Randomised controlled trial of atraumatic versus standard needles for diagnostic lumbar puncture
BMJ 2000; 321 doi: https://doi.org/10.1136/bmj.321.7267.986 (Published 21 October 2000) Cite this as: BMJ 2000;321:986
- S Rachel Thomas, lecturera,
- D R S Jamieson, consultantb,
- Keith W Muir, locum consultant (k.muir{at}clinmed.gla.ac.uk)a
- a Department of Neurology, Institute of Neurological Sciences, Southern General Hospital, Glasgow G51 4TF
- b Department of Neurology, Leeds General Infirmary, Leeds LS1 3EX
- Correspondence to: K W Muir
- Accepted 17 July 2000
Abstract
Objective: To compare the ease of use of atraumatic needles with standard needles for diagnostic lumbar puncture and the incidence of headache after their use.
Design: Double blind, randomised controlled trial.
Setting: Investigation ward of a neurology unit in a university hospital.
Participants: 116 patients requiring elective diagnostic lumbar puncture.
Interventions: Standardised protocol for lumbar puncture with 20 gauge atraumatic or standard needles.
Outcome measures: The primary end point was intention to treat analysis of incidence of moderate to severe headache, assessed at one week by telephone interview. Secondary end points were incidence of headache at one week analysed by needle type, ease of use by operator according to a visual analogue scale, incidence of backache, and failure rate of puncture.
Results: Valid outcome data were available for 97 of 101 patients randomised. Baseline characteristics were matched except for higher body mass index in the standard needle group. By an intention to treat analysis the absolute risk of moderate to severe headache with atraumatic needles was reduced by 26% (95% confidence interval 6% to 45%) compared with standard needles, but there was a non-significantly greater absolute risk of multiple attempts at lumbar puncture (14%, −4% to 32%). Higher body mass index was associated with an increased failure rate with atraumatic needles, but the reduced incidence of headache was maintained. The need for medical interventions was reduced by 20% (1% to 40%).
Conclusions: Atraumatic needles significantly reduced the incidence of moderate to severe headache and the need for medical interventions after diagnostic lumbar punctures, but they were associated with a higher failure rate than standard needles.
Editorial by Serpell and Rawal
Introduction
Headache due to a reduced volume of cerebrospinal fluid and reduced pressure complicates a substantial proportion of lumbar punctures.1-3 In the 1920s Greene hypothesised that complications could be reduced by using a smaller, tapered needle with a blunt tip, which would separate rather than cut dural fibres and thus reduce fluid leakage. 4 5 Atraumatic (“blunt”) needles have been in clinical use since the 1950s, principally in anaesthetic practice, where there is substantial evidence of a reduced incidence of headache and other neurological complications after their use.6
Spinal anaesthesia and myelography differ from diagnostic lumbar puncture because smaller gauge needles are used, smaller volumes of cerebrospinal fluid are removed, and other fluids can be introduced. The incidence of headache after spinal anaesthesia is typically half that after diagnostic lumbar puncture. 2 6 Despite evidence that relevant physical characteristics of atraumatic needles, such as flow rates, are comparable to those of standard needles,6 there are limited data on their benefit in diagnostic lumbar puncture. Also, there is a perception that atraumatic needles are more difficult to use than standard needles. Previous studies of diagnostic lumbar puncture have potentially been confounded by comparing different needle gauges, failing to define the operators' previous experience or the length of follow up, and not addressing technical difficulties.7-9 The Cochrane Collaboration has identified only two methodologically adequate studies of atraumatic needles for diagnostic lumbar puncture (C Sudlow, personal communication). We aimed to compare the incidence of headache with atraumatic and standard needles and to evaluate technical difficulties.
Participants and methods
Participants
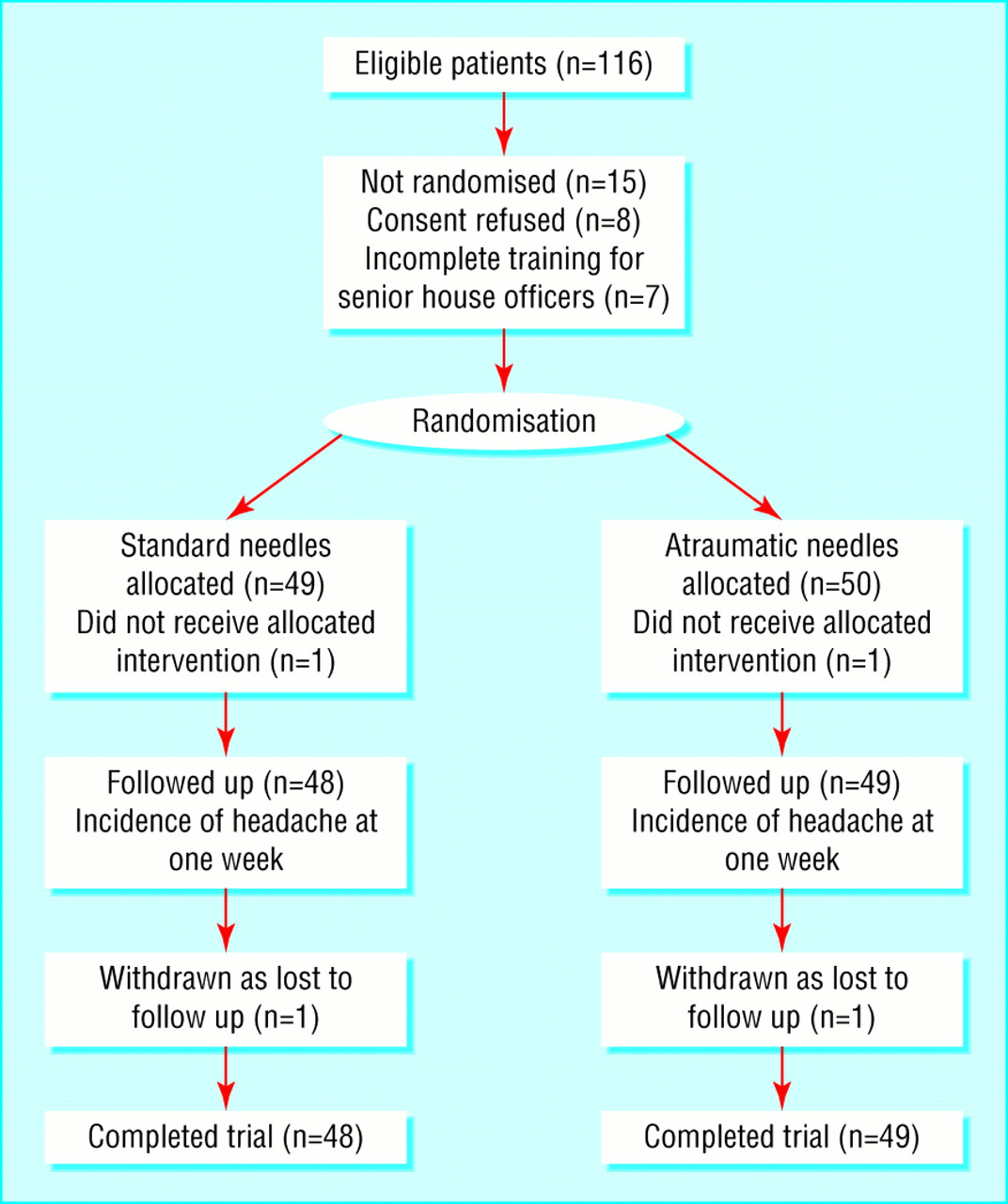
A local pilot study established the feasibility of training medical staff on rotation in the use of atraumatic needles. We considered as eligible for our study all patients attending the investigation ward of a regional neurology unit for elective diagnostic lumbar puncture between September 1998 and February 1999. We excluded patients with a history of chronic headache requiring analgesics and those with known or suspected idiopathic intracranial hypertension or other causes of an increased cerebrospinal fluid pressure. We did not specifically exclude patients if they had had previous lumbar puncture or spinal surgery or if other potential confounding factors were present. Patients received standard information about the procedure and complications. After consenting, the patients were randomised to lumbar puncture with either a 20 gauge atraumatic needle (Sprotte or Pajunk) or a standard needle (Quincke) (fig 1). Randomisation was by a computer generated code stored in opaque envelopes that were serially numbered and sealed.

Atraumatic (top) and standard (bottom) needles for lumbar puncture
Interventions
Seven senior house officers performed the lumbar punctures over the study period. Each was attached to the neurology department for three to six months. Before the study, they received standard training in lumbar puncture techniques, including the manufacturer's video guidelines on the use of atraumatic needles. For at least one month they each performed lumbar punctures with both types of needle. All procedures were performed with the patient in the left lateral position, and 2% lignocaine was used as local anaesthetic. The orientation of the needle bevel during insertion was not stipulated. After withdrawal of cerebrospinal fluid, the needle stylet was reinserted routinely before the needle was withdrawn. Operators were allowed four attempts with the initially allocated needle type, with a maximum of two attempts at any one level. If these were unsuccessful, the operator was allowed two attempts with the alternative needle type before involving a senior colleague or radiological guidance (see figure on BMJ's website). The use of an introducer for the atraumatic needles was left to the operator's discretion. All patients rested in bed for at least four hours after the procedure, and fluid intake was encouraged.
The patients' age, sex, body mass index, and presumptive diagnoses were recorded. During the procedure the operators documented the number of attempts, the time involved with each, opening and closing pressure, the volume of cerebrospinal fluid removed, and the volume of local anaesthetic used. Immediately after the lumbar puncture, the operator and the patient evaluated the procedure for ease and discomfort respectively, with a visual analogue scale (0-10 cm). If both types of needle were necessary, the operator scored each needle separately, but the patient evaluated the procedure as a whole. At 24 hours (or discharge, if sooner) the patients rated the extent of headache and backache on separate visual analogue scales. Nursing staff recorded the length of stay after lumbar puncture.
Follow up
One week after lumbar puncture, the patients were telephoned by a single observer who was blinded to needle allocation. The incidence of both postural headache and backache were recorded and their severity graded as mild, moderate, or severe. The duration of symptoms (hours) and the requirements for analgesia or medical contact were recorded.
End points
Our primary end point was the incidence of moderate or severe headache at one week according to needle type (intention to treat analysis). Our secondary end points were the incidence of moderate or severe headache at one week by successful needle type, incidence of headache at 24 hours, incidence of backache at 24 hours and one week, and ease of use by operator. We undertook additional analyses of the proportion of patients requiring medical interventions within one week of lumbar puncture and the proportion requiring more than one attempt for successful lumbar puncture. For primary and secondary end points we calculated the relative risk, absolute risk reduction, relative risk reduction, and numbers needed to treat for benefit, with 95% confidence intervals. We compared categorical data by χ2 tests and continuous variables by t tests. We calculated the median and interquartile ranges for the duration of symptoms, and we compared them with Mann-Whitney U tests. Correlations were sought with Pearson's product moment coefficient.

{kind=link}
{kind=link}
Results
Patients' characteristics
We randomised 101 of 116 eligible patients during the study period (fig 2), 99 of whom completed the follow up. Presumptive neurological diagnoses being investigated were multiple sclerosis (73 patients), peripheral polyneuropathy (4), chronic fatigue (2), motor neurone disease (2), myelopathy (2), and other cases of neurological disorders (11). Three patients had headache disorders at entry to the trial, and three other patients gave an incidental history of chronic headache, which was not the reason for investigation.
Patients' characteristics and procedural measurements at baseline were identical except for higher body mass index in the standard needle group. Table 1 shows the baseline details.
Baseline characteristics of patients randomised to lumbar puncture with atraumatic or standard needles. Values are means (SDs) unless stated otherwise
Two procedures were abandoned and were therefore excluded from the analyses; one was abandoned after six attempts (four with atraumatic needles and two with standard needles) and the second after four prolonged attempts with the standard needle. We therefore had complete data for 97 patients (49 allocated to atraumatic needles and 48 allocated to standard needles). Lumbar puncture was unsuccessful after four attempts with the atraumatic needle in eight patients. All patients subsequently underwent successful lumbar puncture after one attempt with the standard needle (table 2).
Operator findings with atraumatic and standard needles for lumbar puncture
Symptoms in patients undergoing lumbar puncture with atraumatic or standard needles. Values are numbers of patients unless stated otherwise
Primary and secondary end points. Values are numbers of patients unless stated otherwise
The severity of headache did not differ between the groups at 24 hours (table 3). The incidence of moderate or severe headache was reduced significantly by atraumatic needles both by intention to treat analysis and successful needle analysis (table 4). The incidence of headache did not correlate with the patient's age, sex, or body mass index. The headache at one week in three patients with major prior headache was severe in one and absent in two (all randomised to standard needles). Benefit was maintained irrespective of body mass index, although smaller numbers were reflected in wider confidence intervals and loss of significance: relative risk reduction 46% (−3% to 96%), 48% (−22% to 118%), and 56% (−31% to 111%) in patients with a body mass index of less than 25, 25 or more but less than 29, and 29 or more respectively.
Ease of use
Operators found the atraumatic needle more difficult to use than the standard needle, although the duration of the procedure did not differ between the two needles. Ease of procedure correlated with body mass index (r=0.23). Atraumatic needles were associated with a non-significant increase in the risk of more than one attempt at lumbar puncture being required (table 4). This risk was related to body mass index: relative risk of multiple attempts with atraumatic needles was non-significantly reduced by 45% (32% reduction to 122% increase) in patients with a body mass index of less than 25 and significantly increased by 277% (118% to 436%) in those with a body mass index of 25 or more. In logistic regression there was a significant interaction between needle type and body mass index regarding the need for multiple attempts at lumbar puncture; neither factor individually was predictive.
Other endpoints
Discomfort during the procedure was graded equally by patients in both groups. Discharge was not delayed by symptoms in any patient. Incidence and severity of backache did not differ between groups at 24 hours or one week.
The eight patients in whom lumbar puncture was unsuccessful with atraumatic needles had a higher body mass index, were younger, found the procedure more uncomfortable, and described more severe backache at 24 hours than those in whom first lumbar punctures were successful.
Patients undergoing lumbar puncture with the standard needle required more medical advice, analgesia, and intervention in the week after lumbar puncture, including two hospital admissions, than those undergoing the procedure with an atraumatic needle (table 5). Overall need for medical interventions was reduced by successful use of the atraumatic needle (table 4), although the numbers of patients needing medical contact other than for analgesics were too small to permit definitive conclusions.
Medical intervention according to needle type after successful lumbar puncture
Discussion
Our study confirms a reduced incidence of moderate to severe headache after diagnostic lumbar puncture with atraumatic needles in a patient group typical of neurological practice. We found a higher incidence of dural puncture headache than some reports—for example, 25% with moderate to severe headache over seven days after lumbar puncture with standard 20 gauge needles compared with 16% after lumbar puncture with atraumatic needles in similar neurological populations. 2 3 Others have reported incidences as high as 54%, comparable to our results.10 Operator experience may be a factor, with specifically trained staff or experienced neurologists in previous studies contrasting with our less experienced operators, who are typical of those likely to perform lumbar puncture in UK hospitals. 2 3 Our patients were also younger than those in some series, and younger age has been associated with a higher incidence of dural puncture headache. 2 11
What is already known on this topic
The incidence of dural puncture headache can be reduced by using atraumatic needles for spinal anaesthesia or myelography
A reduction in the incidence of headache has also been shown in two studies of diagnostic lumbar puncture, but confounding factors such as differing needle calibres have impeded ascertainment of the magnitude of benefit, and there are no data on ease of use
What this study adds
A reduced incidence of headache with atraumatic needles was confirmed: one moderate to severe headache was avoided for every four patients undergoing lumbar puncture
The need for medical interventions was also reduced with atraumatic needles: one intervention was avoided for every three patients undergoing lumbar puncture
Atraumatic needles had a higher failure rate than standard needles owing to a greater failure rate in patients with a high body mass index; one additional patient needed more than one attempt for every seven undergoing lumbar puncture
Point estimates of the number needed to treat for benefit indicate that one moderate to severe headache is avoided for every four patients tapped with atraumatic rather than standard needles: this was at the potential expense of one additional patient requiring more than one lumbar puncture attempt for every seven patients treated. Taking into account the higher failure rate with atraumatic needles in “successful needle” rather than intention to treat analysis, the absolute benefit in terms of headaches and subsequent medical interventions avoided persisted, with a number needed to treat of 5 for each end point, but much wider confidence intervals. Reducing the failure rate in practice is therefore crucial if patients are to benefit from lumbar punctures with atraumatic needles. The failure rate in our study (16%) was high, consistent with operators' grading of atraumatic needles as significantly more difficult to use than standard needles, notably so in patients with a high body mass index. The number needed to treat for benefit would be greater if baseline incidence was closer to rates suggested in the literature.
On the basis of these data it would be appropriate to introduce atraumatic needles into standard neurological practice for diagnostic lumbar puncture, provided that failure rates are reviewed. Standard needles will continue to be required, particularly in patients with a high body mass index, in whom failure was most often observed. Standard needles will also continue to be used for therapeutic lumbar punctures for idiopathic intracranial hypertension or hydrocephalus. If these results are borne out in practice, the sevenfold higher cost of atraumatic needles compared with standard needles (£5.30 versus £0.78 at local health board prices) should be offset by the reduced need for medical intervention.
Acknowledgments
We thank the senior house officers who contributed to the study and the medical illustration department of Southern General Hospital for figure 1.
Contributors: DRSJ conceived the study, undertook collection of the pilot data, and reviewed the manuscript. SRT undertook data collection, supervised staff training, performed all follow ups and data entry, and drafted the manuscript. KWM designed the study, performed the analyses, and jointly wrote the manuscript; he will act as guarantor for the paper.
Footnotes
-
Funding Glasgow Neurosciences Foundation.
-
Competing interests None declared.
-
 The procedure for the operators appears on the BMJ's website
The procedure for the operators appears on the BMJ's website