Making decisions about hormone replacement therapy
BMJ 2003; 326 doi: https://doi.org/10.1136/bmj.326.7384.322 (Published 08 February 2003) Cite this as: BMJ 2003;326:322
- Janice Rymer (janice.rymer{at}kcl.ac.uk), senior lecturera,
- Ruth Wilson, professorb,
- Karen Ballard, director of postgraduate studiesc
- a Guy's, King's and St Thomas's School of Medicine, Guy's and St Thomas's Hospital Trust, London SE1 7EH
- b Department of Family Medicine, Queen's University, Kingston, Ontario, Canada
- c Department of General Practice and Primary Care, Guy's, King's and St Thomas's School of Medicine, King's College London SE11 6SP
- Correspondence to: J Rymer, Department of Obstetrics and Gynaecology, St Thomas's Hospital, London SE1 7EH
Since hormone replacement therapy was introduced 70 years ago, a steady flow of studies has produced evidence of both harmful and beneficial effects. Recent British studies have shown that 60% of women aged 51–7 years have taken hormone replacement therapy,1 with 45% having tried it by the time they are 50.2 In the United States, about 38% of postmenopausal women take hormone replacement therapy. In 2000, 46 million prescriptions were written for Premarin (conjugated equine oestrogens), making it the second most frequently prescribed drug in the United States.3
Women are increasingly encouraged to participate in making decisions about hormone replacement therapy. However, the complexity and uncertainty of information about the treatment can make it difficult for women to make a decision, increasing their reliance on medical advice.4 The publication of the heart and oestrogen-progestin replacement study (HERS)5 and women's health initiative (WHI)6 study, both of which found adverse effects, has added to the confusion. In this article, we define who should be offered hormone replacement therapy and why, describe the reasons why women may wish to take hormone replacement therapy, and clarify the advantages and disadvantages of treatment.
Summary points
Hormone replacement therapy can improve the quality of life of women with hypo-oestrogenic symptoms
Long term hormone replacement therapy should be offered to women at high risk of osteoporosis or with established osteoporosis
Hormone replacement therapy should not be offered for prevention of cardiovascular disease or to women with a high risk of cardiovascular disease
Long term treatment is associated with increased incidence of breast cancer
Women should be counselled about the risks, benefits, and uncertainties of hormone replacement therapy before deciding to start or stop treatment
Sources and selection criteria
We based this article on recent publications on hormone replacement therapy and our extensive experience in running a menopause clinic, prescribing hormone replacement therapy, and researching into hormone replacement therapy.
Benefits and risks of hormone replacement therapy
The main reasons for prescribing hormone replacement therapy are relief of menopausal symptoms and prevention or management of osteoporosis. Some evidence also exists that it may have a role in primary and secondary prevention of cardiovascular disease, prevention of colorectal cancer, and prevention of Alzheimer's disease. Hormone replacement therapy seems to be associated with an increased risk of breast cancer, myocardial infarction, cerebrovascular disease, and thromboembolic disease.
Symptoms of menopause
Experiences of menopausal symptoms vary widely and have been found to relate to factors such as social class,7 ethnicity,8 and culture.9 The most common reason motivating women to take hormone replacement therapy is the relief of menopausal symptoms. 2 10–12
Although women report that hormone replacement therapy improves various menopausal symptoms,13 randomised clinical trials have proved that it is effective for only vasomotor14 and urogenital symptoms.15 A “domino” effect may occur—for example, relieving hot flushes may improve sleep, which may improve mood. In addition, oestrogen has been found to improve quality of life in the short term.16
Osteoporosis
After the age of 35 years, men and women start to lose around 1% of bone mass each year. However, bone loss is accelerated during the first three to four years after the menopause. A third of women over the age of 50 years sustain a fracture, with osteopenia a major risk factor.17 Women with specific risk factors (box) should be offered bone density screening (preferably dual x ray absorptiometry) and those with a low bone mass offered hormone replacement therapy or other antiresorptive treatment. Follow up bone density measurements can be used to adjust the dose of hormone replacement therapy and ensure women maintain adequate bone mass.
Royal College of Physicians guidance on risk factors for osteoporosis
Premature menopause (before the age of 40)
Family history of osteoporosis
Taken steroids for more than 6 months
Premenopausal amenorrhoea for more than 6 months (due to low body mass index or excessive exercise)
Liver, thyroid, or renal disease
History of excessive alcohol intake
Taken gonadotrophin releasing hormone analogues for more than 6 months
Randomised controlled trials have shown that hormone replacement therapy reduces bone loss at clinically relevant sites such as the spine (reduced by 50%) and neck of femur (by 30%). In addition, a review of randomised trials reported a significant reduction in fractures in women taking hormone replacement therapy. This effect, however, may be less in women older than 60.18 The WHI study was the first randomised controlled trial to show a reduction in hip fracture with hormone replacement therapy.6 Bone loss resumes within a year after stopping hormone replacement therapy, however, and bone turnover rises to the level of that in untreated women within three to six months.
Non-hormonal therapies such as bisphosphonates and selective oestrogen receptor modulators are as effective as hormone replacement therapy for preventing fractures. These are a good treatment for women with low bone mineral density who do not have problematic hypo-oestrogenic symptoms, have contraindications to hormone replacement therapy, or do not wish to take it.
Cardiovascular disease
Cardiovascular disease rarely affects women before the menopause, strongly implicating oestrogen deficiency in the aetiology of the disease. Observational studies have reported that oestrogen decreases morbidity and mortality from coronary heart disease by 30-50%.19 This benefit is reduced, however, by the addition of progestogens, which are needed to prevent endometrial disease.20 Indeed, the WHI and HERS double blind, randomised, placebo controlled trials have shown that continuous treatment with 0.625 mg of conjugated equine oestrogens plus 2.5 mg of medroxyprogesterone increases the risk of heart disease events by 29% (37 v 30 per 10 000 person years) and stroke by 41% (29 v 21 per 10 000 person years). 5 6 21
The HERS study investigated the risk of events among 2763 postmenopausal women with documented coronary heart disease.5 During a mean of 4.1 and 6.8 years of follow up there were no significant differences between the hormone and placebo groups in coronary heart disease events (non-fatal myocardial infarction plus coronary heart disease related death) or in any secondary cardiovascular outcome.22 However, further analysis showed a significant time trend, with more coronary heart disease events in the hormone group than in the placebo group during the first year of treatment and fewer in years 3-5.
The WHI study examined the effect of hormone replacement therapy in 16 608 healthy menopausal women.6 The study had to be stopped prematurely when the risk of invasive breast cancer exceeded the stopping boundary. The primary outcome was coronary heart disease (non-fatal myocardial infarction and death from coronary heart disease) with invasive breast cancer as the primary adverse outcome. Women in the oestrogen-progestogen group had an absolute excess risk of 7/10 000 person years for coronary heart disease events and 8/10 000 for stroke. Most of the excess events were non-fatal. Another arm of the study continues to compare oestrogen alone with placebo, and this will help determine whether the progestogen is causing the harm.
The recommendation after both these studies was that postmenopausal hormone replacement therapy should not be used for reducing risk of coronary heart disease. The results of these studies cannot be extrapolated to other forms and routes of administration of hormone replacement therapy since different progestogens have significantly different effects.
Thromboembolic disease
Studies generally show an increased risk of deep vein thrombosis and pulmonary embolus in women taking hormone replacement therapy.23–25 The absolute risk in current users is small, with estimates of 16 and 23 excess cases per 100 000 women a year for all venous thromboembolism and 6 per 10 000 women a year for pulmonary embolism. Women taking hormone replacement therapy have twice the risk of venous thromboembolism compared with non-users.
The increase in risk seems to be greater in the first year of use, with an odds ratio of 4.6 (95% confidence interval 2.5 to 8.4) during the first six months. Hormone replacement therapy may therefore be unmasking an underlying thrombophilic tendency. The risks of venous thromboembolism with hormone replacement therapy are likely to be greater in women with predisposing factors such as a family history of thromboembolic disease, severe varicose veins, obesity, surgery, trauma, or prolonged bed rest, and age is an important risk factor.
Colorectal cancer
Observational studies have consistently suggested that hormone replacement therapy reduces the risk of colorectal cancer.26 The WHI study, however, was the first randomised controlled trial to confirm this, reporting six fewer colorectal cancers each year in every 10 000 women taking hormone replacement therapy compared with the placebo group.6 The mechanisms behind this reduction in colorectal cancer are not clear.
Breast cancer
A serious concern for women taking long term hormone replacement therapy is the reported increased risk of breast cancer.27 Several epidemiological studies have reported an increased risk of breast cancer, and the risk is higher with oestrogen-progestogen combinations than with oestrogen alone.
A large meta-analysis of data from 51 observational studies reported that the risk of breast cancer increased by 2.3% for every year of use of hormone replacement therapy.28 This increased risk does not become significant unless hormone replacement therapy is taken for more than five years, when the relative risk is 1.35. The cumulative incidence of breast cancer in women aged 50–70 years in women who have never used hormone replacement therapy is about 45 cases per 1000 women. The excess risk translates to two extra cases of breast cancer for every 1000 women taking hormone replacement therapy for five years, six extra cases for every 1000 women taking it for 10 years, and 12 extra cases for every 1000 taking it for 15 years.
Although the incidence of breast cancer increased over time, the study did not show an increase in mortality. Possible reasons for this include increased health surveillance and a tendency for less aggressive, well differentiated tumours in women taking hormone replacement therapy. The risk of breast cancer falls after stopping hormone replacement therapy and returns to baseline within five years.
Because the WHI study stopped early, it could not examine the risk of death from breast cancer. However, it did confirm the excess risk of breast cancer with hormone replacement therapy. There was a 15% increase in invasive breast cancer in women taking oestrogen plus progestogen for less than five years and a 53% increase in those taking it for more than five years. The study concluded that for every 10 000 women taking oestrogen and progestogen, there would be eight more cases of invasive breast cancer a year.
Endometrial cancer
The increased incidence of endometrial hyperplasia and endometrial cancer associated with unopposed hormone replacement therapy has been established since the 1970s. Progestogen decreases the excess risk of endometrial cancer but protection decreases with long term use of sequential regimens, and the risk is significantly increased after five years of use.29–31 The continuous progestogen regimens correct complex hyperplasia that arises during sequential therapy and keeps the endometrium suppressed in the longer term.32
Ovarian cancer
Although concerns have been raised about an association between hormone replacement therapy and ovarian cancer, studies have not shown a consistent increase in risk. For example, a recent study reported an increased risk of ovarian cancer in women taking postmenopausal oestrogen replacement therapy for more than 10 years (relative risk 1.8, 95% confidence interval 1.1 to 3.0) but no increase in risk of ovarian cancer among users of continuous combined hormone replacement therapy.33
Principles of prescribing
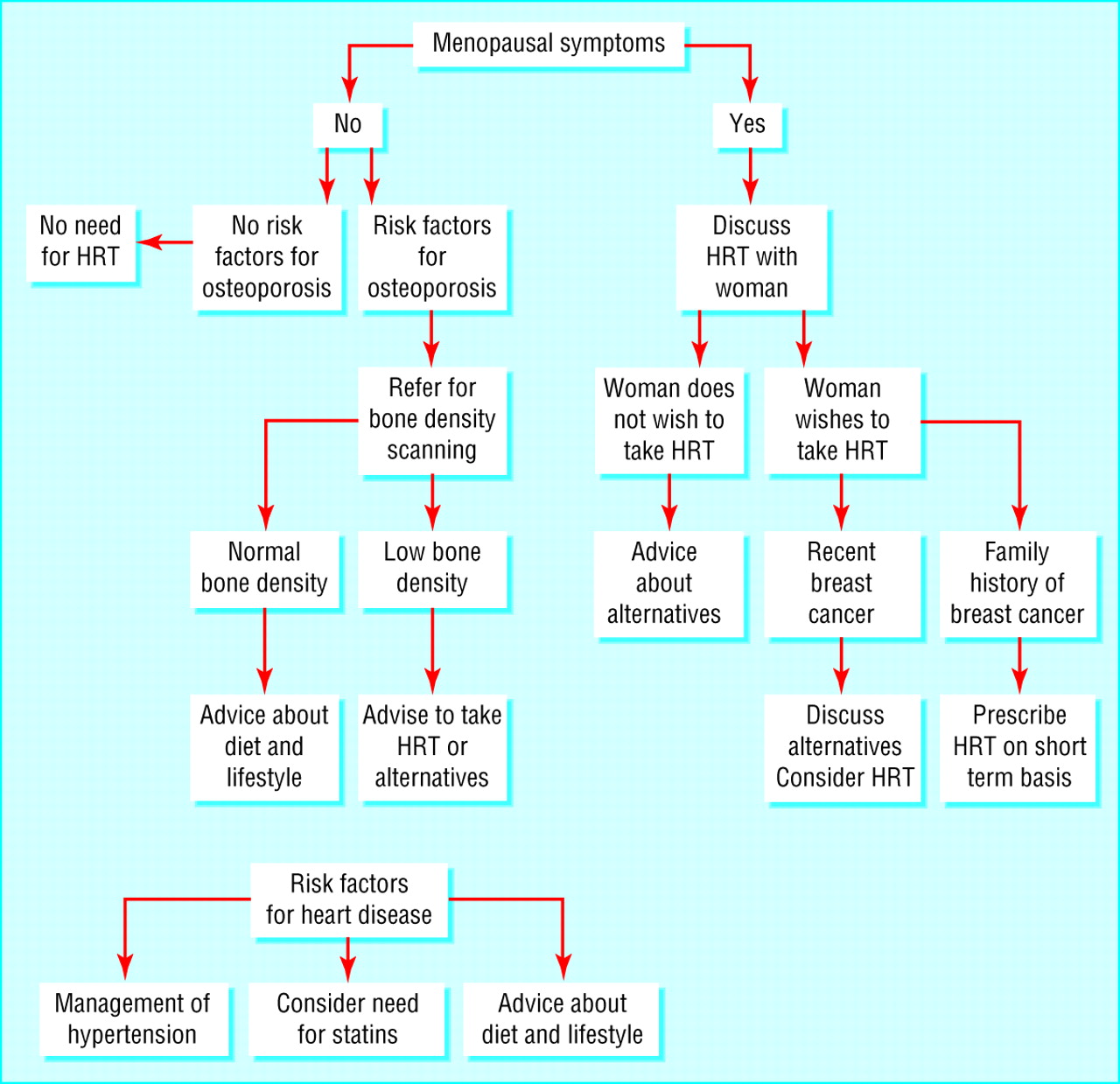
The principles of prescribing require that drugs are efficacious, acceptable, and cost effective and have a reasonable risk-benefit ratio. The figure shows a flowchart to help decide who should be offered hormone replacement therapy.

Flowchart showing who should be offered hormone replacement therapy (HRT)
{kind=link}
Ongoing research
Women's health initiative (WHI) study—Exploring the association between hormone replacement therapy and the development of breast and colon cancer, heart disease, and osteoporosis. The continuous combined hormone replacement therapy arm has been discontinued, but the oestrogen alone arm continues (10 739 postmenopausal women, first results due in 2005)
Women's hormone intervention secondary prevention study—Investigating the efficacy, safety, and tolerability of hormone replacement therapy after acute myocardial infarction in postmenopausal women (125 women, results due in 2003)
Symptomatic perimenopausal women
Women who present with hot flushes or irregular periods may be offered sequential hormone replacement therapy—that is, oestrogen continuously with progestogen for 12–14 days of each cycle. This will relieve symptoms of oestrogen deficiency and control the cycle. Treatment for one to two years is likely to improve quality of life with minimal risk.
Symptomatic postmenopausal women
The risk-benefit ratio for short term use in symptomatic postmenopausal women is weighted towards benefit. However, the situation is less clear for long term use. Women without a uterus need only oestrogen. This will relieve hot flushes, improve urogenital symptoms, and protect against bone loss but increase the risk of breast cancer, stroke, thromboembolic disease, and, in some cases, cardiovascular disease. Long term use may protect against colorectal cancer and delay the onset of Alzheimer's disease.

Additional educational resources
British Menopause Society (http://www.the-bms.org/)
North America Menopause Society (http://www.menopause.org/)
Australian Menopause Society (http://www.menopause.org.au/)
European Menopause and Andropause Society (http://www.emasonline.org/)
International Menopause Society (http://www.imsociety.org/)
Information for patients
Women's Health (http://www.womenshealthlondon.org.uk/)—A charity that provides information on many aspects of women's health
Women's Health Concern (http://www.womens-health-concern.org/)—A charity organisation that provides advice and information to women about different health issues. In addition to producing books and leaflets, they provide telephone advice
National Osteoporosis Society (http://www.nos.org.uk/)—Provides free telephone advice and information on many aspects of osteoporosis and can put you in touch with local support groups
British Heart Foundation (http://www.bhf.org.uk/)—Provides support and information about the causes, treatment, and prevention of heart disease
Breast Cancer Care (http://www.breastcancercare.org.uk/)—A UK charity that offers information and support to people affected by breast cancer
National Women's Health Information Centre (http://www.4woman.gov/)—Website of the office of women's health in the US Department of Health and Human Services
Ballard K. Understanding menopause. Chichester: John Wiley, 2003
Women with a uterus can take sequential hormone replacement therapy (oestrogen continuously and progestogen for 12–14 days of each month), continuous combined oestrogen-progestogen, or oestrogen plus the progestogen containing intrauterine system, which delivers progestogen locally to the endometrium. Women who opt for oestrogen replacement therapy plus the intrauterine system may avoid the apparent negative effects of progestogen on the breast and cardiovascular system. The intrauterine system is not licensed in Britain for this indication, but there is considerable evidence of the safety and efficacy, and it is widely used for this purpose, particularly in Scandanavia.34
Symptomatic women with premature menopause
Women experiencing the menopause before the age of 40 should be advised to start long term hormone replacement therapy. As these women have not been exposed to the normal length of natural oestrogen, the health risks associated with hormone replacement therapy are not thought to apply until they reach the normal postmenopausal age. However, these women may need much higher doses of hormone replacement therapy to maintain their bone mass, particularly if they are younger than 30.
Women with urogenital symptoms
Systemic hormone replacement therapy is not recommended for women with urogenital symptoms alone. Symptoms such as vaginal dryness can be adequately treated with local preparations—for example, creams, pessaries, or rings.
Women with temporary ovarian failure
Gonadotrophin releasing hormone analogues are used to suppress ovarian function in women with endometriosis and breast cancer. Use for more than three months results in appreciable bone loss, which may increase the risk of subsequent osteoporosis. Women taking these drugs for more than six months should therefore be given hormone replacement therapy to prevent bone loss. Since the women are premenopausal and their ovarian function is only temporarily suppressed, hormone replacement therapy should not increase their health risk.
Women who should not be offered hormone replacement therapy
Hormone replacement therapy is difficult to justify in women with no oestrogen deficiency symptoms and no risk factors for osteoporosis. Women who have heart disease, breast cancer, and oestrogen provoked venous thromboembolism should be discouraged from taking hormone replacement therapy unless there are other strong indications. Women at high risk who are keen to take hormone replacement therapy should be referred to a specialist menopause clinic.
Footnotes
-
Competing interests JR has received research funding from Organon, consultancy fees from Organon, Wyeth, Janssen-Cilag, and Pfizer, and been sponsored to attend conferences by several drug companies.