Breast cancer
BMJ 2000; 321 doi: https://doi.org/10.1136/bmj.321.7263.745 (Published 23 September 2000) Cite this as: BMJ 2000;321:745
- J R C Sainsbury,
- T J Anderson,
- D A L Morgan
Breast cancers are derived from the epithelial cells that line the terminal duct lobular unit. Cancer cells that remain within the basement membrane of the elements of the terminal duct lobular unit and the draining duct are classified as in situ or non-invasive. An invasive breast cancer is one in which there is dissemination of cancer cells outside the basement membrane of the ducts and lobules into the surrounding adjacent normal tissue. Both in situ and invasive cancers have characteristic patterns by which they can be classified.

Classification of invasive breast cancers
The most commonly used classification of invasive breast cancers divides them into ductal and lobular types. This classification was based on the belief that ductal carcinomas arose from ducts and lobular carcinomas from lobules. We now know that invasive ductal and lobular breast cancers both arise from the terminal duct lobular unit, and this terminology is no longer appropriate. Some tumours show distinct patterns of growth and cellular morphology, and on this basis certain types of breast cancer can be identified. Those with specific features are called invasive carcinomas of special type, while the remainder are considered to be of no special type. This classification has clinical relevance in that certain special type tumours have a much better prognosis than tumours that are of no special type.
Classification of invasive breast cancers
Special types
• Tubular • Cribriform • Medullary
• Mucoid • Papillary • Classic lobular
No special type
• Commonly known as NST or NOS (not otherwise specified)
• Useful prognostic information can be gained by grading such cancers

Invasive carcinomas showing diffuse infiltration through breast tissue: grade I (left), grade II (centre), and grade III (right)
Tumour differentiation
Among the cancers of no special type, prognostic information can be gained by grading the degree of differentiation of the tumour. Degrees of glandular formation, nuclear pleomorphism, and frequency of mitoses are scored from 1 to 3. For example, a tumour with many glands would score 1 whereas a tumour with no glands would score 3. These values are combined and converted into three groups: grade I (score 3-5), grade II (scores 6 and 7), and grade III (scores 8 and 9). This derived histological grade—often known as the Bloom and Richardson grade or the Scarff, Bloom, and Richardson grade after the originators of this system—is an important predictor of both disease free and overall survival.

Survival associated with invasive breast cancer according to tumour grade
Other features
Other histological features in the primary tumour are also of value in predicting local recurrence and prognosis.
Lymphatic or vascular invasion (LVI)
The presence of cancer cells in blood or lymphatic vessels is a marker of more aggressive disease, and patients with this feature are at increased risk of both local and systemic recurrence.

Extensive in situ component (EIC)
If more than 25% of the main tumour mass contains non-invasive disease and there is in situ cancer in the surrounding breast tissue, the cancer is classified as having an extensive in situ component. Patients with such tumours are more likely to develop local recurrence after breast conserving treatment.
Staging of invasive breast cancers
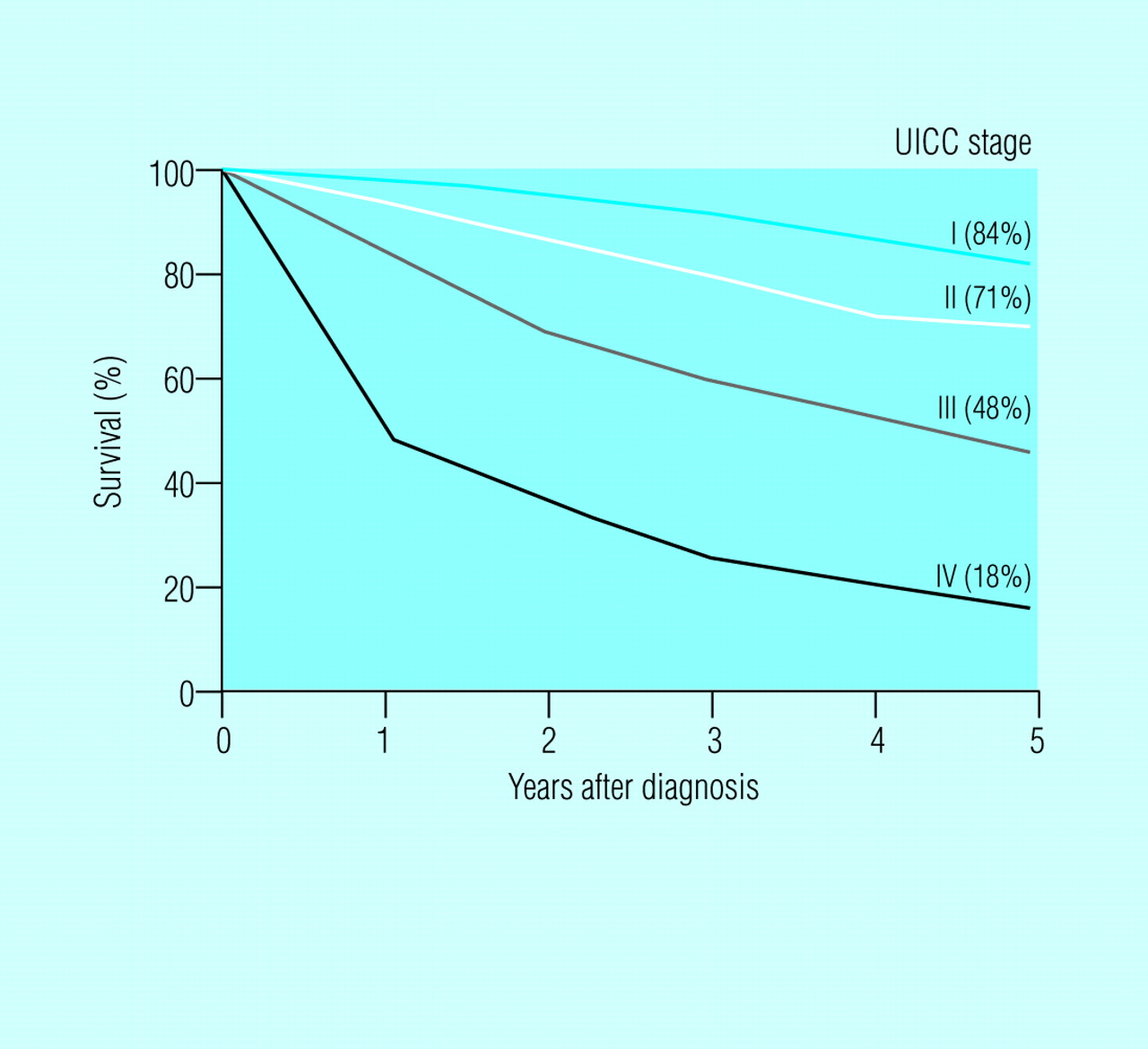
When an invasive breast cancer is diagnosed the extent of the disease should be assessed and the tumour staged. The two staging classifications in current use are not well suited to breast cancer: the tumour node metastases (TNM) system depends on clinical measurements and clinical assessment of lymph node status, both of which are inaccurate, and the International Union Against Cancer (UICC) system incorporates the TNM classification. To improve the TNM system, a separate pathological classification has been added; this allows tumour size and node status, as assessed by a pathologist, to be taken into account. Prognosis in breast cancer relates to the stage of the disease at presentation.

Wide local excision showing invasive and in situ cancer which has been completely excised. As the lesion was very close to the skin, overlying skin has been removed
TNM classification of breast tumours
Tis Cancer in situ
T1 ≤2 cm (T1a ≤ 0.5 cm, T1b >0.5-1, T1c >1-2 cm)
T2 >2 cm-5 cm
T3 >5 cm
T4a Involvement of chest wall
T4b Involvement of skin (includes ulceration, direct infiltration, peau d'orange, and satellite nodules)
T4c T4a and T4b together
T4d Inflammatory cancer
N0 No regional node metastases
N1 Palpable mobile involved ipsilateral axillary nodes
N2 Fixed involved ipsilateral axillary nodes
N3 Ipsilateral internal mammary node involvement (rarely clinically detectable)
M0 No evidence of metastasis
M1 Distant metastasis (includes ipsilateral supraclavicular nodes)
To ensure that there is no gross evidence of disease all patients with invasive breast cancer should have a full blood count, liver function tests, and a chest radiograph. Patients with stage I and stage II disease have a low incidence of detectable metastatic disease, and in the absence of abnormal results of liver function tests or specific signs or symptoms they should not undergo further investigations to assess metastatic disease. Patients with bigger or more advanced tumours should be considered for bone and liver scans if these could lead to a change in clinical management.
Correlation of UICC (1987) and TNM classifications of tumours

Survival associated with invasive breast cancer according to stage of disease
Surgical treatment of localised breast cancer
Most patients will have a combination of local treatments to control local disease and systemic treatment for any micrometastatic disease. Local treatments consist of surgery and radiotherapy. Surgery can be an excision of the tumour with surrounding normal breast tissue (breast conservation surgery) or a mastectomy. At least 12 randomised clinical trials have compared mastectomy and breast conservation treatment. Nine were included in a recent meta-analysis and included 4981 women suitable for mastectomy or breast conservation. There was a non-significant 2% ± 7 relative reduction in death in favour of breast conserving therapy. Local recurrence rates were similar, with a non-significant 4% ± 8 relative reduction in favour of mastectomy.
Risk factors for local recurrence of cancer after breast conservation
Certain clinical and pathological factors may influence selection for breast conservation or mastectomy because of their impact on local recurrence after breast conserving therapy. These include an incomplete initial excision, young age, the presence of an extensive in situ component, the presence of lymphatic or vascular invasion, and histological grade. Young patients (<35) are two to three times more likely to develop local recurrence than older patients. While young patients are more likely to have other risk factors for local recurrence, young age appears to be an independent risk factor.

Patient who was treated with breast conservation and developed a new primary cancer in the lower part of treated breast. The metal clips mark the site of the original cancer. Approximately 20% of so-called breast recurrences after breast conservation are second primary cancers
Breast conservation surgery
Breast conservation surgery may consist of excision of the tumour with a 1 cm margin of normal tissue (wide local excision) or a more extensive excision of a whole quadrant of the breast (quadrantectomy). The single most important factor which influences local recurrence after breast conservation is the completeness of excision. Invasive or in situ disease at the resection margins increases local recurrence by a factor of 3.4 (95% CI 2.6-4.6). EIC increases local recurrence only when margins are involved. The presence of LVI doubles local recurrence rates. Grade I tumours appear to have a lower recurrence rate by a factor of 1.5 compared with grade II or III tumours. The wider the excision the lower the recurrence rate but the worse the cosmetic result. There is no size limit for breast conservation surgery, but adequate excision of lesions over 4 cm produces a poor cosmetic result; thus in most breast units breast conserving surgery tends to be limited to lesions of 4 cm or less. There is no age limit for breast conservation.
Risk factors for local recurrence of cancer after breast conservation
Relation between age and local recurrence of cancer after breast conservation
Breast cancers suitable for treatment by breast conservation
Single clinical and mammographic lesion
Tumour ≤4 cm in diameter
No sign of local advancement (T1, T2 <4 cm), extensive nodal involvement (N0, N1), or metastases (M0)
Tumour >4 cm in large breast

Patient with a poor cosmetic result after breast conservation before (left) and after (right) a myocutaneous flap reconstruction
Factors affecting cosmetic outcome
17% (95% CI 13-23) of women have a poor cosmetic result after wide excision and radiotherapy. Wider excisions give poorer cosmetic results. For this reason only dimpled or retracted skin overlying a localised breast cancer should be excised. Where large volumes of tissue are being removed or where wide excision of a small tumour removes a significant portion of the breast, consideration should be given to filling the defect by a latissimus dorsi mini-flap. For patients who get a poor cosmetic result after breast conservation options include reduction surgery on the contralateral breast or replacing the tissue lost by surgery using a myocutaneous flap.
Mastectomy
About a third of localised breast cancers are unsuitable for treatment by breast conservation but can be treated by mastectomy, and some patients who are suitable for breast conservation surgery opt for mastectomy. Mastectomy removes the breast tissue with some overlying skin, usually including the nipple. The breast is removed from the chest wall muscles (pectoralis major, rectus abdominus, and serratus anterior), which are left intact. Mastectomy should be combined with some form of axillary surgery.
Patients who are best treated by mastectomy
Those who prefer treatment by mastectomy
Those for whom breast conservation treatment would produce an unacceptable cosmetic result (includes most central lesions and carcinomas >4 cm in diameter, although breast conserving surgery is now possible if these lesions are successfully treated by primary systemic therapy or if the breast is reconstructed using a latissimus dorsi mini-flap)
Those with either clinical or mammographic evidence of more than one focus of cancer in the breast
Common complications after mastectomy include formation of seroma, infection, and flap necrosis. Collection of fluid under mastectomy flaps after suction drains have been removed (seroma) occurs in a third to a half of all patients. It is more common after a mastectomy and axillary node clearance than after mastectomy and node sampling. The seroma can be aspirated if it is troublesome. Infection after mastectomy is uncommon, and when it occurs it is usually secondary to flap necrosis. Occasionally areas of necrotic skin need to be excised and skin grafts applied. Most patients treated by mastectomy are suitable for some form of breast reconstruction, which should ideally be performed at the same time as the initial mastectomy.
Factors associated with increased rates of local recurrence after mastectomy
Axillary lymph node involvement
Lymphatic or vascular invasion by cancer
Grade III carcinoma
Tumour >4 cm in diameter (pathological)
Follow up of patients after surgery
Local recurrence after mastectomy is most common in the first two years and decreases with time. By contrast, local recurrence after breast conservation occurs at a fixed rate each year. Follow up schedules should take this difference into account. The aim of follow up is to detect local recurrence while it is treatable or to detect contralateral disease. Patients with carcinoma of one breast are at high risk of cancer in the other breast, and about 0.6% a year develop this. All patients under follow up after breast cancer should, therefore, have mammography performed regularly (the interval between mammograms varies from one to two years in different units) on one or both breasts. Mammograms can be difficult to interpret after breast conservation because scarring from surgery can result in the formation of a stellate opacity and localised distortion, which can be difficult to differentiate from cancer recurrence. Magnetic resonance imaging is useful in this situation.

MRI showing an enhanced lesion in the breast characteristic of local recurrence
Follow up schedule after surgery for breast cancer
Annual clinical examination
Annual or biannual mammography indefinitely
Mastectomy
Annual clinical examination for 5 years
Annual or biannual mammography indefinitely
Radiotherapy
Studies have shown that all patients should receive radiotherapy to the breast after wide local excision or quadrantectomy. Doses of 40–50 Gy are delivered in daily fractions over three to five weeks. A top up or boost of 10–20 Gy can be given to the excision site either by external beam irradiation or by means of radioactive implants, although it is not yet clear whether a boost is always necessary. After mastectomy radiotherapy should be considered for patients at high risk of local recurrence: patients with involvement of pectoralis major or any two of the other factors associated with increased risk should be given postoperative radiotherapy. Although the Early Breast Cancer Trialists' Overview showed no survival advantage for post-mastectomy chest wall radiotherapy, three recent studies which combined radiotherapy and systemic therapy in both premenopausal and postmenopausal high risk women have shown improved survival in patients who received chest wall radiotherapy.

Effect of radiotherapy on local recurrence after wide local excision

Effect of radiotherapy on local recurrence after quadrantectomy

Survival results in the Danish Breast Cancer Cooperative Group trial 82b comparing CMF (cyclophosphamide, methotrexate, 5-fluorouracil) chemotherapy and radiation therapy to chemotherapy alone in premenopausal patients treated with mastectomy
Complications
With modern machinery and the delivery of smaller fractions the dose of radiotherapy delivered to the skin is minimised. This has dramatically reduced the incidence of immediate skin reactions and subsequent skin telangiectasia. With tangential fields, only a part of the left anterior descending artery and a small fraction of lung tissue are now routinely included within radiotherapy fields, and the risks of cardiac damage and of pneumonitis are low. Reports of increased cardiac deaths many years after radiotherapy for left sided breast cancer relate to old radiotherapy techniques which delivered higher doses of radiotherapy to a much greater proportion of the heart.
Key references
Radiation pneumonitis, which is usually transient, affects less than 2% of patients treated with tangential fields. Rib doses are also smaller, with the consequence that rib damage is now much less common than it used to be. In the past there were problems with overlapping radiotherapy fields, resulting in an increased dose of radiation to a small area. If this occurs in the axilla it can cause brachial plexopathy.

Survival results in the Danish Breast Cancer Cooperative Group trial 82c comparing tamoxifen (TAM) and radiation therapy (RT) to tamoxifen alone in postmenopausal patients treated with mastectomy
Cutaneous radionecrosis and osteoradionecrosis are now rarely seen but do occur in patients who were treated several years ago. Excision of affected areas and reconstruction with local or distant myocutaneous flaps are sometimes necessary, as regular antibiotics and dressings rarely result in wound healing.

Good cosmetic result after breast conserving surgery and breast radiotherapy


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Acknowledgments
The italics of the data presented in graphs are: C W Elston and I O Ellis, Histopathology 1992;19:403-10 for survival associated with tumour grade; B Fisher and C Redmond, Monogr Natl Cancer Inst 1992;11:7,13 for recurrence after wide local excision; and U Veronesi et al,. N Engl J Med 1993;328:1587-91 (copyright Massachusetts Medical Society) for recurrence after quadrantectomy. The data are reproduced with permission of the journals or copyright holders.
Footnotes
-
J R C Sainsbury is consultant surgeon, Huddersfield Royal Infirmary, Huddersfield, T J Anderson is reader, Department of Pathology, University of Edinburgh, Edinburgh, and D A L Morgan is consultant clinical oncologist, Nottingham City Hospital, Nottingham.
The ABC of breast diseases is edited by J Michael Dixon, consultant surgeon and senior lecturer in surgery, Edinburgh Breast Unit, Western General Hospital, Edinburgh.