow participants to be included as a case in more than one year, thus excluding another 48 cases and their matched controls. Thus, the population for these analyses consisted of 1125 validated pneumonia cases and 2235 matched controls. Of the 1125 cases, 395 (35.1%) were admitted to hospital, and the remainder were treated as outpatients; 62 (5.5%) cases died within 30 days of their index date.
Characteristics of pneumonia cases and controls
Compared with controls, people with pneumonia were more likely to have chronic lung and heart disease and to have more severe lung and heart disease as indicated by several measures of severity (table 1⇓). For instance, cases were more likely than controls to be receiving home oxygen, chronic oral corticosteroids, or furosemide and, among those with congestive heart failure, to have had their ejection fraction measured. In addition, cases were more likely to be current smokers and to have evidence of functional or cognitive impairment, such as needing assistance with bathing or ambulation.
Characteristics of pneumonia cases and controls. Values are numbers (percentages) unless stated otherwise
Characteristics associated with current statin use
Among our study participants, 636 had received a total of 6176 prescriptions for a statin in the 12 months before the index date. The most commonly used drug was simvastatin, which accounted for 76% (4699/6176) of prescriptions, followed by lovastatin (19%; 1194/6176) and atorvastatin (3.5%; 216/6176). Pravastatin and fluvastatin were rarely used.
Among controls, statin use was more common among men than among women (table 2⇓). It was strongly associated with heart disease and with cardiovascular risk factors, including diabetes mellitus and treated hypertension. Statin users showed healthier behaviour than non-users in several regards: they were less likely to be current smokers and more likely to have received influenza or pneumococcal vaccine. In addition, overall health status was better among current statin users, who were less likely to need assistance with bathing or ambulation than non-users and less likely to have been described as “frail” in the chart.
Characteristics associated with statin use among controls. Values are numbers (percentages) unless stated otherwise
Association between current statin use and pneumonia risk
We found no association between current statin use and decreased risk of pneumonia in models with minimal or full adjustment (table 3⇓). The fully adjusted odds ratio for pneumonia in statin users, compared with non-users, was 1.26 (95% confidence interval 1.01 to 1.56) (table 4⇓). In models limited to pneumonia cases admitted to hospital and their matched controls, statin users were at higher risk than non-users. Current statin use was seen in 17.2% (68/395) of admitted cases and 14.2% (112/788) of their matched controls, and the adjusted odds ratio was 1.61 (1.08 to 2.39) (table 5⇓).
Current statin use and risk of community acquired pneumonia. Values are numbers (percentages) unless stated otherwise
Results of multivariable regression model for statin use and risk of community acquired pneumonia*
Results of multivariable regression model for statin use and risk of admission to hospital for community acquired pneumonia*
Sensitivity analyses
We got similar results from a parsimonious model adjusting only for matching factors and those covariates that altered the statin-pneumonia odds ratio by 10% or more (chronic obstructive pulmonary disease, hospital admission for chronic obstructive pulmonary disease, and other heart disease): the adjusted odds ratio for current statin use was 1.12 (0.93 to 1.36) (fig 2⇓).

Fig 2 Risk estimates for association between statin use and community acquired pneumonia: sensitivity analyses. Current statin use defined as at least two prescriptions for statin within 180 days before index date; pneumonia outcomes defined from ICD-9 codes for cohort analyses and validated by medical record review for all other analyses. NA=not applicable. *Adjusted for matching variables, history of chronic obstructive pulmonary disease (with or without hospital admission), and other heart disease. †Possible statin use defined as receipt of at least one prescription for statin in previous year but not meeting criteria for current use; possible users removed from non-user (referent) group but included in model as separate category. ‡Indication for statin for secondary prevention defined as presence of at least one of congestive heart failure, stroke, diabetes, history of myocardial infarction or coronary revascularisation, or other heart disease. §On basis of days’ supply of most recent filled prescription. ¶All restrictions and adjustments based on administrative and pharmacy data
{kind=link}
Analyses that excluded “possible” statin users (those with at least one prescription for a statin in the previous year but not meeting criteria for current use) from the non-user group also yielded similar results: for all community acquired pneumonia the adjusted odds ratio comparing current statin users with non-users 1.22 (0.98 to 1.51), and for community acquired pneumonia requiring hospital admission it was 1.61 (1.08 to 2.41). In analyses in which current statin use was defined on the basis of the days’ supply of the last prescription before the index date, results were again similar: for all community acquired pneumonia the adjusted odds ratio for current statin use was 1.15 (0.94 to 1.42) compared with non-use, and for community acquired pneumonia requiring hospital admission it was 1.44 (0.98 to 2.13).
We repeated our primary analyses in subgroups stratified by indication for statin use (grouped broadly as primary versus secondary prevention). Because of the matched study design, about 25% (273/1125) of cases and 50% (1082/2235) of controls had to be excluded because they were discordant for this characteristic. In the primary prevention subgroup, current statin use was seen in 4.4% (16/360) of pneumonia cases and 5.4% (27/504) of controls, and the adjusted odds ratio was 0.81 (0.46 to 1.42). In the secondary prevention subgroup, statins were used by 25.2% (124/492) of cases and 25.7% (167/649) of controls, and the adjusted odds ratio was 1.25 (0.94 to 1.67).
Other sensitivity analyses included the entire source cohort and defined pneumonia on the basis of ICD-9 codes (without validation). The crude analyses included 5021 events, of which 720 (14%) occurred in statin users, and yielded a crude odds ratio of 1.12 (1.03 to 1.21) for the association between current statin use and risk of pneumonia. Further analyses that restricted the source cohort and adjusted for covariates on the basis of administrative and pharmacy data included 3712 events, 537 (14%) of which occurred in statin users, and the corresponding risk estimate was 0.99 (0.90 to 1.09.).
Discussion
In this population based case-control study of immunocompetent, community dwelling older people, we found no decreased risk of pneumonia associated with current use of statins. For all cases of community acquired pneumonia, if anything a slight increase in risk was associated with current statin use (adjusted odds ratio 1.26, 95% confidence interval 1.01 to 1.56, compared with non-use). For pneumonia leading to admission to hospital, the increased risk was greater still (adjusted odds ratio 1.61, 1.08 to 2.39).
Study strengths and limitations
Strengths of our study include extensive efforts to minimise confounding, including both “healthy user” bias and confounding by indication, and the validation of all pneumonia outcomes. Firstly, we used restriction to focus on relatively healthy, community dwelling elderly people, a group in which less potential for bias may exist compared with an unselected older population including residents in nursing homes and people with serious or terminal illness. More specifically, we excluded immunocompromised people, who may be at higher risk of pneumonia but less likely to receive statin treatment. Our use of medical record review as well as pharmacy data to determine eligibility criteria, comorbid illness, and functional and cognitive status probably resulted in more accurate ascertainment of confounding factors, including measures of severity of comorbid illnesses. We reviewed and validated all cases of pneumonia, specifically excluding nosocomial pneumonia, which may reduce confounding from health differences between statin users and non-users.
Our study also has some limitations. Information on exposure came from computerised pharmacy data, so misclassification of exposure is possible if participants filled prescriptions outside of Group Health or filled a prescription but failed to take the drug. However, we note that in previous studies, 98% of Group Health members in this age group have reported filling all or almost all prescriptions at Group Health pharmacies.39 Consistent with the demographics of Washington State, Group Health members are predominantly white, so our findings may not be generalisable to other racial and ethnic groups. Because of our focus on community acquired pneumonia in a relatively healthy population, we cannot answer the question of whether statins may be beneficial in a sicker, more frail elderly population, such as nursing home residents or immunosuppressed people.
Comparison with previous studies
Our results differ from the findings of two previous studies that examined use of statins and risk of pneumonia. In a case-control study limited to people with diabetes, van den Garde et al found a reduced risk in current statin users (adjusted odds ratio 0.49, 0.35 to 0.69, compared with non-users).10 Schlienger et al did a case-control study within the general practice research database and found an association of statin use with decreased risk of pneumonia (adjusted odds ratio 0.71, 0.56 to 0.89).11 The association was strongest for fatal pneumonia (adjusted odds ratio 0.47, 0.25 to 0.88) and was not significant for pneumonia treated in the outpatient setting (adjusted odds ratio 0.84, 0.61 to 1.17). Several methodological differences exist between these studies and ours that may explain the divergent results. Whereas we extensively reviewed medical records, both the previous studies relied on large electronic databases, which may have limited sensitivity for important comorbid conditions. Neither previous study excluded nursing home residents, a group that may be particularly frail and susceptible to pneumonia yet have reduced likelihood of receiving a statin. Neither previous study identified nor adjusted for measures of functional or cognitive status. All of these aspects may have contributed to healthy user bias in these studies. Notably, Majumdar et al studied patients admitted to hospital for pneumonia and found that analyses adjusting only for typical administrative variables found a decreased risk of mortality or admission to an intensive care unit among statin users compared with non-users, whereas analyses with more thorough adjustment, including for functional status, showed no association, and their final risk estimate suggested increased risk among current statin users.25 These findings are consistent with ours and support the idea that healthy user bias may help to explain why our results differ from those of van de Garde and Schlienger.10 11
Possible biological mechanisms
A biological basis could exist for the increased risks that we and Majumdar et al found among current statin users.25 By altering the immune response, statins may impair host defence mechanisms, leading to the spread of infection. One study in which mice were inoculated with Klebsiella pneumoniae found increased bacterial growth and enhanced systemic dissemination of bacteria in statin treated mice.4 Alternatively, this apparent increased risk could be due to chance or it could reflect residual confounding by indication, particularly in the hospital admission outcome, as statin use is associated with conditions such as diabetes and congestive heart failure that may influence the decision to admit patients with pneumonia.
Conclusions and policy implications
Our results suggest that caution is warranted in attributing benefits to statin use that may instead reflect unmeasured differences between users and non-users. Although we examined risk of developing community acquired pneumonia, rather than outcomes after pneumonia or sepsis, our findings may be relevant to that area of research as well, suggesting that great care should be taken in interpreting the findings of studies of sepsis and infectious mortality, in which similar patterns of confounding may exist. That is, as is true for pneumonia, some groups at particularly high risk for sepsis and infectious mortality—such as nursing home residents, people with serious cancer or chronic renal disease, or immunosuppressed people—may be less likely to receive statin treatment, an example of the healthy user effect.
On the basis of previous observational studies, some investigators have called for randomised trials of statins for prevention or treatment of sepsis and lung disease and have suggested that statins could be beneficial in cases of pandemic influenza.9 10 14 15 41 42 43 44 According to Clinicaltrials.gov, five randomised clinical trials of statins in the setting of sepsis are currently under way,45 46 47 48 49 with numbers of participants ranging from 20 to 250, and an additional randomised trial is examining ventilator associated pneumonia.50 We believe that investing additional resources in trials may be premature, given the weaknesses of the observational research in this area and resulting uncertainties about the true benefits of statin use. Instead, an individual level meta-analysis of existing data from randomised placebo controlled trials of statins might be useful to examine infectious outcomes such as pneumonia or sepsis.
Our findings highlight some of the limitations of large administrative databases in studying some unanticipated effects of commonly used drugs such as the statins. These results are particularly relevant, as the use of administrative data sources for research purposes continues to increase and widen in scope. For example, the Sentinel Initiative, which was launched by the US Food and Drug Administration in May 2008, aims to monitor safety of medical products by combining existing data sources such as administrative medical claims data to support research on a population of 100 million people by 2012.51 Our work suggests that policy makers as well as researchers should carefully consider the limitations of such data, particularly regarding the ability to characterise the population exposed and not exposed to certain drugs. More work needs to be done to learn how to improve the content of large administrative databases by incorporating richer and more detailed data, including clinical data, which should become increasingly feasible with the growing use of electronic medical records. Such detailed data may be critical to obtaining valid results in studies of some drug-disease associations.
What is already known on this topic
Statins have diverse anti-inflammatory and immunomodulatory effects
Observational studies have reported associations of statin use with decreased infectious morbidity and mortality, including decreased risk of pneumonia
Statin use is less common in people with certain severe comorbid illnesses, frailty, and functional or cognitive impairment, so previous studies’ findings may be due to “healthy user” bias
What this study adds
Statin use does not decrease risk of pneumonia among healthy, community dwelling older people (odds ratio 1.26, 95% confidence interval 1.01 to 1.56)
Augmenting large administrative databases with richer and more detailed clinical data may be critical to obtaining valid results in studies of some drug-disease associations
Notes
Cite this as: BMJ 2009;338:b2137
Footnotes
We appreciate the assistance of Rod Walker, who did additional statistical analyses.
Contributors: SD, MLJ, JCN, NSW, and LAJ were involved in study conception and design and in acquisition of data. SD and MLJ were responsible for data analysis. All authors were involved in interpretation of results and in drafting or revising the manuscript. All authors approved the final submitted version. SD is the guarantor.
Funding: SD was funded by a Paul Beeson Career Development Award from the National Institute on Aging (grant K23AG028954). The Beeson award is also supported by the Hartford and Starr Foundations and Atlantic Philanthropies. Group Health Center for Health Studies internal funds covered the data collection and analysis. The sponsors played no role in study design; the collection, analysis or interpretation of data; the writing of the report; or in the decision to submit the manuscript for publication.
Competing interests: JCN has done consulting work for GlaxoSmithKline.
Ethical approval: All study procedures were approved by the Group Health Human Subjects Review Committee.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.