Relation between maternal haemoglobin concentration and birth weight in different ethnic groups
BMJ 1995; 310 doi: https://doi.org/10.1136/bmj.310.6978.489 (Published 25 February 1995) Cite this as: BMJ 1995;310:489
- Philip Steer, professora,
- M Ash Alam, medical studentb,
- Jane Wadsworth, senior lecturerc,
- Anne Welch, research assistantd
- a Academic Department of Obstetrics and Gynaecology, Charing Cross and Westminster Medical School, Chelsea and Westminster Hospital, London SW10 9NH
- b St Bartholomew's Hospital Medical College, London EC1A 7BE
- c Academic Department of Public Health, St Mary's Hospital Medical School, London W2 1PG
- d Academic Department of Obstetrics and Gynaecology, St Mary's Hospital Medical School, London W2 1PG
- Correspondence to: Professor Steer.
- Accepted 12 December 1994
Abstract
Objective: To assess the relation of the lowest haemoglobin concentration in pregnancy with birth weight and the rates of low birth weight and preterm delivery in different ethnic groups.
Design: Retrospective analysis of 153602 pregnancies with ethnic group and birth weight recorded on a regional pregnancy database during 1988-91. The haemoglobin measurement used was the lowest recorded during pregnancy.
Setting: North West Thames region.
Subjects: 115262 white women, 22206 Indo-Pakistanis, 4570 Afro-Caribbeans, 2642 mediterraneans, 3905 black Africans, 2351 orientals, and 2666 others.
Main outcome measures: Birth weight and rates of low birth weight (<2500 g) and preterm delivery (<37 completed weeks).
Results: Maximum mean birth weight in white women was achieved with a lowest haemoglobin concentration in pregnancy of 85-95 g/l; the lowest incidence of low birth weight and preterm labour occurred with a lowest haemoglobin of 95-105 g/l. A similar pattern occurred in all ethnic groups.
Conclusions: The magnitude of the fall in haemoglobin concentration in pregnancy is related to birth weight; failure of the haemoglobin concentration to fall below 105 g/l indicates an increased risk of low birth weight and preterm delivery. This phenomenon is seen in all ethnic groups. Some ethnic groups have higher rates of low birth weight and preterm delivery than white women, and they also have higher rates of low haemoglobin concentrations. This increased rate of “anaemia,” however, does not account for their higher rates of low birth weight, which occurs at all haemoglobin concentrations.
Key messages
Key messages
Failure of the haemoglobin concentration to fall during pregnancy was associated with a five to sevenfold increase in the incidence of low birth weight and preterm birth
Routine haematinic administration in pregnancy is unnecessary on fetal grounds for most pregnancies
The mean corpuscular volume may be a better indicator of maternal iron deficiency, but this needs prospective study
Introduction
During normal pregnancy in women not given supplementary iron the haemoglobin concentration of the maternal blood falls from a non-pregnant average of about 133 g/l to an average of about 110 g/l at 36 weeks.1 The fall is steepest up to 20 weeks' gestation; the concentration remains fairly constant up to 30 weeks and then rises slightly thereafter.2 3 Thus, any estimation of haemoglobin concentration taken after 20 weeks' gestation will be reasonably representative of the fall induced by pregnancy. Whether this represents anaemia or not remains a controversial issue. The World Health Organisation in its nutritional report of 1972 suggested that anaemia was likely to be present in pregnant women when the haemoglobin fell below 110 g/l4; this will therefore include about half of all unsupplemented women. A recent paper reporting a study of 8684 pregnant women in Oxford (one of the most affluent areas of the United Kingdom) suggested that 47% were iron deficient and that this had adverse effects on the ratio of the placental weight to birth weight, which could lead to hypertension in later life.5
Supplementation of pregnant women with iron and folic acid reduces the incidence of haemoglobin <110 g/l to under 5%.1 As a result, routine prophylaxis is commonly advocated.6 7 In contrast, a recent review of 20 randomised controlled trials reported that “routine supplementation has no detectable effect on any substantive measures of either maternal or fetal outcome, [in particular] on preterm delivery, low birthweight, stillbirths or neonatal morbidity. The available data from controlled clinical trials provide no convincing case for routine as opposed to selective iron supplementation. This may be a reflection of the low prevalence of iron deficiency likely in most of the populations studied. Routine supplementation may be warranted in populations in which iron deficiency is common.”8
Most of the obstetric units in the North West Thames region have for the years over which our dataset extends (1988-91) used a common maternity information system (the St Mary's maternity information system, SMMIS) and have thus created a large database available for examination. We used it to examine the relation between the lowest haemoglobin concentration in pregnancy, birth weight, and preterm delivery after controlling for ethnic group.
Patients and methods
The total dataset comprised 157996 pregnancies resulting in a registrable birth (24 or more weeks' gestation and including live and stillbirths). Ethnic origin and birth weight were available for 153602 (4394 cases with missing data (2.8%); ethnic group missing in 4393 and birth weight in 86). Of these, 115262 were classified as white (73%), 22206 as Indo-Pakistani (14%), 4570 as Afro-Caribbean (2.9%), 3905 as black African (2.5%), 2642 as mediterranean (1.7%), 2351 as oriental (1.5%), and 2666 as other ethnic group (1.7%). Coding of ethnic group was done at booking by the midwife after consideration of the woman's family history and appearance and taking into account the woman's own views. All women whose families derived from the Indian subcontinent were classified as Indo-Pakistani, and all Chinese, Japanese, and similar races were classified as oriental. Women who could not be classified into any of the main groups (either because of an unusual race or mixed parentage) were classified as other. Data analysis was performed with SAS (Version 6) run in a Sun minicomputer with UNIX.
Gestational age was entered as the best estimate by the midwife after the birth of the baby as part of the birth notification process, by taking into account the menstrual history and early ultrasound measurements when performed. Data on gestational age were missing for 134 cases (0.08%), commonly in cases already excluded from analysis because of missing birth weight. Low birth weight was defined as <2500 g and preterm birth as before 37 completed weeks of gestation.
Lowest haemoglobin values were entered by the midwife after the birth of the baby as part of the birth notification process after inspection of all the measurements made during pregnancy. Standard practice in all the hospitals entering data was to take blood for haemoglobin estimation at booking, at the end of the second trimester (26-28 weeks), and again half way through the third trimester (34-36 weeks). Data were missing in 8442 cases (5.3%). For ease of interpretation, haemoglobin values were classified into groups each spanning 10 g/l, centred around decile values. The number of cases in white women (109050) was sufficient to allow creation of eight groups, from </=85 g/l to >145 g/l. The total data were then analysed by using the SAS procedure “logistic” to create logistic models of the relations between haemoglobin concentration and low birth weight and preterm delivery, allowing for the differences between ethnic groups and other potentially confounding variables.
Results
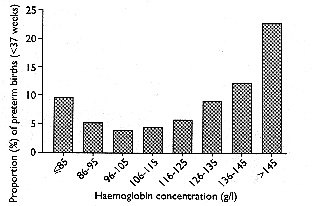
Analysis of data for white women showed that mean birth weight rose as haemoglobin concentration fell (table I), with the highest mean birth weight of 4483 g in the 86-95 g/l haemoglobin band, 545 g higher than if the lowest measurement of haemoglobin concentration was >145 g/l. Even more striking was the U shaped distribution of the rate of low birth weight by haemoglobin group (fig 1), with the incidence of low birth weight being least at 96-105 g/l. The major factor determining birth weight was the incidence of preterm delivery (fig 2), although the same pattern of relation between birth weight and haemoglobin concentration was seen even when we controlled for gestational age (table II).
Mean (SD) birth weight and incidences of low birth weight (<2500 g) and preterm births (<37 completed weeks) by haemoglobin concentration for white women in North West Thames region
Birth weight by haemoglobin concentration for 40, 38, and 36 weeks' gestation. Data for white women in North West Thames region

Incidence of low birth weight (<2500 g) by haemoglobin concentration (g/l) (data for white women only)
{kind=link}

Incidence of preterm labour (<37 completed weeks) by haemoglobin concentration (g/l) (data for white women only)
{kind=link}
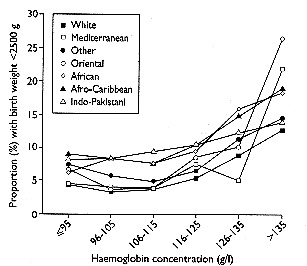
There were differences in the incidence of low haemoglobin concentration, low birth weight, and preterm delivery between the ethnic groups (table III), notably between white women and Africans, Afro-Caribbeans and Indo-Pakistanis. The logistic model, however, showed that ethnic origin had no significant effect on the relation between haemoglobin concentration and birth weight—that is, the higher rate of low birth weight in the ethnic minorities was seen at all haemoglobin concentrations (fig 3). Table IV shows the results of the logistic model after allowing for the effects of ethnic origin and other potential confounders. They show that the incidence of low birth weight was significantly raised (compared with the incidence at 96-105 g) below 85 g/l and at all concentrations of haemoglobin above 105 g/l. Exclusion of cases ending in stillbirth made no significant difference to any of the above results.
Incidence of preterm birth (<37 completed weeks), incidence of low birth weight (<2500 g), mean (SD) birth weight, and mean (SD) haemoglobin concentration for different ethnic groups
Adjusted odds ratios* (95% confidence intervals) for low birth weight (<2500 g) and preterm birth (<37 completed weeks)

Incidence of low birth weight in different ethnic groups by haemoglobin concentration (g/l)
{kind=link}
Discussion
Our study has shown the striking association of birth weight with haemoglobin concentration. Not only was there a five to sevenfold increase in preterm delivery and low birth weight if the lowest haemoglobin concentration measured during pregnancy was above 145 g/l but also the concentrations of haemoglobin associated with the highest mean birth weight (86-95 g/l) were much lower than is commonly appreciated. Birth weight is the single biggest determinant of mortality in the first year of life,9 and has therefore a strong claim to being a good indicator of the efficiency with which a woman has supported her fetus. By this criterion, a mid-trimester fall of haemoglobin concentration to about 100 g/l seems to be optimal. This probably reflects good expansion of plasma volume.10 11 Failure of the haemoglobin concentration to fall is known to be associated with up to a threefold increased risk of pre-eclampsia,12 the birth of small for gestational age infants,12 13 14 15 16 17 and preterm delivery.9 18 This effect is apparent even in relation to the haemoglobin concentration at booking, before completion of the pregnancy induced fall.12 These phenomena are probably closely interrelated. The mechanism by which expansion of the plasma volume enhances fetal growth is not known, but it may be that reduced blood viscosity favours blood flow in the low velocity flow system of the maternal intervillous space.
Haemoglobin concentrations <95 g/l seem to be remarkably harmless. Our study has shown that, although low haemoglobin concentrations are more common in some ethnic minorities, notably Africans, Afro-Caribbeans, and Indo-Pakistanis, this does not account for the increase in low birth weight and preterm labour in these groups, which persists at all haemoglobin concentrations. It may be that haemoglobin concentrations, birth weight, and length of gestation are genetically programmed to be different in these groups and are therefore physiological, although their higher rates of clearly adverse outcome such as perinatal mortality mean such a conclusion should properly be drawn only after more detailed studies of morbidity.
Many authors have drawn attention to the fact that we should be more concerned about high rather than low concentrations of haemoglobin in pregnancy,9 12 13 14 15 16 17 18 and some have decried the routine use of iron supplementation in pregnancy.19 20 21 There is a theoretical risk that increasing haemoglobin concentration might actually reduce birth weight and do harm, although the meta-analysis of the controlled trials does not support this hypothesis.8 Rather, routine supplementation seems simply to be unnecessary.
It remains possible that genuine anaemia (as opposed to a low haemoglobin value) has adverse consequences on fetal growth and long term outcome, as suggested by Godfrey et al.5 This would need more specific definition. Ferritin is not a useful measure as it falls dramatically in pregnancy irrespective of whether or not iron supplementation is given.22 Mean corpuscular volume usually remains fairly constant,22 however, and might prove to be a more robust indicator, although it can be confounded by the macrocytic effect of a simultaneous folate deficiency. Studies that link any variable proposed with fetal and neonatal function are needed lest we replace one misleading variable with another.