Management of severe malaria in children: proposed guidelines for the United Kingdom
BMJ 2005; 331 doi: https://doi.org/10.1136/bmj.331.7512.337 (Published 04 August 2005) Cite this as: BMJ 2005;331:337
- Kathryn Maitland, lecturer in tropical paediatrics (kmaitland{at}kilifi.mimcom.net)1,
- Simon Nadel, consultant in paediatric intensive care2,
- Andrew J Pollard, consultant in paediatric infectious diseases3,
- Thomas N Williams1, Wellcome Trust senior research fellow,
- Charles R J C Newton1, Wellcome Trust senior research fellow,
- Michael Levin, professor in experimental medicine4
- 1 Kenya Medical Research Institute/Wellcome Trust Programme, Centre for Geographic Medicine Research-Coast, PO Box 230, Kilifi, Kenya
- 2 Department of Paediatrics, St Mary's Hospital, London W2 1NY
- 3 Department of Paediatrics, University of Oxford, John Radcliffe Hospital, Oxford OX3 9DU
- 4 Brighton and Sussex Medical School, Medical Research Building, University of Sussex, Falmer, Brighton BN1 9PS
- Correspondence to: K Maitland
Introduction
Malaria is the most important vector borne disease worldwide. Globally it results in an estimated 400 million infections and more than 1 million deaths each year.1 Although malaria is a rare cause of hospital admission in the United Kingdom, it constitutes a substantial health threat for people travelling in endemic areas. The incidence of imported malaria is rising throughout much of the developed world, largely because of a global increase in long distance travel, immigration, and the resurgence of malaria in many tropical countries.2–4 Moreover, although Plasmodium vivax was once the most common form of imported malaria, it has since been superseded by P falciparum5—the only form of malaria that can be lethal—which now accounts for some 80% of reported cases. Around 15% of episodes of malaria occur in children aged 15 years or younger. Most of those affected are UK residents of African ethnicity who have recently visited family in endemic areas but have not taken preventive measures.5 Nevertheless, even strict compliance with preventive measures is never 100% effective, as resistance to available chemoprophylactic agents is increasing in many parts of the world.
Although most cases of P falciparum malaria in patients presenting to health services in the UK are uncomplicated, up to 10% become severe and life threatening malaria, principally because of delays in diagnosis and inadequate treatment.5 6 In uncomplicated disease, the clinical features of malaria are similar in children and adults, but in severe disease, the clinical spectrum, complications, and management differ and merit the development of separate guidelines for children. We therefore propose the following guidelines for the assessment and emergency management of children with imported malaria.
Methods
Few data are available on the clinical spectrum of severe malaria in children living in non-endemic areas. As a result, the working definitions for severe malaria that we use in this review draw heavily on studies conducted in critically sick children in Africa and on information obtained from personal archives of references, the current guidelines from the World Health Organization,7 and the Advanced Paediatric Life Support (APLS) guidelines.8 We have used the revised grading system for evidence based guidelines (GRADE).9 We graded sources available for this review as follows: randomised controlled trials are grade 1+ (low risk of bias); case-control studies, cohort studies, and observational studies are grade 2; case series are grade 3; and expert opinion is grade 4. Most sources of evidence come from grades 2 and 3. Where key recommendations are made, the strength of evidence is indicated as “grade 1-4 evidence.”
Summary points
Malaria is the most important imported mosquito borne infection in the United Kingdom
As preventive measures are never 100% effective, malaria should be suspected in any patient with “flu-like symptoms” who has travelled to malarious areas within a year
Most cases of severe malaria result from a failure to expedite prompt “same day” diagnosis and initiate appropriate treatment in patients with suspected malaria
Oral quinine and chloroquine or pyrimethamine with sulfadoxine should never be prescribed to treat falciparum malaria in children
In children, the development of one or more features of severe or complicated malaria constitutes a medical emergency
The emergency assessment of a child with severe malaria should follow the structured approach advocated by the Advanced Paediatric Life Support guidelines
If in doubt: admit, monitor closely, and seek specialist advice
Scope of these guidelines
The guidelines we propose should not be seen as a consensus statement but as recommendations to help with the initial assessment and identification of children at risk of complications, who require close monitoring or parenteral medication (box 1). Although some principles of treatment may be applicable to adults,7 some relate specifically to children (in particular those concerning volume resuscitation).
Clinical malaria
Malaria should be considered in any patient presenting with a fever who has ever travelled to an area where malaria is endemic. Although the first symptoms begin 10 days to four weeks after transmission by an infected mosquito in most children, in exceptional cases presentation can be as early as eight days or as late as one year, particularly in malaria caused by P vivax, P ovale, or P malariae or in children who have taken prophylaxis. The illness generally begins with non-specific flu-like symptoms that may include fever, cough, headache, malaise, vomiting, and diarrhoea. Supportive findings may include splenomegaly, thrombocytopenia, anaemia, and mild jaundice7; these features are, however, often absent in the early stages of disease. The presumptive diagnosis of malaria should prompt urgent referral for immediate diagnosis and management. Failure to expedite appropriate referral may lead to the development of life threatening disease. Thick and thin blood films, processed from an ethylenediaminetetra-acetic acid (EDTA) sample by the local haematology laboratory, are the mainstay of diagnosis. Direct liaison with the laboratory will ensure urgent processing. Malaria can generally be excluded by three negative thick blood films, taken 12 hours apart; however, further films are warranted if clinical suspicion remains high. Rapid diagnostic tests, such as the OptiMAL assay, are being increasingly employed. In general, these are quick and simple to use, distinguish between the major forms of human malaria, and may have some advantages over microscopy, particularly in children with low density parasitaemia, a characteristic that often applies to those who have taken prophylaxis.10 11
Box 1: Recognising severe malaria
High risk: immediate risk of dying and urgent need for supportive treatment
Depressed conscious level (any degree)
Active seizure activity
Irregular respirations or obstructed airway (pooling saliva or vomit in mouth)
Hypoxia (oxygen saturations < 95%)
Evidence of shock (systolic blood pressure < 80 mm Hg or < 70 mm Hg if patient aged < 1 year) or two or more of the following: tachycardia, increased work of breathing, cool peripheries, capillary refill time ≥ 3 seconds, temperature gradient)
Clinical evidence of dehydration
Hypoglycaemia < 3 mmol/l
Metabolic acidosis (base deficit > 8 mmol/l)
Severe hyperkalaemia (potassium > 5.5 mmol/l)
Intermediate risk: need for high dependency care
Haemoglobin < 100 g/l
History of convulsions during this illness
Hyperparasitaemia > 5%
Visible jaundice
Plasmodium falciparum in a child with sickle cell disease
Low risk: need admission for parenteral medication
Vomiting
Unable to take or comply with oral medication (see note)
Low risk: need for observation
None of the above
Admit and observe on oral treatment (see note)
Note: Oral quinine (tablets or syrup) is unpalatable for most children, hence it should never be prescribed for young children.
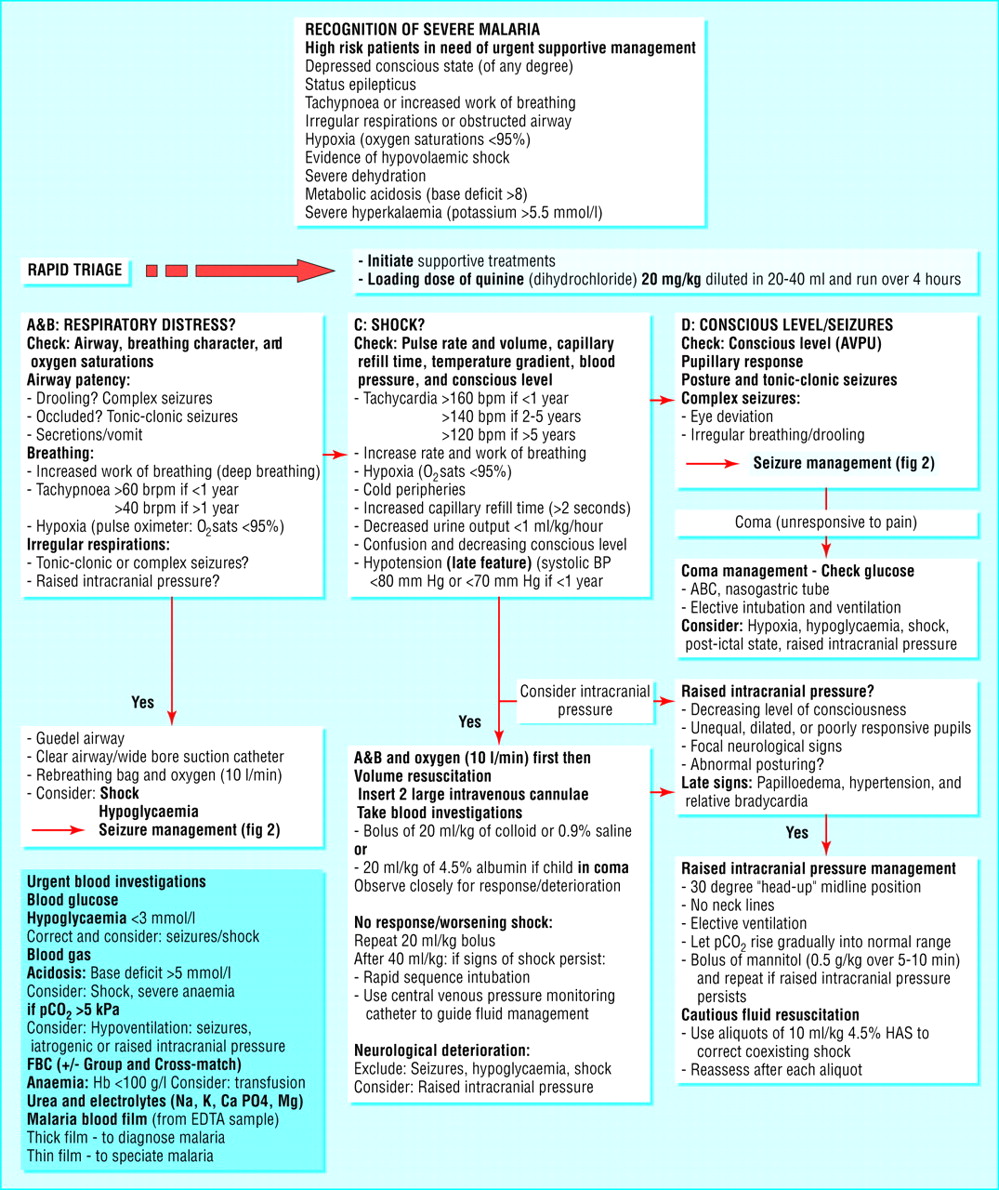
Recognition of severe malaria
Emergency assessment and management
Over the past decade, there has been increasing recognition that severe falciparum malaria is a complex syndrome affecting many organ systems and has features in common with the sepsis syndrome.12 In areas where malaria is endemic, most deaths occur within hours of admission, principally because the clinician fails to recognise impending circulatory collapse or respiratory compromise. The latter is particularly true in children with prolonged seizures. Raised intracranial pressure may complicate cases in patients presenting in a coma,13 prompting a cautious approach to volume resuscitation in such children (grade 4 evidence; fig 1).

Triage and management algorithm for severe malaria in children. (The proposed algorithm has been developed by the authors, based on APLS (UK) guidelines for the management of critically sick children and includes some principles of management practised at the Kenya Medical Research Institute unit, Kilifi, Kenya. To date, this algorithm has not been prospectively evaluated)
{kind=link}
As for any other sick child presenting to hospital, the initial management of a child with suspected malaria should be guided by a rapid, structured, triage assessment, aimed at identifying emergency and priority signs (fig 1).8 14 The sequence of clinical assessment should include the early recognition of impending respiratory failure initially, followed by the detection of shock, and neurological assessment. This approach will guide early management towards the complications that are the most commonly life threatening (fig 1). Emergency management should not be delayed while the diagnosis of malaria is confirmed. Unless an undue delay is likely, the administration of specific antimalarial drugs can usually be deferred until resuscitation treatments have been given and the diagnosis confirmed. Nevertheless, if the clinical suspicion of malaria is high, an intravenous infusion of quinine should be started empirically after initial resuscitation, even if the results are awaited. Experimental treatments, such as exchange transfusion, have no role in the initial management of children with suspected malaria and may distract attention from providing urgent and simple life saving interventions (grade 4 evidence).
Initial assessment and emergency treatments
Checking the child's airway and breathing is important as severe malaria has characteristic respiratory patterns.
Respiratory patterns of severe malaria
Irregular breathing or drooling—The presence of respiratory depression or irregular breathing should alert the clinician to the presence of complex seizures,15 iatrogenic respiratory depression (because of multiple anticonvulsant medications), or the presence of raised intracranial pressure. High flow oxygen and appropriate airway management are as important as the administration of anticonvulsants. Hypoglycaemia (blood sugar < 3 mmol/l) may precipitate seizures or posturing and should be considered in such cases.16
Respiratory distress—Tachypnoea and increased work of breathing are common complications of severe malaria in children. Studies conducted in Kenya have shown that these signs are usually associated with underlying metabolic acidosis (base deficit > 8 mmol/l) (grade 3 evidence).17 Moreover, more recent studies show that this metabolic acidosis is often associated with hypovolaemia (grade 2) and can safely be treated with volume resuscitation by using colloid or crystalloid (grade 2-3).18
Circulation
Hypovolaemic shock needs to be identified and managed if present. Acidosis (base deficit > 8 mmol/l) is a common feature of severe malaria and in children is often accompanied by features of compensated shock (grade 3 evidence).19 These include hypoxia, increased work of breathing, tachycardia, altered peripheral pulse volume, cool peripheries, prolonged capillary refill time (≥ 2 seconds), and altered consciousness (grade 3).19 Hypotension (systolic blood pressure < 80 mm Hg) complicates about 25% of cases presenting with severe acidosis (base deficit > 15 mmol/l).18 Delayed capillary refill time (≥ 2 seconds) is a reasonable prognostic indicator, especially in children with a decreased conscious level (grade 3).20
Treatment
In the absence of coma (children's Glasgow coma score < 8), we have shown that volume resuscitation with 20-40 ml/kg of either 0.9% saline or 4.5% human albumin solution safely corrects the haemodynamic features of shock and improves renal function in Kenyan children with severe malaria (grade 2 evidence),18 21 and that pulmonary oedema is a rare complication (< 0.5%; grade 2).21
Hypovolaemic shock and coma
In children presenting in coma (inability to localise pain; children's Glasgow coma score ≤ 8) we advise a more cautious approach to volume expansion. A recent phase II trial has shown that volume expansion with human albumin solution may result in a lower mortality (5%) than with saline (46%) in children with shock and coma (grade 2).21 Until further data become available from larger trials, we recommend that human albumin solution should be considered the resuscitation fluid of choice in the subgroup of children who present with coma and features of shock (grade 2-4).
Further management
Volume resuscitation should proceed cautiously in children with shock and should be stopped once the signs of circulatory failure have been reversed. Urine output of < 1 ml/kg/hour, in the absence of urinary retention or established renal failure, indicates impaired renal perfusion secondary to hypovolaemia and is a good non-invasive guide to fluid management (grade 3 evidence). For any child with persisting features of shock despite 40 ml/kg of fluid, we recommend elective intubation and ventilation, and placement of a central venous catheter to guide further fluid management (grade 2).8 Patients with severe acidosis may self ventilate their partial pressure of carbon dioxide (Pco2) to very low levels, as compensation for the metabolic acidosis (grade 3). When initiating ventilation, great care should therefore be taken to avoid a rapid rise of Pco2, even to normal levels, before acidosis has been partly corrected (grade 4). If the patient is still shocked or if the shocked state returns then treatment of shock should take priority, since cerebral perfusion depends on an adequate blood pressure (grade 4).
Disability: coma
Impaired consciousness—Rapid assessment of neurological function should include an assessment of the conscious level using either the AVPU scale (Alert, responds to Voice, responds to Pain, or Unresponsive)8 or children's Glasgow coma scale8 are adequate; pupillary size, and reaction to light, in addition to observing the child's posture and convulsive movements, if present. Other infections of the central nervous system or intracranial haemorrhage, rather than malaria, should be considered as alternative diagnoses in a child with neck stiffness or a full fontanel.22 23 Hypoglycaemia (blood sugar < 3 mmol/l) may precipitate coma and should be excluded. The cardinal features of cerebral malaria are impaired consciousness, convulsions, abnormal neurological signs, and opisthotonic posturing.7 Only in a small proportion of children do these features suggest raised intracranial pressure (grade 3 evidence).24–26 Recent studies in children in Malawi have shown a retinopathy that is peculiar to severe malaria and consists of patchy whitening of the retina in the macular and extramacular areas, pale opacification of retinal vessels, and white centred haemorrhages. In children who die, a correlation between the density of haemorrhages in the retina with their density in the brain has been found.24
Treatment
Initial management should include maintenance of the airway, support of breathing, and immediate correction of hypoglycaemia and volume deficits. Children who remain unconscious (children's Glasgow coma score ≤ 8) or have features suggestive of raised intracranial pressure warrant elective intubation and ventilation. For children with seizures, the decision to ventilate should be delayed if they are in a postictal state, as long as the airway is patent and respiration is not compromised.

Seizure management algorithm (recommended in the APLS (UK) guidelines)
{kind=link}
Further management
No adjunctive therapies have shown any benefit in treatment of children in coma. Repeated seizures and motor posturing movements are common in children in coma. Their relation to raised intracranial pressure has not been established (grade 3 evidence); nevertheless, because of the potential risk of raised intracranial pressure, ventilation should aim to optimise the Pco2 in the normal range, as there is no evidence that hyperventilation is beneficial in raised intracranial pressure (grade 4). Most patients will regain full conscious level over the following 48 hours.
Management of seizures
Seizures are common in severe childhood malaria. Most present as tonic-clonic convulsions, but 25% are subtle or subclinical (grade 2-3 evidence), commonly manifesting as eye deviation, an irregular respiratory pattern, or drooling.14 Initiating high flow oxygen and appropriate airway management are as important as the administration of anticonvulsant drugs. Hypoglycaemia may precipitate seizures or posturing and should be considered in such cases (grade 3). After establishing an adequate airway and respiratory support, specific management should follow the evidence based consensus guideline advocated by the Advanced Paediatric Life Support Group (fig 2).8 Seizure prophylaxis is not recommended. A recent trial of prophylactic phenobarbital, at a loading dose of 20 mg/kg given intramuscularly, increased mortality in Kenyan children with cerebral malaria. Mortality was greatest in those receiving two or more doses of diazepam, which may have caused respiratory depression in these unventilated children (grade 2).24 Nevertheless, the safe use of anticonvulsants in the setting of a modern paediatric intensive care setting is likely to differ greatly from that in African centres where ventilatory support is unavailable and should follow the standard algorithm (fig 2).
Raised intracranial pressure
Monitoring of intracranial pressure and postmortem studies in two separate series of malaria patients with a prolonged and complicated course have shown that brain swelling is a major feature in fatal cases (grade 3 evidence).24 25 Nevertheless, in most cases, signs suggestive of raised intracranial pressure developed in the later stages of the illness (grade 3). Signs include a declining conscious level, focal neurology including unequal, dilated, or poorly responsive pupils, and abnormal posturing.8 28 29 Papilloedema and the combination of hypertension and relative bradycardia are late findings in acute raised intracranial pressure.25 Unilateral sluggish or absent pupillary responses are the only reliable signs (grade 3).29 We advocate caution in the diagnosis of raised intracranial pressure in children in the peri-ictal state, where pupillary signs and conscious level may be misleading (grade 4).
Treatment
The development of features suggestive of raised intracranial pressure should be considered a medical emergency and should be treated by the rapid induction of anaesthesia, tracheal intubation, mechanical ventilation, and close, and frequent monitoring of blood gases (grade 4 evidence).8 To stabilise cerebral blood flow, Pco2 should be kept within the normal range. However, in patients with hyperventilation and low initial Pco2, ventilation should allow the Pco2 to rise to a normal range more gradually. Mannitol (0.5 mg/kg) infused rapidly over five to 10 minutes may be effective in lowering the intracranial pressure, but its short term effect means that repeated doses are often necessary (grade 3).28 Other forms of osmotherapy for the management of raised intracranial pressure, such as hypertonic saline, have not been evaluated in children with severe malaria. Steroids are not recommended as their effect on raised intracranial pressure remains unclear and their use may adversely affect outcome (grade 3).7
General management
Antimalarial medication
Parenteral quinine remains the antimalarial treatment of choice for patients with severe falciparum malaria (table 1). An initial loading dose (20 mg salt/kg) should be given over four hours, followed by 10 mg/kg every eight hours (infused over four hours). Clinicians should be aware that, because of the mode of action of quinine, peripheral parasitaemia may not decrease and might even continue to increase during the first 24 hours of treatment. This rarely indicates quinine resistance in children presenting from Africa; however, resistance has been reported in Southeast Asia, and advice on appropriate alternative treatments should therefore be sought from one of the regional centres if children presenting from that region fail to respond appropriately within the first few days of treatment.
Antimalarial treatments
Table 2 Glucose and electrolytes: corrective measures
Box 2: Anticipated complications
Very common
Hypoglycaemia (blood glucose < 3 mmol/l): often correlates with disease severity. Maintenance fluids containing 5-10% glucose should prevent this complication
Hyperpyrexia: increases the risk of convulsions in children and should be treated with antipyretics or tepid sponging. Ibuprofen is superior to paracetamol for reducing fever (grade 3 evidence); the dose should be reduced in cases complicated by impaired renal function.
Seizures and posturing—see under seizure management
Common
•Electrolyte derangement:
Hyperkalaemia may complicate cases with severe metabolic acidosis at admission. Treatment should follow standard Advanced Paediatric Life Support guidelines
Hypokalaemia, hypophosphataemia, and hypomagnesaemia are often apparent only after admission after metabolic derangements have been corrected (grade 3). Serial monitoring of plasma electrolytes is suggested, correction should follow the recommendations given by the Advanced Paediatric Life Support guidelines (table 2)
• Metabolic acidosis:
Resolves with the correction of hypovolaemia and treatment of anaemia by adequate blood transfusion
No evidence to support the use of sodium bicarbonate (grade 3)
Dichloroacetate reduces lactic acidosis in African children, but effect on mortality unknown (grade 2)
• Severe malaria anaemia:
Most patients will experience some reduction of haemoglobin and do not require transfusion. The decision to transfuse should be influenced by the parasitaemia level and clinical condition of the patient (grade 3)
Transfuse if the haemoglobin concentration falls below an absolute value of 100 g/l (grade 4)
Uncommon
Secondary bacterial infection may occur (grade 3) and empiric broad spectrum antibiotics are warranted—such as ceftriaxone 100 mg/kg/day
Coagulation activation: Bleeding is rare despite the customary thrombocytopenia of severe malaria (platelet counts often < 50×109/l; grade 3)
At the time of writing these guidelines, injectable artesunate, an artemesinin based malaria drug, is being evaluated in large multicentre trials in Southeast Asia and Africa. Until the results of these trials are available, intravenous quinine remains the drug of choice for patients with severe malaria and should be prescribed for seven days. However, in children who have fully recovered clinically, the course of intravenous quinine may be shortened by switching to a full oral course of an appropriate non-quinine medication (grade 4 evidence). Because of its bitter taste, oral quinine is often associated with poor compliance in children, and we therefore strongly advocate alternative oral preparations such as mefloquine (Lariam), proguanil with atovaquone (Malarone), or artemether with lumifantrine (Riamet and Coartem) to achieve full parasitological cure.
Glucose and electrolytes
Hypoglycaemia is a common complication of severe malaria.7 16 Moreover, as quinine stimulates insulin secretion, hypoglycaemia may also result from quinine therapy. Blood glucose concentrations should therefore be monitored serially. Derangements of electrolytes, particularly hypokalaemia,30 hypophosphataemia, and hypomagnesaemia are common31; serial monitoring and correction are advised (grade 3 evidence; table 2).
Anticipated complications and management are covered in box 2.
Role of exchange transfusion
Exchange transfusion has been advocated for hyperparasitaemia (> 10%) in adult intensive care settings, despite little evidence to indicate an improved outcome (grade 2 evidence).32 Even when parasitaemia exceeds 25%, most children respond rapidly to the management outlined above. In children with persistent acidosis and multiorgan impairment who are not responsive to these resuscitation treatments, exchange transfusion may be considered as a means of rapidly reducing the level of abnormally rigid red cells, or parasite toxins (grade 2). This treatment, however, remains experimental.
Additional educational resources for health professionals and patients
All sources provide information on health risks for international travel, including information on malaria risks for specific countries or regions, on antimalarial prophylaxis, and on up to date health surveillance
UK based
Fit For Travel (http://www.fitfortravel.scot.nhs.uk/)—public access website provided by the NHS (Scotland), which gives travel health information for people travelling abroad from the UK
Health Protection Agency (http://www.hpa.org.uk/)—An independent body that protects the health and wellbeing of everyone in England and Wales. The agency has a critical role in protecting people from infectious diseases
National Travel Health Network and Centre (http://www.nathnac.org/)—Funded by the Department of Health to promote clinical standards in travel medicine (see, in particular, the Yellow Book, www.nathnac.org/yellow_book/01.htm)
Non-UK based
World Health Organization International Travel and Health (www.who.int/ith/en/)—offers guidance on the full range of health risks likely to be encountered at specific destinations and associated with different types of travel
Centers for Disease Control and Prevention, Travelers' Health (www.cdc.gov/travel/)—US based resource
Treatment advice
• Telephone numbers of the main UK tropical centres that may be consulted by health professionals are available in the British National Formulary under “Antimalarial treatments”
Further management and prognosis
Frequent reassessment and close monitoring of critically ill children will identify most complications. Even in the absence of raised intracranial pressure, coma may persist for several days. Unlike sepsis, severe malaria is rarely complicated by refractory shock, perhaps because of the lack of gross capillary leak syndrome (grade 3 evidence). Nevertheless, complications of fluid overload, including pulmonary oedema or raised intracranial pressure, should be monitored closely. Raised intracranial pressure may develop late in a proportion of children, especially those presenting in a coma. Some 10% of African children with cerebral malaria develop persisting neurological sequelae (grade 3)1 33 and an even greater proportion are left with learning and language disorders34; nevertheless, most experience has been drawn from a population for whom use of and access to modern intensive care facilities are not possible.
We thank the numerous scientific colleagues we have worked with over the years for clinical guidance and illuminating discussions. We specifically thank several colleagues including Suzanne Anderson, David Pace, Robert Tasker, and Shunmay Yeung for their helpful feedback on earlier drafts of these guidelines, and Chris Whitty for constructive comments during the review of this manuscript.
Footnotes
-
Contributors All authors participated in editing the final version of the guidelines. KM conceived the need for paediatric guidelines, developed the consortium, and wrote the initial and final drafts of the guidelines. TNW helped with the literature search and provided specialist input on the management of malaria. CRJCN provided specialist input pertaining neurological manifestations and treatment of severe malaria. SN provided specialist advice on the management of critically ill children and edited the guidelines such that they are appropriate to general practice in most paediatric intensive care units in the United Kingdom. AJP conceived the need for paediatric guidelines, helped with the initial draft, and ensured that the guidelines provided clear advice for frontline medical personnel. ML provided specialist infectious disease and intensive care advice and edited several versions of the guidelines and is the guarantor.
-
Competing interests None declared.