Chemotherapy in non-small cell lung cancer: a meta-analysis using updated data on individual patients from 52 randomised clinical trials
BMJ 1995; 311 doi: https://doi.org/10.1136/bmj.311.7010.899 (Published 07 October 1995) Cite this as: BMJ 1995;311:899
- Non-small Cell Lung Cancer Collaborative Groupa
- a The collaborative group members and the organisations and groups that collaborated in the meta-analysis are listed at the end of the article.
- Correspondence to: Dr L A Stewart, MRC Cancer Trials Office, 5 Shaftesbury Road, Cambridge CB2 2BW, or Dr J P Pignon, Institut Gustave Roussy, 94805 Villejuif Cedex, France.
- Accepted 21 July 1995
Abstract
Objective: To evaluate the effect of cytotoxic chemotherapy on survival in patients with non-small cell lung cancer.
Design: Meta-analysis using updated data on individual patients from all available randomised trials, both published and unpublished.
Subjects: 9387 patients (7151 deaths) from 52 randomised clinical trials.
Main outcome measure: Survival.
Results: The results for modern regimens containing cisplatin favoured chemotherapy in all comparisons and reached conventional levels of significance when used with radical radiotherapy and with supportive care. Trials comparing surgery with surgery plus chemotherapy gave a hazard ratio of 0.87 (13% reduction in the risk of death, equivalent to an absolute benefit of 5% at five years). Trials comparing radical radiotherapy with radical radiotherapy plus chemotherapy gave a hazard ratio of 0.87 (13% reduction in the risk of death; absolute benefit of 4% at two years), and trials comparing supportive care with supportive care plus chemotherapy 0.73 (27% reduction in the risk of death; 10% improvement in survival at one year). The essential drugs needed to achieve these effects were not identified. No difference in the si
Conclusion: At the outset of this meta-analysis there was considerable pessimism about the role of chemotherapy in non-small cell lung cancer. These results offer hope of progress and suggest that chemotherapy may have a role in treating this disease.
Key messages
This international collaborative meta-analysis collected updated data on individual patients from 9387 patients included in 52 randomised clinical trials
This meta-analysis provides the currently most reliable estimates of the average effect of chemotherapy in broad classes of non-small cell lung cancer
Modern chemotherapy regimens may have a role in treating all stages of non-small cell lung cancer, although further research is needed to confirm the suggestion of benefit
Further clinical trials are needed to assess short term chemotherapy and to compare different chemotherapies
Introduction
Worldwide more than half a million new cases of lung cancer are diagnosed annually.1 About 80% of these tumours are of non-small cell histological type,2 including adenocarcinomas and squamous cell and large cell carcinomas. Non-small cell lung cancer is a leading cause of deaths related to cancer,3 and five year survival across all stages is about 12%.4 Surgery is the treatment of choice, but only about 20% of tumours are suitable for potentially curative resection.5 A further, small proportion of patients, usually presenting with locally advanced disease, undergo radical thoracic radiotherapy. Most patients with late stage or metastatic disease are treated palliatively.
Although cytotoxic chemotherapy is used routinely in treating small cell lung cancer, its role in non-small cell lung cancer remains controversial. A recent international consensus report concluded that post-operative chemotherapy was of unproved benefit and should be considered experimental.6 This uncertainty remains despite over 30 years of research involving around 10000 patients in over 50 randomised clinical trials examining the efficacy of chemotherapy when combined with local treatment or best supportive care. With few exceptions, however, most of these trials were too small to reliably detect moderate treatment effects. Only four trials involved more than 400 patients and about half the trials each recruited fewer than 100 patients. Consequently, although a few trials have reported significant results,both for and against chemotherapy, most trials have been inconclusive and the pattern of results could be consistent with moderate treatment benefits. The most reliable and unbiased way to assess the evidence and to establish the size of any possible treatment effect is to conduct a meta-analysis of updated data on individual patients.7
Such a meta-analysis was therefore initiated by the British Medical Research Council's Cancer Trials Office, Cambridge; the Institut Gustave Roussy, Villejuif, France; and the Istituto Mario Negri, Milan, Italy, and was carried out on behalf of the Non-small Cell Lung Cancer Collaborative Group.
Patients with non-small cell lung cancer can be classified into three broad categories according to the primary treatment that they receive: surgery, radical, or potentially curative radiotherapy and supportive care. There is a continuum of patients both within and between these categories, but we took the pragmatic approach of asking general questions about whether chemotherapy is effective in each of these groups. We made comparisons corresponding to the type of treatment usually considered at the time of presentation: early disease (surgery v surgery plus chemotherapy; surgery plus radiotherapy v surgery plus radiotherapy plus chemotherapy); locally advanced disease (radical radiotherapy v radical radiotherapy plus chemotherapy); and advanced disease (supportive care v supportive care plus chemotherapy). The main objective was to investigate the effect of chemotherapy on survival in these four treatment settings. A further objective was to assess whether any possible effects were consistent in well defined subgroups of patients.
Methods
The methods and investigations were prespecified in clinical and analysis protocols. (Copies of these documents are available on request.) Collection and validation of data were carried out in two centres (Cancer Trials Office and the Institut Gustave Roussy), and after the data had been cross checked, a common database was agreed.
ELIGIBILITY CRITERIA
Trials were eligible for inclusion if they randomised patients with non-small cell lung cancer between one of the four primary treatments and the same treatment plus an established form of cytotoxic chemotherapy. Each trial had to be unconfounded and be believed to have been randomised in a way that precluded prior knowledge of the next treatment to be assigned. Trials were eligible if they started recruitment after 1 January 1965 and completed recruitment by 31 December 1991. Trials allowing patients to have received chemotherapy before randomisation were ineligible. Trials with surgery and radical radiotherapy should not have permitted previous treatment for any other malignancy in the surgical comparison. Trials were eligible only if they had randomised patients who had undergone a potentially curative resection. Trials of neo-adjuvant treatment were not included in this comparison as it was considered too early to evaluate such trials. Trials of radical radiotherapy using orthovoltage radiotherapy or a total radiation dose of <30 Gy were excluded, as were trials in which drugs were used with the primary aim of sensitisation to radiation.
IDENTIFICATION OF TRIALS
To avoid publication bias both published and unpublished studies were included, and several methods were used to identify all relevant trials. Computerised bibliographic searches with Medline and CancerCD were supplemented with hand searches of meetings abstracts, bibliographies of books, reviews, and specialist journals. Trial registers managed by the National Cancer Institute (PDQ, ClinProt), United Kingdom Coordinating Committee for Cancer Research, and the Union Internationale Contre le Cancer were also consulted. Experts, pharmaceutical companies, and all trialists who took part in the meta-analysis were also asked to help to identify trials.
DATA
Updated information on survival status and date of last follow up was sought, together with treatment allocated, date of randomisation, age, sex, histological cell type, stage, and performance status. To avoidpotential bias this information was also required for patients who had been excluded from the investigators' analysis. All data were checked for internal consistency and against the trial protocol and published reports. Range checks were performed and extreme values were checked with the trialists. Each trial was analysed individually, and the resulting survival analyses and trial data were sent to the trialists for verification.
ANALYSIS
The protocol specified that trials would be subdivided according to the use of cisplatin, primarily as an objective means of specifying modern and older chemotherapy regimens. Classification based on date was considered unsatisfactory as it has less clinical meaning and trials take different periods of time to complete. There was also much interest in the role of cisplatin. Before the data were analysed, it became clear that trials in the groups not using cisplatin were either early trials that used alkylating agents (often administered orally) over a prolonged period of time or recent trials using modern regimens not containing cisplatin. Trials were therefore finally classified into the following categories: (a) regimens containing cisplatin, (b) regimens using alkylating agents for more than one year, (c) regimens containing etoposide or vinca alkaloids but not cisplatin, and (d) other regimens. Each trial could belong to only one category.
All analyses were carried out on intention to treat—that is, patients were analysed according to their allocated treatment—irrespective of whether they received that treatment.
STATISTICS
For each comparison, survival analyses were stratified by trial, and the log rank expected and observed numbers of deaths were used to calculate individual and overall pooled hazard ratios with the fixed effect model.8 Thus the time to death for individual patients was used within trials to generate the hazard ratio representing the overall risk of dying receiving treatment c ompared with the control. To investigatethe effect of chemotherapy within prespecified subgroups, similar stratified analyses were performed. A hazard ratio was calculated for each prespecified category—for example, for males and for females within each individual trial—and these ratios were then combined to give overall hazard ratios for males and females for each treatment setting.
As the absolute difference in treatment effect depends on the hazard ratio and the underlying baseline survival—and the way that these interrelate is not intuitive—the results are presented as both hazard ratios and absolute differences. Here, as in the other analyses, proportional hazards are assumed. The absolute survival difference was calculated by using survival on the control arms of cisplatin based trials within each treatment comparison as a baseline at given points in time as follows:
Absolute benefit=(exponential (hazard ratiox1n baseline survival))-baseline survival
χ2 Heterogeneity tests10 were used to test for gross statistical heterogeneity over all trials in a comparison (χ2Het T), between chemotherapy categories (test for interaction χ2HetB) and within chemotherapy categories (χ2HetW, (χ2HetT=χ2HetB+χ2HetW). When appropriate, the heterogeneity within a single category (χ2HetC) has also been calculated. These tests are aimed primarily at detecting quantitative differences—that is, differences in size rather than direction—and were chosen because qualitative differences were not anticipated. Whenever gross satistical heterogeneity was detected the rationale for combining trials was questioned and the source of heterogeneity investigated, rather than using a random effects model.11
Survival curves are presented as simple (non-stratified) Kaplan-Meier curves.12 All P values quoted are two sided. Unless otherwise specified χ2 values are on one degree of freedom.
Results
In all, 91 trials were identified as potentially eligible for the meta-analysis. Thirty three of these were found to be ineligible and therefore excluded (appendix 1). Of the 58 eligible trials13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 (Lung Cancer Study Group protocol 853, unpublished data; M Imaizumi, personal communication; Finnish Lung Cancer Study Group, unpublished data; European Organisation for Research and Treatment of Cancer protocol 08861, unpublished data; G Anderson, personal communication; European Organisation for Research and Treatment of Cancer protocol 08842, unpublished data; South Western Oncology Group protocol 8300, unpublished data), data were not available from six as they had been lost or destroyed or were untraceable25 26 49 50 51 52 (appendix 1). Data from 52 randomised trials and 9387 patients were therefore included in this meta-analysis.
EARLY DISEASE Surgery v surgery plus chemotherapy
Data were available from 14 trials (4357 patients and 2574 deaths) (table I). Five trials used long term alkylating agents (2145 patients, 1670 deaths), mainly cyclophosphamide and nitrosourea; eight more recent trials (1394 patients, 614 deaths) used cisplatin based combination chemotherapy, three used the regimen of cisplatin, doxorubicin, and cyclophosphamide (CAP), and three used cisplatin with vindesine. The intended dose of cisplatin ranged from 40 mg/m2 to 80 mg/m2 per cycle and total dose from 50 mg/m2 to 240 mg/m2. A further three trials used other drug regimens, all of which included tegafur or UFT (tegafur plus uracil), a drug similar to fluorouracil.63 In all the trials chemotherapy was scheduled to start no later than six weeks after surgery.
Trials comparing surgery with surgery plus chemotherapy. Drugs were given intravenously anddoses per cycle were in mg/m2 unless stated otherwise
The results showed considerable diversity and evidence of a difference in direction of effect between the predefined categories of chemotherapy (table II, fig 1). The test for overall statistical heterogeneity was conventionally significant (P=0.02), as was the test for interaction (P=0.004). No evidence existed, however, of heterogeneity within each category (P=0.21). Thus it is more useful to concentrate on the results for each of the predefined chemotherapy categories than on the overall result.
Main results of meta-analysis of chemotherapy in non-small cell lung cancer

Results of trials of surgery versus surgery plus chemotherapy (test for heterogeneity χ2HetT=28.98, df=16, P=0.02; test for interaction χ2HetB=10.97, df=2, P=0.004, χ2HetW=18.01, df=14, P=0.21) (see tables for references to trials). As West Japan Study Group for Lung Cancer Surgery's seco ndtrial (WJSG 2) fell into two categories, patients in the control arm are included in subtotals of “other drugs” and “cisplatin based” but used only once in overall total, to calculate hazard ratio and confidence interval. The test for heterogeneity (χ22HetT) was calculated by counting the study group's second trial as two separate trials. Each individual trial is represented by a square, the centre of which denotes the hazard ratio for that trial, with horizontal bars whose extremities denote the 99% confidence interval and inner bars mark the 95% confidence interval. The size of the square is directly proportional to the amount of information in the trial. The black diamond at the foot of the plot gives the overall hazard ratio when the results of all trials are combined, the centre of which denotes the hazard ratio and the extremities the 95% confidence interval (shaded diamonds represent the hazard ratio for the various specified categories of chemotherapy). Trials are ordered chronologically by date of start of trial (oldest first) within chemotherapy categories
{kind=link}
The results for long term alkylating agents were consistent—the hazard ratio estimates all favoured surgery alone with a combined hazard ratio of 1.15 (P=0.005). This 15% increase in the risk of death translates to an absolute detriment of chemotherapy of 4% at two years and 5% at five years. For regimens containing cisplatin (figures 1 and 2) the pattern of results was again consistent, with hazard ratio estimates for most trials favouring chemotherapy. No obvious statistical heterogeneity existed in the results of these trials (χ2HetC=5.92, df=7, P=0.55), and the overall hazard ratio of 0.87 (P=0.08), or 13% reduction in the risk of death, suggested an absolute benefit from chemotherapy of 3% at two years and 5% at five years (table II), although on their own these results were not conclusive. The 95% confidence intervals for absolute difference in survival were consistent with a 0.5% detriment to a 7% benefit of chemotherapy at two years and similarly consistent with a 1% detriment to a 10% benefit at five years. The trials that were classified as using other regimens gave an estimated hazard ratio of 0.89 in favour of chemotherapy (P=0.30), but there was insufficient information to draw any reliable conclusions.

Survival in trials of surgery versus surgery plus chemotherapy (only trials using regimens based on cisplatin)
{kind=link}
Surgery plus radiotherapy v surgery plus radiotherapy plus chemotherapy
Data were available from all seven eligible trials (807 patients and 619 deaths), six of which used a cisplatin based regimen, with intended doses of cisplatin ranging from 40mg/m2 to 100mg/m2 per cycle and total dose from 80mg/m2 to 400mg/m2 (table III). Total planned doses of radiotherapy ranged from 40 Gy in 10 fractions to 65 Gy in 33 fractions, and the delay between surgery and the first adjuvant treatment was scheduled to be no longer than seven weeks.
Trials comparing surgery plus radiotherapy with surgery plus radiotherapy plus chemotherapy. Drugs were given intravenously and doses per cycle were in mg/m2 unless stated otherwise
The overall hazard ratio of 0.98 (P=0.76) was marginally in favour of chemotherapy (table II, fig 3). No gross statistical heterogeneity existed between the trials (P=0.73). For the cisplatin based trials (figures 3 and 4) the hazard ratio of 0.94 (P=0.46), or 6% reduction in the risk of death, favoured chemotherapy, suggesting a 2% absolute benefit at both two and five years. 95% Confidence intervals ranged from a 4% detriment to an 8% benefit at two years and from a 3% detriment to an 8% benefit at five years.

Results of trials of surgery plus radiotherapy versus surgery plus radiotherapy plus chemotherapy (test for heterogeneity χ2HetT=3.62, df=6, P=0.73; test for interaction χ2HetB=1.92, df=1, P=0.17 (see fig 1 for explanation of plot)) (see tables for references to trials). Symbols and conventions as in figure 1
{kind=link}
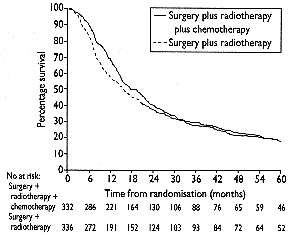
Survival in trials of surgery plus radiotherapy versus surgery plus radiotherapy plus chemotherapy (only trials using regimens based on cisplatin)
{kind=link}
LOCALLY ADVANCED DISEASE Radical radiotherapy v radical radiotherapy plus chemotherapy
Data were available from 22 trials (3033 patients and 2814 deaths) (table IV). Five trials used long term alkylating agents, mainly cyclophosphamide or nitrosourea in combination with methotrexate. Three used vinca alkaloids or etoposide, and three used “other” regimens, which in this comparison were mostly based on doxorubicin. Eleven trials (1780 patients, 1696 deaths) used chemotherapy regimens containing cisplatin, of which two used the regimen of cisplatin, doxorubicin, and cyclophosphamide and seven used a combination of cisplatin plus a vinca alkaloid or etoposide. Intended doses of cisplatin ranged from 40mg/m2 to 120mg/m2 per cycle and total doses from 120mg/m2 to 800mg/m.2 The intended radiation dose forcisplatin based trials ranged from 50 Gy in 20 fractions to 65 Gy in 30 fractions. Ten of these trials started chemotherapy before radiotherapy.
Trials comparing radical radiotherapy with radical radiotherapy plus chemotherapy. Drugs were given intravenously and doses per cycle were in mg/m2 unless stated otherwise
The results showed a significant overall benefit of chemotherapy (table II, fig 5). The hazard ratio of 0.90 (P=0.006), or 10% reduction in the risk of death, corresponded to absolute benefits of 3% at two years and 2% at five years. No gross statistical heterogeneity existed between trials (P=0.56), nor such strong evidence of a difference between chemotherapy categories, which was reflected in the non-significant test for interaction (P=0.59). Trials using long term alkylating agents and “other” regimens yielded a hazard ratio of 0.98 (P=0.81 and P=0.88 respectively), both marginally in favour of chemotherapy but inconclusive. Trials using regimens containing vinca alkaloids or etoposide also favoured chemotherapy, with a hazard ratio of 0.87 (P=0.23), a 13% reduction in the risk of death, but no firm conclusions can be drawn. Trials using cisplatin based chemotherapy provided the most information (more than 50%) and the strongest evidence for an effect in favour of chemotherapy (figures 5 and 6). The hazard ratio of 0.87 (P=0.005), or 13% reduction in the risk of death, was equivalent to absolute benefits of 4% (95% confidence interval 1% to 7%) at two years and 2% (1% to 4%) at five years. However, no firm evidence exists that the results of the trials using regimens containing vinca alkaloids or etoposide or of those using other regimens of modern drugs were any different from those using cisplatin based chemotherapy.

Results of trials of radical radiotherapy versus radical radiotherapy plus chemotherapy (test for heterogeneity χ2HetT=22.33, df=24, P=0.560; test for interaction χ2HetB=1.91, df=3, P=0.592 (see fig 1 for explanation of plot)) (see tables for references to trials). Symbols and conventions as in figure 1
{kind=link}

Survival in trials of radical radiotherapy versus radical radiotherapy plus chemotherapy (only trials using regimens based on cisplatin)
{kind=link}
ADVANCED DISEASE Supportive care v supportive care plus chemotherapy
Data were available from 11 trials (1190 patients and 1144 deaths) (table V). Two trials used long term alkylating agents and one used etoposide as a single agent. The remaining eight trials (778 patients, 761 deaths) used cisplatin based chemotherapy, seven of which used a combination of cisplatin and vinca alkaloids or etoposide. The intended dose of cisplatin ranged from 40mg/m2 to 120mg/m2 per cycle, with total doses of 280mg/m2 upwards, including several trials in which chemotherapy was given until the disease progressed or the toxicity was unacceptable. In this advanced disease setting, however, many patients would not have received the planned number of treatment cycles. One trial allowed entry of only patients with metastatic disease; the rest included patients with both locally advanced and advanced disease.
Trials comparing supportive care with supportive care plus chemotherapy. Drugs were given intravenously and doses per cycle were in mg/m2 unless stated otherwise
There was again considerable overall statistical heterogeneity (P<0.0001) and a pronounced difference in the results for the different chemotherapy categories (P=0.003) (table II, fig 7). The result for trials using long term alkylating agents suggests a detriment of chemotherapy, with a hazard ratio of 1.26. With only two such trials, however, the confidence interval was wide (0.96 to 1.66) and the result did not reach conventional levels of significance (P=0.095). The cisplatin based trials showed a benefit of chemotherapy, with a hazard ratio of 0.73 (P<0.0001), a reduction in the risk of death of 27%, equivalent to an absolute improvement in survival of 10% (5% to 15%) at one year, or an increased median survival of 1 1/2 months (1 month to 21/2 months). One trial (CEP-85) showed an extreme result in favour of chemotherapy. Even if this trial was excluded from the analysis, however, the result was still significant in favour of chemotherapy (hazard ratio 0.77 (0.63 to 0.85), P=0.001). When this trial was removed, no gross statistical heterogeneity existed within the cisplatin based category (χ2HetC=10.91, df=6, P=0.09). Survival curves in this setting are drawn only to two years as few patients were alive after this time (fig 8).

Results of trials of supportive care versus supportive care plus chemotherapy (test for heterogeneity χ2HetT=39.65, df=10, P=<0.0001; test for interaction χ2HetB=11.67, df=2, P=0.003 (see fig 1 for explanation of plot)) (see tables for references to trials). Symbols and conventions as in figure 1
{kind=link}

Survival in trials of supportive care versus supportive care plus chemotherapy (only trials using regimens based on cisplatin)
{kind=link}
TREATMENT EFFECT IN PATIENT SUBGROUPS
Predefined subgroups of patients were analysed to determine if evidence existed of a different size of treatment effect in any such group. To minimise heterogeneity, only cisplatin based regimens were included in this analysis. Data on stage were available for 92% of patients, performance status for 94% of patients, and age, sex, and histological cell type for more than 99% of patients. No evidence existed that any group of patients specified by age, sex, histological cell type, performance status, or stage benefited more or less from chemotherapy (figure 9 shows stage, histological cell type, and performance status; more detailed plots and results for age and sex are available on request).

Treatment effect (test for interaction) in cisplatin based trials according to (a) stage: surgery χ2HetB=2.33, P=0.13; surgery plus radiotherapy χ2HetB=3.30, P=0.07; radicalradiotherapy χ2HetB=0.15, P=0.70; supportive care χ2HetB=0.01, P=0.92; (b) histological evidence: surgery χ2HetB=5.4, df=2, P=0.07; surgery plus radiotherapy χ2HetB=4.71, df=2, P=0.09; radical radiotherapy χ2HetB=2.59, df=2, P=0.27; supportive care χ2HetB=1.66, df=2, P=0.44; and (c) performance status: surgery χ2HetB=0.96, P=0.33; surgery plus radiotherapy χ2HetB=1.13, P=0.29; radical radiotherapy χ2HetB=0.01, P=0.92; supportive care χ2HetB=0.66, P=0.42. Symbols and conventions as in figure 1. The various conventional staging and scoring systems used in the trials were converted to common meta-analysis categories (details of these conversions are available on request)
{kind=link}
Discussion
This meta-analysis was based on an extensive dataset comprising 9387 patients from 52 randomised clinical trials that compared local surgical or radiotherapy treatment or best supportive care with the same treatment plus chemotherapy in non-small cell lung cancer. Only six other eligible trials were found, for which data were not available; these were mostly older trials using chemotherapy regimens based on the long term administration of oral alkylating agents, regimens that are no longer used. For the modern, cisplatin based regimens data from approximately 95% of all patients ever entered into all known relevant trials were analysed. Furthermore, for almost all trials the data on individual patients had been updated to the point of data collection, which was often many years after the publication of the trial's results. This meta-analysis therefore provides the most comprehensive and reliable current assessment of the average treatment effect of broad categories of chemotherapy regimens among broad classes of patients with non-small cell lung cancer.
One of the most striking aspects of the results is the consistency inthe direction, and indeed in the estimated hazard ratios, of the various chemotherapy categories among the different primary treatments compared (table II). This consistency allows stronger conclusions to be drawn than perhaps could be inferred from each of the individual results.
In the early and advanced disease settings older trials using long term alkylating agents tended to show a detrimental effect of chemotherapy. This effect was conventionally significant for the adjuvant surgical trials. Chemotherapies of the type used in the early 1970s based on long term administration of alkylating agents are therefore likely to be detrimental to patients with non-small cell lung cancer. The mechanism for this is unknown, although some occurrences of leukaemia after treatment with busulphan have been described for non-small cell lung cancer,64 and a possible model for an observed detrimental effect of cyclophosphamide and other alkylating agents in non-small cell lung cancer has been proposed.65 Clearly, such regimens are not used today, but the result may have implications for other disease sites, although the administration of chemotherapy and the drugs used have changed a lot over the past 20 years.
In all comparisons, results for modern regimens containing cisplatin favoured chemotherapy. These were conventionally significant in the locally advanced and supportive care settings. However, we emphasise that the categorisation of drug regimens was chosen mainly as an objective way of classifying modern chemotherapy. Furthermore, several cisplatin based regimens were used, and it is not possible to deduce to what extent the observed effects were due to the cisplatin or to the other drugs, in the combinations studied. Indeed cisplatin was used in combination with vinca alkaloids or etoposide in two thirds of trials. It is therefore not possible to recommend a particular regimen over another. Further randomised trials are needed to determine which regimens are the most effective of the modern chemotherapies studied. Trials using regimens containing vinca alkaloids or etoposide and those in the “other drugs” category also always tended to favour chemotherapy, although for these categories the confidence intervals were relatively wide and no reliable conclusions can be drawn. The meta-analysis provided no evidence that modern, cisplatin based chemotherapy was more or less effective in any particular subgroup of patients. Thus no good evidence exists that the relative effect of chemotherapy is any smaller or larger for any particular type of patient. Nevertheless, as certain types of patient may have intrinsically different prognoses and consequently differing baseline survivals, the same relative effect may provide different absolute differences in survival. For example, the hazard ratio of 0.87 for adjuvant chemotherapy would increase the survival of patients with a good prognosis from a baseline of, say, 80%, to 82% but patients with a poor prognosis from a baseline of, say, 40%, to 45% at two years. Similarly, the same observed hazard ratio of 0.87 in the locally advanced setting would increase the survival of patients with a good prognosis from a baseline of, say, 30%, to 35% and patients with a poor prognosis from 5% to 7%.
The meta-analysis suggests that modern chemotherapy regimens may provide absolute benefits of about 5% in the surgical and 2% in the radical radiotherapy setting at five years and 10% at one year in the supportive care setting. The confidence intervals are such, however, that the results are consistent with benefits of as much as 10%, 4%, and 15% respectively or with as little as a 1% detriment and 1% and 5% benefits respectively. Although modest, such improvements can, given the high incidence of lung cancer, be important in public health terms, and studies of patients' opinions of treatments for cancer have shown that many patients accept considerable toxicity in return for small improvements in survival.66 However, patients are n ot uniform intheir preferences, and the trade offs involved in choosing between more and less intensive therapy are not necessarily straightforward and warrant further study.67
IMPLICATIONS FOR RESEARCH
Extended follow up on existing trials and the inclusion of current randomised trials will add to the evidence of subsequent updates of this meta-analysis. Nevertheless, further randomised trials are still needed, especially in early disease. Moderately sized developmental trials, recruiting a few hundred patients, are needed to screen new treatment regimens and new methods of delivering treatments, thus attempting to improve long term survival. Large public health trials, recruiting thousands of patients, are also needed to assess the value of short term chemotherapies in a broad range of patients with non-small cell lung cancer. Such trials have already been launched in Europe as a consequence of this meta-analysis.
IMPLICATIONS FOR PRACTICE
Although, inevitably, meta-analyses give only average estimates of treatment effects, these are probably the best estimates on which to base treatment policy. At the outset of this meta- analysis there wasconsiderable pessimism about the treatment of non-small cell lung cancer. Although the observed effects are modest, these results offer hope of progress and show that chemotherapy may have a role in treating this disease. Some patients and clinicians would need to observe larger treatment effects than others before being convinced that chemotherapy is worth while, and undoubtedly these results will be applied differently by individual clinicians and patients around the world. Some groups may consider these results to be good enough evidence to use cisplatin based chemotherapy for certain patients. As essential drugs were not determined by this meta-analysis, however, others may need further evidence to decide whether to use chemotherapy routinely in the treatment of non-small cell lung cancer.
Just as no clinical trial can provide “prescriptions” of how to treat individual cases, neither can a meta-analysis. Ultimately, the use of chemotherapy is to be decided by the clinician and patient together and will depend on many factors, including survival, toxicity, quality of life, and economic cost of treatment. This meta-analysis provides clinicians and patients with the current most reliable estimate of average survival benefit to use as part of this decision making process.
We thank all the patients who took part in all the trials included in the meta-analysis. We also thank the following institutions that funded the Non-small Cell Lung Cancer Collaborative Group's meeting in September 1993, at which preliminary results of this meta-analysis were presented and discussed: Bristol-Myers Oncology, Bristol-Myers Squibb, Amgen, Asta-Medica, Asta-Sarget, Beecham Sevigne, Roger Bellon, Cancer Research Campaign, Chugai, Ciba-Geigy, Eurocetus, Farmitalia Carlo Erba, Glaxo France, Harold Hyam Wingate Foundation, Institut National de la Sante et de la Recherche Medicale, Ipsen Biotech, Lederle, Lilly France, Lilly Industries, Medical Research Council, Pfizer, Rhone-Poulenc, and Servier Medical. The Cancer Trials Office's secretariat thanks RichardWood, Sarah Walker, John Machin, and all the computing, data management, and secretarial staff at the office for their support throughout this project. The Institut Gustave Roussy's secretariat thanks Ben Affaied for programming support and Sylviane Iacobelli for secretarial help. We thank Linda Baulk for typing the manuscript.
The collaborative group members were: W Alberti, G Anderson, A Bartolucci, D Bell, J Blanco Villalba, O Brodin, C Cardiello, F Cartei, G Cartei, R Cellerino, C Chastang, Y Cormier, J D Cox, L Crino, J Crowley, B Dautzenberg, A Depierre, A Dietemann, R O Dillman, O Doi, R Feld, R Figlin, P A Ganz, M R Green, A Gregor, P A Helle, J E Herndon, S Hitomi, H Host, M Imaizumi, J R Jett, D Johnson, S Kaasa, H Kimura, J Klastersky, H Kondo, H Kreisman, M G Kris, K Kunishima, O Kuwahara, T E Lad, A H Laing, F Macbeth, A Masaoka, K Mattson, E Minatel, J G Mira, T Mori, C F Mountain, N Niederle, A Niiranen, E Nou, W Page, J Pater, S Piantadosi, K M W Pisters, S Pyrhonen, E Quoix, E Rapp, N P Rowell, T Sahmoud, K Sawamura, D C C Schallier, C Scott, J Simpson, M Stagg, T Teramatsu, M G Trovo, R Tsuchiya, D Tummarello, P Van Houtte, N Van Zandwijk, R G Vincent, H Wada, J E White, C J Williams, R L Woods, Y Yamaguchi.
The organisations and groups that collaborated in the meta-analysis were: Cancer and Leukemia Group B, Cercle d'Etudes Pneumologiques (Strasbourg), European Organisation for Research and Treatment of Cancer, Federation Nationale des Centres de Lutte Contre le Cancer, Finnish Lung Cancer Study Group, Groupe d'Etude et de Traitement des Cancers Bronchiques, Japan Lung Cancer Surgical Study Group, Lung Cancer Study Group, Medical Research Council, National Cancer Institute of Canada Clinical Trials Group, North Central Cancer Treatment Group,Osaka Lung Cancer Study Group, Radiation Therapy Oncology Group, Southeastern Cancer Study Group, South West Oncology Group, Study Group of Adjuvant Chemotherapy for Lung Cancer (Chibu, Japan), Swedish Lung Cancer Study Group, Veterans Administration Surgical Adjuvant Group, Veterans Administration Surgical Oncology Group, West of Scotland Lung Cancer Research Group, West Japan Study Group for Lung Cancer Surgery.
The members of the secretariat were: R Arriagada, J Cartmell-Davies, D J Girling, T Le Chevalier, S Marsoni, M K B Parmar, J P Pignon, C Rekacewicz, R L Souhami, L A Stewart, M Tarayre, A Tinazzi, V Torri.
Appendix 1
Ineligible trials—Four trials were not properly randomised, including one randomised by date of birth and two using historical controls. Three trials allowed prior chemotherapy and seven used compounds that were not considered to be established chemotherapy (mopidamol, razoxane, lonidamine, RSV (1,2-diphenyl-(alpha)β-dicetone and its superoxide), sizofiran). One early trial randomised all lung cancers but did not record histological cell type. Four trials were confounded because they used different radiotherapy doses or schedules per arm. Fourteen trials used chemotherapy only during radiotherapy or stated chemotherapy was given with the aim of radiosensitisation, or did both, including three that were also ineligible for other reasons. A full list of these trials is available on request.
Unavailable trials—Six trials were not available for analysis; two were early trials in the surgical setting,25 26 and four were from the locally advanced setting,49 50 51 52 only one of which was a modern trial using cisplatin based chemotherapy.52
Appendix 2
AOI-Udine Udine Associazione Oncologica Italiana AZ-OC Academisch Ziekenhuis Oncologic Centre (Vrije Universiteit Brussels) Buenos Aires Hospital Militar Central, Buenos Aires CALGB Cancer and Leukemia Group B CEP Cerc
le d'Etudes Pneumologiques (Strasbourg)EORTC European Organisation for Research and Treatment of Cancer FI Finsen Institute, Copenhagen FLCSG Finnish Lung Cancer Study Group GETCB Groupe d'Etude et de Traitement des Cancers Bronchiques IPCR, Chiba Institute of Pulmonary Cancer Research, Chiba, Japan JLCSSG Japan Lung Cancer Surgical Study Group LCSG Lung Cancer Study Group MCL McGill Cancer Center, Lung MRC British Medical Research Council MSKCC Memorial Sloan Kettering Cancer Center NCCTG North Central Cancer Treatment Group NCI National Cancer Institute NCIC CTG National Cancer Institute of Canada, Clinical Trials Group NRH Norwegian Radium Hospital OLCSG Osaka Lung Cancer Study Group RLW Royal North Shore Hospital, St Leonards, NSW RTOG Radiation Therapy Oncology Group SCG Swiss Chemotherapy Group SECSG Southeastern Cancer Study Group SGACLC Study Group of Adjuvant Chemotherapy for Lung Cancer, Chibu, Japan SLCSG Swedish Lung Cancer Study Group SWOG South West Oncology Group UCLA University of California at Los Angeles (Solid Tumour Study Group) VASAG Veterans Administration Surgical Adjuvant Group VASOG Veterans Administration Surgical Oncology Group WJSG West Japan Study Group for Lung Cancer Surgery WPL Working Party for Lung Cancer (Committee on Surgery and Surgery Consultants) WSLCRG West of Scotland Lung Cancer Research Group
Footnotes
-
Funding The chemotherapy meta-analysis in non-small cell lung cancer was supported by the British Medical Research Council and the Institut Gustave Roussy and by grants INSERM 921204 and ARC 2025.
-
Conflict of interest None.