Article Text

Abstract
Objectives: To investigate the relationship between smoke-free law coverage and secondhand smoke (SHS) exposure in the United States non-smoking adult population.
Design: We used data from the 1999–2002 National Health and Nutrition Examination Survey, a cross-sectional survey designed to monitor the health and nutritional status of the US population. Serum cotinine levels were available for 5866 non-smoking adults from 57 survey locations. Each location was categorised into one of three groups indicating extensive, limited, and no coverage by a smoke-free law.
Main outcome measures: The proportion of adults with SHS exposure, defined as having serum cotinine levels ⩾ 0.05 ng/ml.
Results: Among non-smoking adults living in counties with extensive smoke-free law coverage, 12.5% were exposed to SHS, compared with 35.1% with limited coverage, and 45.9% with no law. Adjusting for confounders, men and women residing in counties with extensive coverage had 0.10 (95% confidence interval (CI) 0.06 to 0.16) and 0.19 (95% CI 0.11 to 0.34) times the odds of SHS exposure compared to those residing in counties without a smoke-free law.
Conclusions: These results support the scientific evidence suggesting that smoke-free laws are an effective strategy for reducing SHS exposure.
- ANRF, American Nonsmoker’s Rights Foundation
- LOD, limit of detection
- MEC, mobile examination centre
- MVU, masked variance unit
- NCHS, National Center for Health Statistics
- NHANES, National Health and Nutrition Examination Survey
- SHS, secondhand smoke
- PSU, primary sampling unit
- secondhand smoke
- cotinine
- NHANES, National Health and Nutrition Examination Survey
Statistics from Altmetric.com
- ANRF, American Nonsmoker’s Rights Foundation
- LOD, limit of detection
- MEC, mobile examination centre
- MVU, masked variance unit
- NCHS, National Center for Health Statistics
- NHANES, National Health and Nutrition Examination Survey
- SHS, secondhand smoke
- PSU, primary sampling unit
Secondhand smoke (SHS), a preventable health hazard, causes lung cancer and coronary heart disease in non-smokers.1–3 The adverse health effects of SHS exposure in non-smokers have been documented since the early 1970s, yet the exposure still exists in many public places across the United States.4 Each year, there are 3000 lung cancer deaths and at least 35 000 coronary heart disease deaths in US non-smokers attributed to SHS exposure.5
Communities have been enacting laws to restrict smoking in public places for more than 30 years. The first tobacco control ordinance in the United States to limit smoking in restaurants was enacted in Berkeley, California in 1977. Ordinances limiting exposure to SHS in public spaces, restaurants, and worksites continued to be implemented throughout the 1980s.4 These early ordinances most often restricted rather than completely eliminated smoking in public areas.
Research now shows that worksites and restaurants with total smoking bans offer more protection from SHS exposure than worksites and restaurants with less restrictive smoking bans.1,6,7,8,9,10 Beginning in 1990, several cities in California passed 100% smoke-free laws, which completely prohibited smoking in certain types of locations and did not allow for variances.4 As more states and communities adopted restrictions, the evidence continued to show that they rapidly reduced SHS exposure and improved health.11–16 As of January 2006, there were 440 local laws and 15 state laws that require smoke-free air in at least one of three locations (workplaces, restaurants, and bars), covering 39% of the total US population.17
The National Health and Nutrition Examination Survey (NHANES) provides a unique opportunity to study the relationship between smoke-free indoor air regulations and SHS exposure. Since 1988, NHANES has used serum cotinine levels to estimate SHS exposure in the United States. Cotinine, the major metabolite of nicotine, has a half-life of about 16–20 hours.18,19 From 1988 to 2000 median cotinine levels declined by more than 70% in non-smokers, suggesting a dramatic reduction in SHS exposure of the US population.20,21 In this study, we examine the impact of smoke-free laws on SHS exposure utilising cotinine measures from NHANES.
METHODS
NHANES sample design
NHANES, conducted by the National Center for Health Statistics (NCHS), is designed to monitor the health and nutritional status of the civilian, non-institutionalised US population. In 1999 NHANES became a continuous survey and public use data files are released in two year cycles. This paper is based on the first four years of the continuous NHANES (1999–2002).
The NHANES sample is selected through a complex, multistage design, the details of which have been described previously.22 From 1999 through 2002, African-Americans, Mexican Americans, persons 12–19 years of age, and persons 60 years and older were over-sampled to improve estimates for these groups.
The survey consisted of a household interview and a standardised physical examination conducted in a specially-outfitted mobile examination centre (MEC). The interview included questions on sociodemographic characteristics, medical history, and health-related behaviours. During the physical examination, blood was obtained by venepuncture, and serum cotinine levels were measured for persons three years and older. Laboratory methods for serum cotinine have been described previously.20 The NHANES protocol was approved by the National Center for Health Statistics Research Ethics Review Board, Hyattsville, Maryland. Signed informed consent was obtained for all participants and remuneration was provided upon completion of the examination.
Of the 9471 adults aged 20 years and older who participated in the interview and physical examination, 8726 (92%) persons had cotinine measurements. We limited our sample to non-smokers, defined by both cotinine level and self-reported smoking status. A total of 6554 persons had cotinine levels ⩽ 10.0 ng/ml, a cut-off that has been used to define non-smokers.20,21 We further excluded 128 adults who reported they were current smokers, 12 adults with missing smoking histories, and 55 adults who reported tobacco or nicotine use in the five days before blood collection during the physical examination. We further excluded 428 adults who reported home SHS exposure and 65 persons with missing home exposure data to control for places of exposure potentially not regulated by public smoking laws, resulting in a final sample of 5866 persons, used for initial descriptive analyses.
Analytic variables
The outcome variable, exposure to SHS, was defined using cotinine levels ⩾ 0.05 ng/ml. This cut-off was based on the laboratory limit of detection (LOD) for NHANES survey years 1999–2000.
Respondents who had current jobs and indicated that they could smell smoke for one hour or more per day at work were classified as having work SHS exposure. To control for potential restaurant exposure to SHS we used the reported number of meals eaten at restaurants, dichotomised as either 0–3, or 4 or more meals per week.
Race/ethnicity was categorised as non-Hispanic white, non-Hispanic black, and Mexican American and other. Age, defined as age in years at the time of the household interview, was categorised as 20–39, 40–59, and 60+ years. Education was dichotomised as having a high school education or less, or more than a high school education.
Smoke-free laws: source and categorisation
Information on state and local smoke-free laws was obtained for all 57 NHANES locations from a database of local and state indoor air ordinances maintained by the American Nonsmoker’s Rights Foundation (ANRF).23 In order for a location to be classified as having a smoke-free law, state or local laws could not allow for separately ventilated smoking rooms, size exemptions, or allow smoking in bars attached to restaurants.23 For each NHANES study location, we only included laws enacted through the end of the calendar year preceding the year that the survey was administered.
The ANRF list indicated presence of smoke-free laws for workplaces, restaurants, and bars at the city, county, and state level. We categorised the survey locations (counties) into three smoke-free law coverage groups—extensive, limited, or no coverage—and classified survey participants accordingly based on their county of residence. Counties were categorised as having extensive coverage if at least one smoke-free law (workplace, restaurant, or bar) existed at the county or state level and covered the entire county population. Of the 12 counties that fell into this category, all had smoke-free restaurant laws and some had additional smoke-free workplace or bar laws. For these counties the laws covered both incorporated and unincorporated areas. A county was categorised as having limited coverage if there was not a state or county smoke-free law, but there was at least one municipality within the county with a smoke-free law (workplace, restaurant, or bar). Five counties fell into this category, and included a combination of restaurant, workplace, and bar smoke-free laws. Forty counties had no smoke-free law coverage at the state, county, or city level. For confidentiality and statistical disclosure reasons, the actual survey locations are not disclosed.
Data analysis and statistical methods
Data were analysed using the statistical programs SAS version 9.1 (SAS Institute Inc, Cary, NC) and SUDAAN version 9.0 (Research Triangle Institute, Research Triangle Park, NC). Examination sample weights were used to account for differential probabilities of selection and for non-response. Variance estimates were calculated using the Taylor linearisation with replacement method. T tests were calculated to test the null hypothesis of no difference in proportions using a significance level of p < 0.05. Estimates shown for counties with limited coverage by a smoke-free law had zero degrees of freedom, and therefore, standard errors in this category were estimated using the difference between the strata value and the overall mean for the population.24 Estimates for the extensive and limited coverage categories were compared to the no coverage group and these comparisons did not include an adjustment for multiple comparisons.
As described in the NHANES analytic guidelines, publicly released data files provide masked variance units (MVUs) to estimate sampling errors.25 MVUs were created to comply with disclosure avoidance principals that prohibit the public release of the primary sampling units (PSUs). Our main independent variable of interest, the smoke-free law coverage category, is based on the true PSUs and we used these strata variables, which are available through the NCHS Research Data Center (http://www.cdc.gov/nchs/r&d/rdc.htm), for calculating standard errors for all estimates.
Logistic regression analysis was conducted to examine the likelihood that non-smoking adults were exposed to SHS (cotinine levels ⩾ 0.05 ng/ml), controlling for potential confounding variables. We limited this analysis to non-Hispanic whites, non-Hispanic blacks and Mexican Americans, resulting in the exclusion of 484 persons of other race/ethnicity. Logistic regression modelling was performed to evaluate all covariates and first order interaction terms. The only significant interaction was between gender and law coverage; gender-specific models were employed to account for this interaction. No additional interaction terms were significant in the gender-stratified models.
RESULTS
Approximately 16.8% (95% confidence interval (CI) 10.3% to 26.1%) of non-smoking adults resided in counties with extensive coverage by a smoke-free law, 9.4% (95% CI 3.5% to 22.8%) lived in counties with limited coverage, and 73.9% (95% CI 61.6% to 83.3%) in counties with no coverage. Demographic characteristics of the survey participants varied across smoke-free law coverage categories (table 1). In the extensive coverage category, there was a larger proportion of Mexican Americans and a smaller proportion of non-Hispanic blacks compared with the no coverage category. Gender, education, and workplace SHS exposure differed between the limited and no coverage categories; however, this should be interpreted with caution because of the small number (5) of PSUs in the limited coverage category.
Selected characteristics of non-smoking adults by smoke-free law coverage category
Selected centiles of cotinine concentrations by smoke-free law coverage category are shown in table 2. The median cotinine level was below the limit of detection for all three groups. Adults with extensive coverage showed no detection of cotinine up through the 75th centile. The 90th and 95th centile values in the extensive coverage group were 80% lower than for the no coverage group.
Selected centiles of cotinine concentrations (ng/ml) for non-smoking adults by smoke-free law coverage category
An estimated 39.1% of all non-smoking adults had measured SHS exposure (table 3). Among adults in counties with extensive coverage, 12.5% were exposed to SHS, compared with 35.1% in counties with limited coverage, and 45.9% in counties with no coverage. The prevalence of SHS exposure among non-Hispanic blacks (63.8%) was significantly higher than the prevalence among non-Hispanic whites (35.4%) and Mexican Americans (37.5%). Other demographic groups with comparatively higher SHS exposures were men, persons with a high school education or less, and younger adults. Those with workplace exposure and those who reported four or more restaurant meals per week also had higher SHS exposure.
Prevalence of secondhand smoke (SHS) exposure (cotinine levels ⩾0.05 ng/ml) among non-smoking adults by selected characteristics
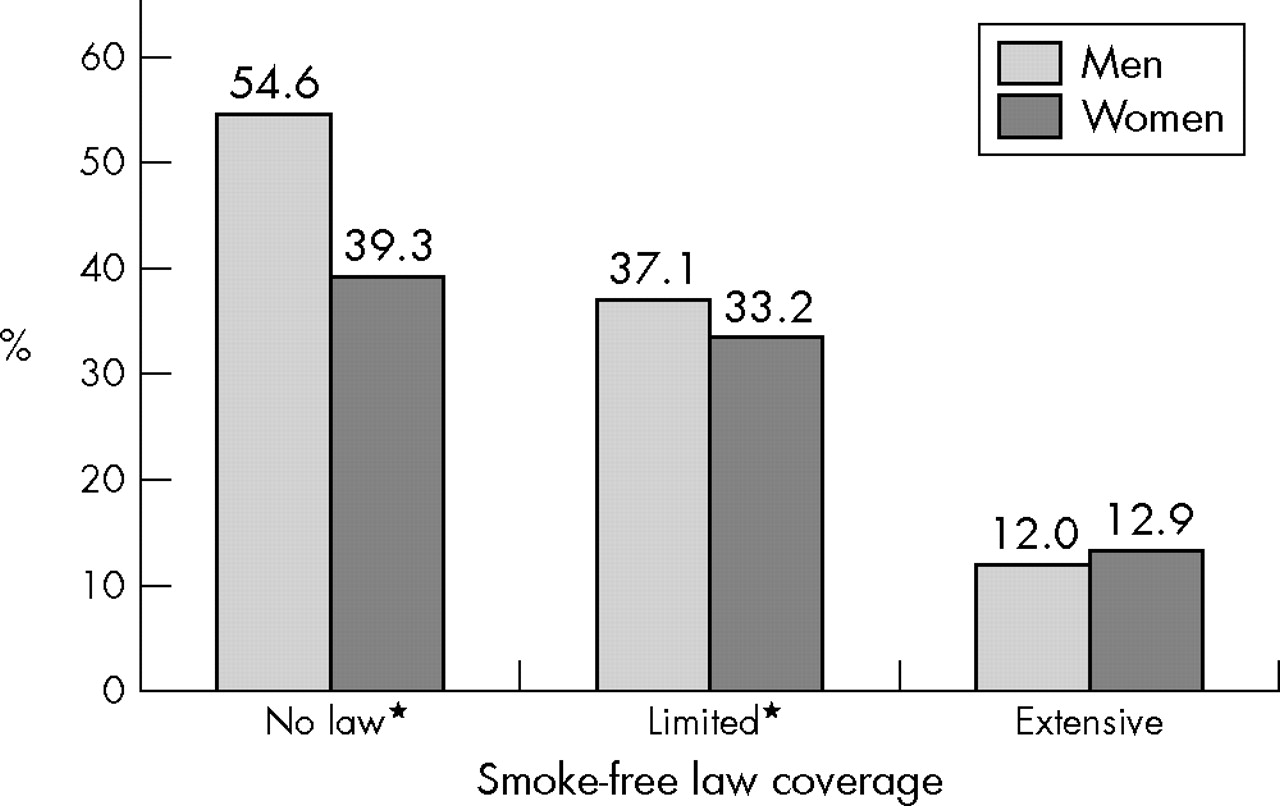
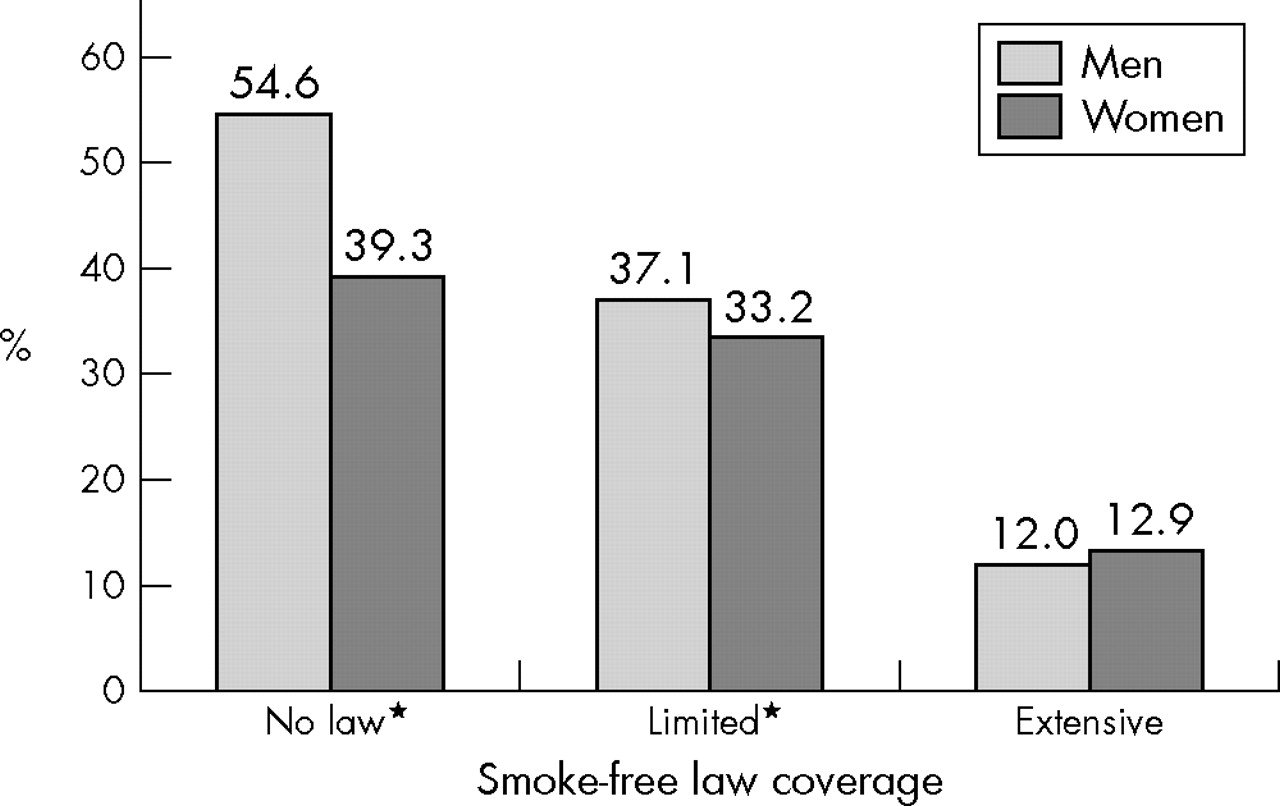
Gender and SHS exposure varied by smoke-free law coverage (fig 1). In counties with limited or no smoke-free law coverage, men had a higher prevalence of SHS exposure than did women. There was no difference between men and women in counties with extensive coverage. Due to this interaction effect between gender and the degree of coverage we used gender-specific logistic regression models.
{kind=link}
Prevalence of secondhand smoke exposure among non-smoking adults by gender and smoke-free law coverage category. *p < 0.05.
Table 4 shows the adjusted odds ratios among non-smoking adults from gender stratified logistic regression models, excluding those classified as “other race/ethnicity”. Both men and women in counties with extensive coverage had decreased odds of SHS exposure after adjusting for race/ethnicity, age, education, and number of restaurant meals. Among men, those residing in counties with extensive coverage had 0.10 (95% CI 0.06 to 0.16) times the odds of SHS exposure, and among women, those in counties with extensive coverage had 0.19 (95% CI 0.11 to 0.34) times the odds of SHS exposure compared to those without smoke-free law coverage. Men residing in counties with limited coverage had 0.57 (95% CI 0.38 to 0.89) times the odds of SHS exposure compared with men residing where there was no smoke-free law. There was no significant difference in exposure for women comparing counties with limited coverage to those with no coverage. For both sexes, younger age groups relative to older age groups, non-Hispanic blacks relative to whites, those with less than or equal to a high school education, and those who ate at restaurants four or more times a week, had an increased odds of SHS exposure, controlling for level of law coverage.
Adjusted odds ratios (95% CI) for SHS exposure, stratified by men and women*
DISCUSSION
This is the first study to examine the relationship between coverage by state and local smoke-free laws and an objective measure of SHS exposure in a national survey. Our findings indicate that there was a significant association between the level of coverage and SHS exposure. Tobacco-free adults without home SHS exposure living in areas with county-wide coverage by at least one smoke-free workplace, restaurant, or bar law consistently had a lower prevalence of SHS exposure than adults residing in counties without a smoke-free law. Our results showed that there was up to a 90% reduction in the odds of SHS exposure for adults residing in counties with extensive coverage compared to those without smoke-free policies. Specifically, men in counties covered by at least one smoke-free law had one tenth the odds and women had one fifth the odds of being exposed to SHS, compared with men and women residing in areas not governed by a smoke-free law. The strength of the associations in both men and women provides evidence of the beneficial effects of smoke-free laws in the US population.
We used gender-stratified logistic regression models because of the interaction effect between gender and smoke-free law coverage categories. The prevalence of SHS exposure among men and women was similar living in areas with extensive coverage, suggesting that smoking restrictions may protect both men and women equally. However, men had higher SHS exposure than women in the limited and non-coverage areas. A possible reason for this difference is that men may work in or frequent establishments that allow smoking more often than women. We do not have additional exposure information in NHANES to explore this issue further.
For all non-smoking adults, education (less than or equal to a high school education) and age (20–39 years) were associated with an increased likelihood of SHS exposure. This is consistent with patterns of cigarette smoking among adults. Adults with less than a high school diploma typically are more likely to be employed in blue collar or service worker jobs, and less likely to be protected by a smoke-free policy than white collar workers.26,27 Non-smoking adults in our study may be exposed to SHS through demographically similar peer groups.
In our multivariate analysis, non-Hispanic blacks were up to three times more likely to be exposed to SHS than non-Hispanic whites. Previous studies have shown that non-Hispanic blacks have higher cotinine levels than non-Hispanic whites in non-smokers20,28 as well as smokers.29–31 The studies of smokers have suggested that differences may be due to nicotine metabolism or clearance, type of cigarette smoked (mentholated or non-filter) and patterns of smoking behaviour.29,30,32 Although there was a smaller proportion of non-Hispanic blacks in counties with extensive coverage compared to the other coverage groups, this was controlled for in the multivariate analyses.
Limitations of our study should be noted. Because the smoke-free law classification scheme is not part of the sample design of NHANES, the primary sampling units (counties) selected during the four years of the survey may not be statistically efficient with respect to representation of all US counties within each coverage category. Estimates for smoke-free law coverage groups may have differed if the counties were selected to be specifically representative of these categories.
Another limitation is that individual risk of exposure to SHS may not be captured by the three smoke-free law coverage categories in our analysis. Individual workplaces and restaurants may have more restrictive voluntary policies than their respective local or state laws. For example, participants classified as residing in a county with no coverage may have potentially worked in a 100% smoke-free building, and this may explain the low proportions of adults who reported work SHS exposure (9.3%) in counties with no smoke-free laws. Likewise, counties with extensive smoke-free law coverage were not uniform with respect to the type of location covered. Specifically, all of the counties had a smoke-free restaurant law, but not all counties had bar or workplace laws. Also, we did not take into account adults who worked or spent time outside their county or state of residence and may have been subjected to a different set of tobacco control laws. Lastly, we focused on smoke-free laws and did not consider less restrictive ordinances,33 which, nevertheless, provide some protection from SHS exposure in public places and worksites.
In our survey we found that the prevalence of current smoking among all adults varied by level of law coverage. In counties with extensive, limited and no smoke-free law coverage, the prevalence of smoking was 17.2% (95% CI 13.6% to 21.6%), 16.7% (95% CI 12.4% to 22.1%), and 26.6% (95% CI 24.7% to 28.5%), respectively. Research suggests that strong smoke-free laws may contribute to reductions in smoking prevalence.1,8,34–36 Due to the cross-sectional design of the survey, we could not determine whether smoke-free laws help reduce smoking prevalence or whether smoke-free laws were more likely to be implemented in areas with lower smoking rates. We also cannot rule out the possibility that less second hand smoke exposure occurs in places with extensive coverage because there are fewer smokers in these areas.
Despite these limitations, our results are consistent with previous studies comparing SHS levels in localities before and after the implementation of smoke-free laws. In California, self-reported SHS exposure among bartenders showed a reduction of about 93% in the median hours of exposure.11 New York and Delaware both saw reductions in respirable suspended particles in hospitality venues of 84% and 90%, respectively, after state laws required all indoor workplaces and public places to be smoke-free.13,14 In the Republic of Ireland, after legislation of smoke-free workplaces and bars was enacted, salivary cotinine levels declined by 80% among bar staff.37
Other studies show that not only do smoke-free laws reduce SHS exposure, but that they improve the respiratory and cardiovascular health of populations as well. Eisner et al found that after smoking was banned in bars and taverns in California in 1998, there was a rapid improvement in respiratory health among bartenders.11 During a six month period that a smoke-free workplace law was in effect in Helena, Montana, hospital admissions for acute myocardial infarction decreased by 40% and returned to previous levels after the ordinance was suspended.12 Farrelly and colleagues showed a decline in salivary cotinine, as well as in sensory symptoms among hospitality workers one year after the implementation of New York’s smoke-free laws.15 Declines in respiratory symptoms were also reported among bar staff in the Republic of Ireland and in Norway after the implementation of smoke-free laws.37–39
Smoking bans and restrictions as a means to reduce exposure to SHS and prevent significant morbidity and mortality are based on strong scientific evidence.1,40 Our results enhance earlier findings that smoke-free laws are an effective strategy for reducing SHS exposure. Over the past 10 years, we have seen a marked increase in smoke-free laws at the state and local levels in the United States, as well as in other countries.17,33,41 When cotinine levels were first measured in NHANES (1988–91) 90% of non-smokers had detectable levels of cotinine,20 and less than 1% of the US population was covered by a smoke-free worksite, restaurant, or bar law.42 By 2002, approximately 15% of the population was covered by a smoke-free law (L Williams, ANRF, personal communication), and according to the 1999-2002 NHANES, only 43.4% had detectable cotinine levels. It is encouraging to note that by 2006, 39% of Americans are protected by a state or local smoke-free law.17
What this paper adds
Several studies have shown reduced levels of secondhand smoke (SHS) in public places after implementation of a smoke-free law. These studies have focused on policies specific to state, city, or workplace laws, and have most often measured SHS exposure using self-reported or environmentally monitored data.
This is the first study to look at the relationship between smoke-free laws and SHS exposure in a national population using a direct measure of SHS exposure, serum cotinine. We found a strong inverse association between smoke-free law coverage and SHS exposure. This study adds a new perspective to the body of evidence showing that persons who live in areas with smoke-free laws have lower SHS exposure than persons not protected by these regulations.
REFERENCES
Supplementary materials
An error has occured in the exclusions to obtain the final analytic sample for the research paper titled "Smoke-free laws and secondhand smoke exposure in US nonsmoking adults, 1999-2002" which was published in the August 2006 issue of Tobacco Control. The authors inadvertently did not excude 51 persons who indicated that they had used tobacco products in the past 5 days from the 2001-2002 NHANES survey because of a slight modification in the variable name from the 1999-2000 survey. If the exclusion had been applied correctly the final analytic sample would have consisted of 5815 persons rather the 5856, a difference of less than 1 percent. The authors have not yet rerun their analyses with the correct exclusion, but do not expect any substantial differences in their results or conclusions because the difference in the sample size is so small.
Footnotes
-
↵* At the time that this research was conducted, Ms Pickett was an Association of Teachers for Preventive Medicine Fellow at the National Center for Health Statistics, Centers for Disease Control and Prevention
-
Funding: The NHANES is supported by direct appropriations from the US Congress. Ms Pickett was supported under a cooperative agreement from the Centers for Disease Control and Prevention through the Association of Teachers of Preventive Medicine
-
Declaration of competing interests: The authors of this manuscript have no competing interests to declare
-
Ethics approval: The NHANES protocol was approved by the National Center for Health Statistics Research Ethics Review Board, Hyattsville, Maryland
-
The findings and conclusions in this report are those of the author(s) and do not necessarily represent the views of the Centers for Disease Control and Prevention.