Practising medicine when you have colour blindness
BMJ 2004; 329 doi: https://doi.org/10.1136/bmj.329.7468.s126 (Published 25 September 2004) Cite this as: BMJ 2004;329:s126
Abstract
Tony Spalding explains the different types of colour blindness (or to use the correct term, congenital colour vision deficiency) and outlines how doctors and medical students with these deficiencies can overcome or avoid any difficulties
Inherited (congenital) colour vision deficiency (CCVD), also called Daltonism and colour blindness, is the commonest human inherited defect. There are two outstanding features of practical importance for people who have it: when viewing colour, they sometimes fail to see what other people see quite plainly, and they can be unaware of the occasions when this occurs. This leads to the common but incorrect attitude that this condition causes few problems.
The medical profession in the United Kingdom, like many other countries, has no agreed policy for identifying and advising students and doctors with CCVD, so that those with the condition are unlikely to receive any formal advice. Different specialties make different demands on the ability of the doctor to see colour so that students and doctors should take it into account in making a choice of career (see below).
Colour is a valuable guide to the presence of health and disease. All doctors make errors but the kind caused by CCVD should be largely avoidable if you are aware of how and when they are likely to occur. The red of fresh blood is one example. Its observation can be critical to outcome for the patient, and it is known that doctors with CCVD can sometimes fail to see it.12
Background information
Classification and prevalence
The classification (table 13) is based on abnormal or missing pigments in the retina. In most Western countries the prevalence is one in 12 for men and one in 200 for women. In the UK and the US medical professions it is similar to that of the whole population. There were approximately 5800 doctors with CCVD in all forms of practice in the United Kingdom in 1994.4⇓

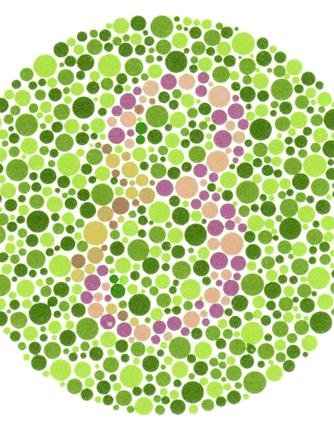
Ishihara test. Images from tests for colour blindness by Dr Shinobu Ishihara
The deficiency and its effects
The colour confusion is across most of the spectrum: red, pink, yellow, green, orange, blue, violet, purple, brown, and grey are all affected. The two main forms have very similar effects, but protans (red deficiency) see red as darker than deutans (green deficiency) (table 1). The defect can be mild, moderate, or severe and the effects vary with the severity.
The effects are on the discrimination, naming, and matching of colours. For example, “Is that blood?” and “Is that patient pale?” are questions that can be difficult to answer. Dappled backgrounds, light and dark colours, and poor illumination can make it more difficult.
Testing
The Ishihara test (see pictures) identifies all those with the two main forms and also helps to distinguish between them, but it does not test for severity. Other tests, for example the Farnsworth D15 test, are needed for this.3 Computer graphic methods are also being developed.
Attitudes to university admission
In Western countries you are unlikely to be screened for CCVD or given advice about it, and it is not a bar to studying medicine. In some Eastern countries, admission to medical school may not be allowed if the deficiency is severe. Japan has recently relaxed such rules.
The difficulties of doctors in general practice and specialties
Table 2 gives a list of some of the difficult areas reported by 37 general practitioners and three specialists with CCVD.⇓

{kind=link}
{kind=link}
Other studies have shown that general practitioners make errors in testing for blood glucose and observing samples of stool and vomit12 for the presence of fresh blood. Specialists make errors in microscopy and ophthalmology, and studies for endoscopy showed conflicting results.
Individual doctors have told me the specialties that they would avoid. These include pathology, surgery, anaesthesia, and dermatology. Definitive statements have not been made about these by the specialists themselves (see box for other comments).
Doctors' comments
This is what some doctors with CCVD say.56
Difficulties are overcome by awareness, self training, and effort (deutan physician)
I often ask my colleagues for advice, especially over babies with rashes and fevers etc, and the chance of a red ear or throat. I feel very vulnerable at the end of a busy surgery. I believe there are times when patients describe red rashes and I cannot see them and nurses point to the invisible dots (deutan general practitioner)
You do not necessarily know when you have problems—others point them out (deutan general practitioner)
In my ophthalmology training I will probably choose a subspecialty that does not concentrate on fundal examination (protan ophthalmologist)
The performance of general practitioners can be affected by the fact that they sometimes work alone and sometimes in poor illumination.
Choice of career
There is no reason why you should not study medicine but you should give thought to the specialty you enter. General practice and pathology, for example, make definite demands on the sense of colour, but psychiatry and radiology do so much less. You should discuss frankly with an experienced specialist the difficulties that might occur in a specialty before making a decision. Awareness of your limitations will be your major way of avoiding difficulties, but it may not overcome all of them. Sometimes you will need to avoid the situation in which they arise.
Specific advice
Find out the type and severity of your deficiency. Do not rely on the Ishihara test alone. High Street optometrists, ophthalmologists, and university departments of optometry can do the tests.
Know the colours you can confuse and realise that they are across most of the spectrum.
If you have a severe deficiency, realise that you are incapable of discriminating between red and green even when they are pure hues if the object you are viewing subtends an angle of less than two degrees at the eye. Distant and small objects of these colours can therefore present a special problem to you. (It is a useful guide to know that the terminal segment of the thumb when held at arm's length subtends an angle of two degrees at the eye).⇓
Arrange for good illumination.
Use numerical readouts for clinical tests if they cause difficulty (for example, Glucostix, Bayer Diagnostics).
Be open with medical colleagues about your problem and particularly your teachers. Turn to them when you need help, so they will learn to understand and to help you.
Place greater reliance on other sources of information—for example, the history and body language. But be aware that an isolated sign, which is sometimes a colour, can be critical in making a diagnosis or in deciding on a course of action for a patient.

The Ishihara test doesn't test for severity of colour blindness
{kind=link}
Key points
You will not always be aware of what you fail to see.
Find out the degree type of severity of your deficiency and its effects on your work as a student and doctor
Be open with teachers and colleagues about it
Take advice about your choice of career
Further information
General—www.medicdirect.co.uk/diseases/defaultihtm?pid=13768&step=4
Reviews—www.mcintyre.plus/cvd/reviews.htm
Associations concerned with colour vision: International Colour Vision Society; membership information: anne.kurtenbach{at}uni-tueringe.de
Applied Vision Association UK—www.dmu.ac.uk/ava
A book: Effects of Colour Blindness. Spalding and Arden, 2001. ISBN:0953995607 £14.00. Obtainable from: Optometry Today Bookshop, email fiona{at}optometry.co.uk