Article Text

Abstract
BACKGROUND The rise in the incidence of Crohn's disease (CD) suggests the role of an environmental factor in the development of the disease in susceptible individuals. Perinatal exposure to infection has been proposed as such an environmental factor.
AIM To investigate the influence of birth date on the development of CD in later life.
PATIENTS AND METHOD Four registers of patients with CD, diagnosed from 1972 to 1989, were combined, and data from 1624 patients were examined. The birth dates of CD patients were compared with national birth figures for three decades (1941–50, 1951–60, and 1961–70) to avoid temporal changes in birth trends, and year of birth was compared with epidemic measles years between 1951 and 1967. Risk ratios with 95% confidence intervals (CI) and χ2 tests were performed.
RESULTS There were marginal differences between the birth dates of the CD patients and those predicted from the general population. Further analysis of both season of birth and year halves revealed a very weak association with the first half of the year (relative risk 1.14 (95% CI 1.01–1.30)). There was no association between developing CD and birth during measles epidemics between 1951 and 1967.
CONCLUSIONS In utero or perinatal exposure to seasonal environmental factors are unlikely potential aetiological agents in the later development of CD.
- measles
- birth date
- Crohn's disease
- epidemiology
Abbreviations used in this paper
- CD
- Crohn's disease
- IBD
- inflammatory bowel disease
- CI
- confidence intervals
- RR
- relative risk
Statistics from Altmetric.com
The aetiology of inflammatory bowel disease (IBD) remains unknown. In Cardiff, over a 50 year period, the incidence of Crohn's disease (CD) has increased from 0.18 cases/105population/year to 8.3 cases/105/year.1 This rise could imply an environmental factor to which genetically susceptible people have been exposed. Researchers from the Royal Free Hospital have suggested that perinatal or in utero factors are important aetiological factors in the development of CD. They proposed that early exposure to wild-type or live attenuated measles virus may be of aetiological importance.2-4
We hypothesise that if IBD is due to early exposure to infectious agents, or other environmental factors, then season of birth will be associated with an increased risk of developing IBD because perinatal or in utero exposure to environmental factors may be seasonal. In the present study, we have assessed the association between these factors and IBD.
Patients and methods
We combined four registers of patients with CD who were diagnosed between 1972 and 1989: two registers were hospital based, from Cardiff and Derby, and two were community based, from Leicestershire and Tower Hamlets.5-10 The Tower Hamlet and Leicestershire databases were collected using identical methods.5-7Cases were identified retrospectively from both hospital and community sources. The case notes of all potential cases were obtained and examined by two investigators using a standard proforma, based on Lennard-Jones' criteria of case definition.11
The Cardiff register was established in 1934 and is now computerised. Initially, this was a hospital based register using the diagnostic coding of all inpatients and outpatients but this has been supplemented with general practitioner cases using a questionnaire8 ,9and is essentially a community based register. The notes of these patients are examined and included only if they reach strict diagnostic criteria. Data from Derby are hospital based.10 Data were recorded retrospectively from 1951 until 1978 inclusively, and then prospectively. The records of the hospital activity analysis, histopathology, and the two consultant gastroenterologists in Derby were examined. The case notes identified were examined and patients were included only if strict diagnostic criteria were achieved. To allow comparison between all four registers, only patients diagnosed between 1 January 1972 and 31 December 1989 were analysed. Complete data were available for 1624 patients with CD: 670 in Leicestershire, 426 in Derby, 424 in Cardiff, and 104 in Tower Hamlets (table 1). The month of birth distribution of the CD cases was compared to that expected from population statistics.12 To avoid temporal changes in birth date distribution, three separate decades (1941–50, 1951–60, and 1961–70) were analysed during which time 968 CD patients were born. χ2 tests were performed and relative risk (RR) and 95% confidence intervals (CI) calculated using confidence interval analysis software.13
Month of birth for Crohn's disease (CD) patients in four inflammatory bowel disease registers
The preferred model that fits well many seasonal and other cyclical trends is known as the von Mises distribution,as described by Mardia.14 Using this model, the number of cases born in each month is fitted by a constant and a sinusoidal term, with time of peak fitted to the observed data. The model has two degrees of freedom, which is the minimum that is meaningful; one of the fitted parameters represents the time of the peak, the other the amplitude. In this instance, because the numbers of births were different at different times of the year (not only because the lengths of the months are unequal), the number of cases in each birth month category were first adjusted slightly so that they still added up to the correct total (968) but took account of the expected values.
Data on yearly incidence of measles was obtained from the Public Health Laboratory Service from 1940–1997.15 During the period 1951–67, measles notifications exhibited an almost perfect biennial pattern with over 450 000 notifications in odd years and less than 400 000 in even years. CD cases were compared between odd and even birth years in this period, taking account of changing numbers of total births per year. The relative risk in epidemic years relative to non-epidemic years was calculated (with 95% CI).16
Results
Results are displayed in table 2. There appeared to be an excess of births in spring, especially in the 1940s. Analysis of individual months revealed no statistically significant differences from expected totals. Analysis using the von Mises distribution gave an estimated peak at 102° relative to a turn of year reference point (that is, 12 April; χ2 2=4.11, p=0.13).
Month of birth for the general population and Crohn's disease (CD) by decade (1941–50; 1951–60; 1961–70)
When the data were analysed by season (table 3) and individual decades summated, the ratios of observed to expected CD births were 1.088, 1.042, 0.969, and 0.893 (χ3 2=5.19, p>0.05). The data only became significantly different if analysed by first and second halves of the year, which showed observed versus expected ratios of 1.065 and 0.932 (χ2=4.24, p=0.039). This is demonstrated in table 4, with a relative risk of 1.14 (95% CI 1.01–1.30).
Observed (Obs) Crohn's disease (CD) births versus expected (Exp) by season
Crohn's disease (CD) births versus expected by year halves
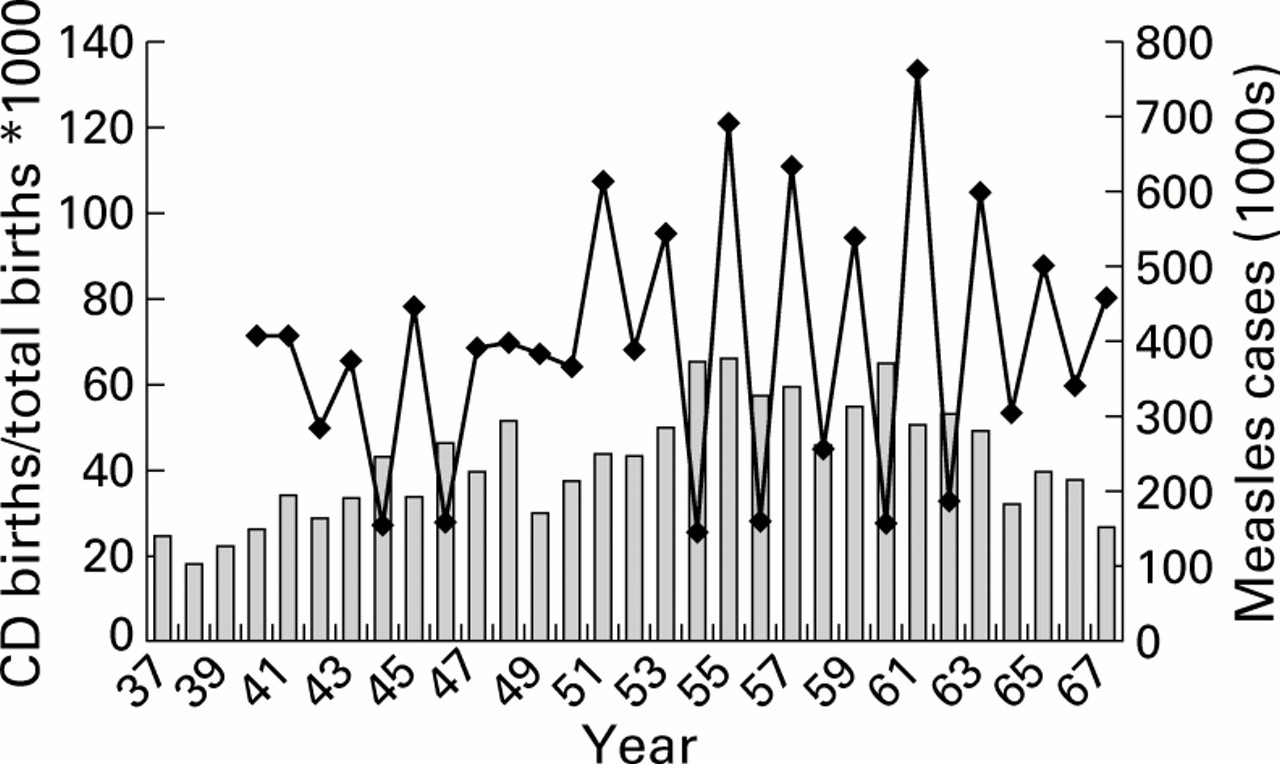
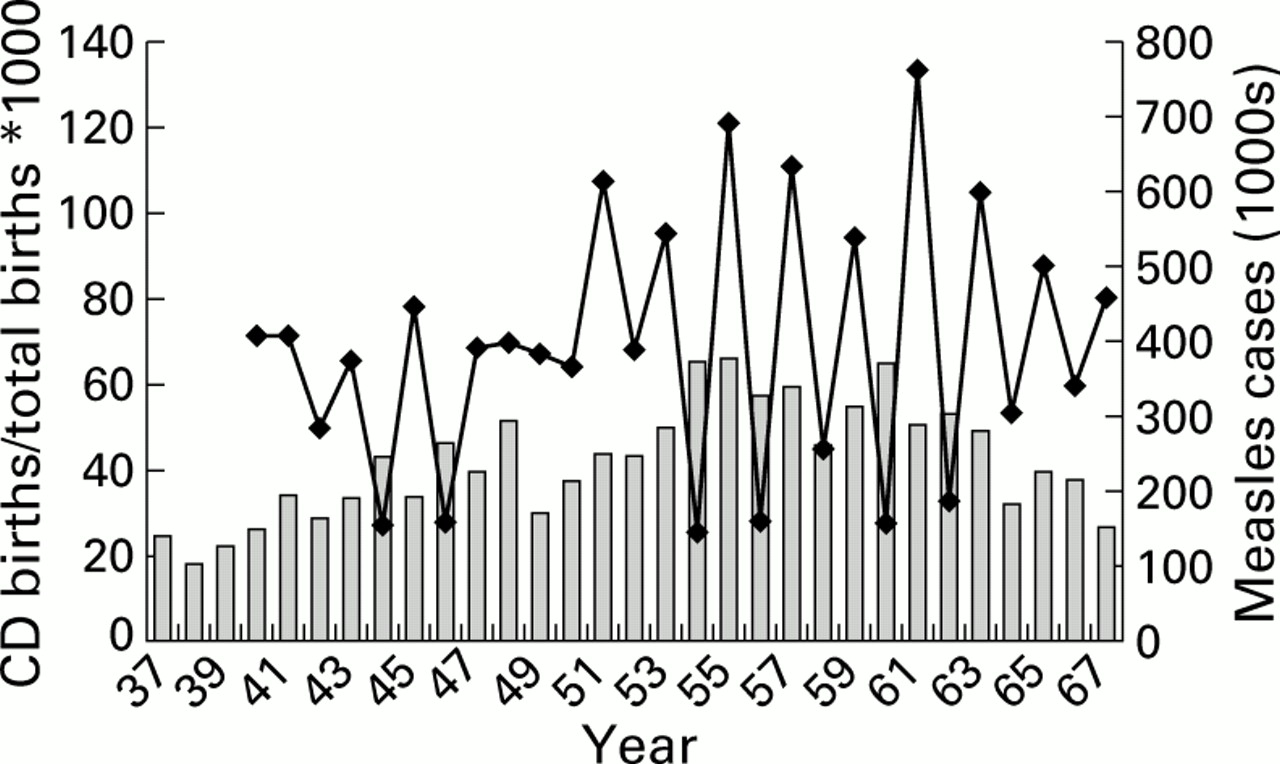
The number of measles notifications per year and CD cases born in those years are shown in table 5. CD cases are divided by total births in those years (multiplied by 1000) to produce an adjusted CD birth rate. The number of CD cases born in odd and even years during the period 1951–67 is shown in Figure 1. There was no significant difference in the proportion of CD cases between epidemic and non-epidemic years (χ1 2=0.17; p=0.68) (table 6). The estimated relative risk in a measles year was 0.98 (95% CI 0.84–1.14).
Total births, Crohn's disease (CD) births, adjusted CD birth rate, and measles notifications 1940–1967
{kind=link}
Measles notifications versus adjusted Crohn's disease (CD) birth rate by year.
Crohn's disease (CD) births in odd years versus even years for the years 1951–67
Discussion
Our results demonstrated no seasonal variation in the month of birth of patients who subsequently developed CD. Only when the data were analysed by year halves did a significant difference from expected arise and here the lower confidence limit for the relative risk (1.14) was only just greater than unity (1.01–1.30). With regard to measles, there was no evidence of any difference in incidence between epidemic and non-epidemic year births as would be expected whatever the hypothetical age of the patients subsequently.
We do not feel that the weak association we have demonstrated between births in year halves supports the hypothesis that early exposure to seasonal environmental factors may be of substantial aetiological importance. However, this seasonality has been reported previously. In a study of 1469 CD cases and 2509 ulcerative colitis (UC) cases diagnosed between 1945 and 1954, Ekbom and colleagues found that there was an increased risk of developing both CD and UC in those born in the first half of the year.17 The authors linked excess of births in the first half of the year in the Swedish study to influenza epidemics but a similar study in the UK18 found no association with measles epidemics and birth date and this is supported by the results of our data.
We believe our data suggest that in utero or perinatal exposure to seasonal environmental factors are unlikely potential aetiological agents in the later development of CD and that early exposure to measles is very unlikely to be implicated in the aetiology of CD.
Abbreviations used in this paper
- CD
- Crohn's disease
- IBD
- inflammatory bowel disease
- CI
- confidence intervals
- RR
- relative risk