Article Text

Abstract
This study aimed to assess whether previously established risk factors for sudden infant death syndrome (SIDS) are still valid now that the incidence in the Netherlands has dropped to 0.26 per 1000 liveborn infants. A distinction was made between immutable and mutable risk factors. This case-control study (part of the European Concerted Action on SIDS) comprised 73 SIDS cases and 146 controls and lasted from March 1995 to September 1996. Adjustments were made for sleeping position and bedding factors by treating them as covariables. Apart from these factors, well known risk factors that remain of importance in the Netherlands are: male sex, young maternal age, twins, and low socioeconomic status. These factors are largely immutable. Other well known risk factors which might reflect attitudes to child care and could possibly be mutable are: smoking, alcohol consumption by the mother, bottle feeding, and change of babycare routine. Intervention strategies should focus on early signalling, thereby assisting parents in changing these unfavourable parenting attitudes. Information on optimal child care and extra support by public health nurses specifically aimed at families at risk could help to decrease further the incidence of SIDS in the Netherlands.
- sudden infant death syndrome
- risk factors
Statistics from Altmetric.com
Since 1969, when the term “sudden infant death syndrome” (SIDS) was introduced, many factors associated with this syndrome have been elucidated.1 These include immutable risk factors, such as male sex, low birth weight, short gestation, twins, young motherhood and multiparity, age at death of the infant (2–3 months), and death during the winter season. Risk factors which are difficult to change but possibly mutable are smoking, bottle feeding, psychological factors such as postpartum depression of the mother, child abuse, poor socioeconomic status, parental drug use, change of routine, and colds. Risk factors for SIDS that seem to be mutable, and thus amenable to prevention, are prone sleeping position, hyperthermia, use of sedatives, and bed sharing.2-19Protective factors that have been described recently are room sharing,20 use of dummies (pacifiers),21 and use of a sleeping sack (a simple cotton bag with armholes, no sleeves, with a zip in the front).18
In this study we examined whether the risk factors for SIDS described in 19691 remain valid in light of the 1995 rate of only 0.26 per 1000 livebirths (fig 1). The present population of SIDS infants could well have different characteristics from previous populations. Treating the newly identified risk and protective factors18 as confounders, the present study aimed to identify remaining risk factors amenable to prevention. A ranking was made from “immutable”, to “difficult to change”, to “mutable” in order to improve and target preventive strategies more effectively.

Sudden infant death syndrome (SIDS), sudden unexpected death (SUD) incidence, and post-perinatal death per 1000 livebirths in the Netherlands (Dutch Central Bureau of Statistics 1996 (Overledenen naar doodsoorzaak, leeftijd en geslacht. Serie A1. Voorburg: CBS, 1997) and the percentage of infants placed prone to sleep. SIDS defined as: 1969–1978 International Classification of Diseases, Injuries and Causes of Death (ICD) eighth revision, number 795.0 (sudden death, cause unknown and other ill defined and unknown causes of morbidity and mortality); 1979–1994 ICD ninth revision, number 798.0 (SIDS/cot death/sudden death of non-specific cause in infancy); 1995–1996 ICD 10th revision number R95 (SIDS/cot death). SUD defined as: 1969–1978 ICD eighth revision numbers 795.0 (sudden death, cause unknown), 796.0, 796.2, 796.3, 796.9 (other ill defined conditions), E913.0, E913.9 (accidental mechanical suffocation); 1979–1994 ICD ninth revision numbers 798.0, 798.2, 798.9 (cot death, sudden death of non-specific cause in infancy), 799.0, 799.1, 799.8, 799.9 (respiratory failure and other ill defined conditions or specific causes), E913.0, E913.1, E913.2, E913.3, E913.8, E913.9 (accidental mechanical suffocation and other unspecified means); 1996 ICD 10th revision numbers R95.0, R96.1, R98.0 and R09.0, R09.2, R99.0, and W75, W76, W81, W83, W84.
Methods
The methods in this study have been described in detail previously.18 The Dutch European Concerted Action on SIDS (ECAS) cot death study was carried out nationwide from 1 March 1995 to September 1996. The population of the Netherlands is 15 million, with 190 000 livebirths, and currently about 50 SIDS cases a year. We intended to include all sudden and unexpected deaths. A case-control design was chosen, with two controls for every SIDS case, matched for date of birth. Controls were born within one week of the case. Owing to strict privacy rules, researchers do not have access to municipal records. Names and addresses of two control families were selected and they were asked to participate by the municipal authority in whose district the death had occurred. Two other controls were recruited from the list of births in the nearest largest urban area. When there were more than two replies, two were randomly selected.
Initially we included all infants who died suddenly and unexpectedly and whose death was unexplained when first found. After postmortem examinations were completed, three pathologists, not primarily involved in the case, independently reviewed the cases. By consensus cases were excluded when major pathological abnormalities were found.
The ECAS questionnaire consisted of 228 questions and included demographic, maternal, infant, and family factors. Several questions, of particular relevance to the Dutch situation, were added to the ECAS protocol. All questionnaires were completed by an interviewer during a home visit. The interviewers were two of the researchers and four medical students who had been given repeated special training.
Protocol for a full postmortem examination comprised a short initial history, external clinical examination, death scene investigation, and necropsy. Deaths between 7 days of age and 730 days were included. Excluded were deaths of premature babies who had never left hospital, and babies specifically taken home to die. Reference sleep was defined for SIDS cases as the sleeping period when the baby died, and for controls as the sleeping period on the day before interview corresponding to the time of day when the index baby died. For cases and controls, “usual” related to the usual routine for the time of day of reference sleep. Socioeconomic status was defined by several markers concerning housing and education. An average socioeconomic status was marked zero, above average given a positive value and below average a negative value. A change in routine was defined very broadly as all changes in babycare, such as unusual sleeping period, change in feeding, absence of the usual caretaker, and a sleeping place other than usual.
National demographic data were obtained from the Dutch Central Bureau of Statistics and from the Royal Dutch Meteorologic Institute.
STATISTICS
Data were entered by EPI info and analysed with the Statistical Package for Social Sciences. χ2 tests, correlations, andt tests were used to compare cases and controls; p values are two tailed, unless stated otherwise. Odds ratios (OR) are given, with a 95% confidence interval (CI). In all analyses, adjustments were made for the following confounders: age, sleeping position, bedding, found with head and body covered, and dummy (pacifier) use. These are the risk and protective factors found in the previous logistic regression analysis of the same dataset.18 We chose to use age as a linear term, because using a logarithm or quadratic term did not make a significant difference.
MATCHING
We were able to match all controls for date of birth of the case within two weeks. The median time from death to the home interview was 34 days for SIDS cases and 77 days for controls, owing to delay of ascertainment via municipalities. Therefore, we adjusted for the age of the child over the analyses. Adjustment for age did not have a major impact on the age independent risk factors, so no new confounding was introduced by this correction. By comparing unconditional (no matching) and conditional logistic regression analyses (matched) we found no differences in the standard error. We decided to use an unconditional logistic regression analysis, due to the complexity of the statistical analyses.
Results
RESPONSE CASES AND CONTROLS
Of 105 sudden unexpected deaths notified to the research centre, six were excluded according to the criteria and 11 families refused to participate. Of these 11 cases the age distribution was similar to the response group; there were eight boys and one girl (sex in two cases was unknown), three belonged to an ethnic minority group and two had a strict religious background. In the other 88 cases a home visit was made and the questionnaire completed. Fourteen cases were excluded as non-SIDS with major pathological abnormalities. Of the remaining 74 cases, a complete postmortem examination was carried out on 49 and no postmortem examination was conducted on 25 cases. Of the 81 SIDS cases that were booked at the Dutch Central Bureau of Statistics in the 798.0 and 798.1/798.2 (more than 1 year, less than 2 years) categories of the International Classification of Diseases, Injuries and Causes of Death (ICD) ninth revision (ICD-9), and R95 and R96 categories of the ICD-10 revision during the research period, 74 cases participated in our study. There were always at least two controls per case. Because of a matching error at a municipality, two control questionnaires had to be excluded. Finally, 73 SIDS cases and 146 controls were included in the multivariate analyses.
ANALYSES
Boys were overrepresented in our study, compared to the national distribution of male liveborn infants. The mean (SD) age at death in children under 1 year was 5 (3.07) months. The infants who died within the first year of life were classified according to their age at death (0–11 months, fig 2). A statistical test of the null hypothesis of a uniform frequency distribution over the 12 months was significant (χ2 = 19.85, df = 11, p = 0.04). The same null hypothesis was used separately for boys and girls and these tests were not significant (Fisher exact test, boys p = 0.49, girls p = 0.10).
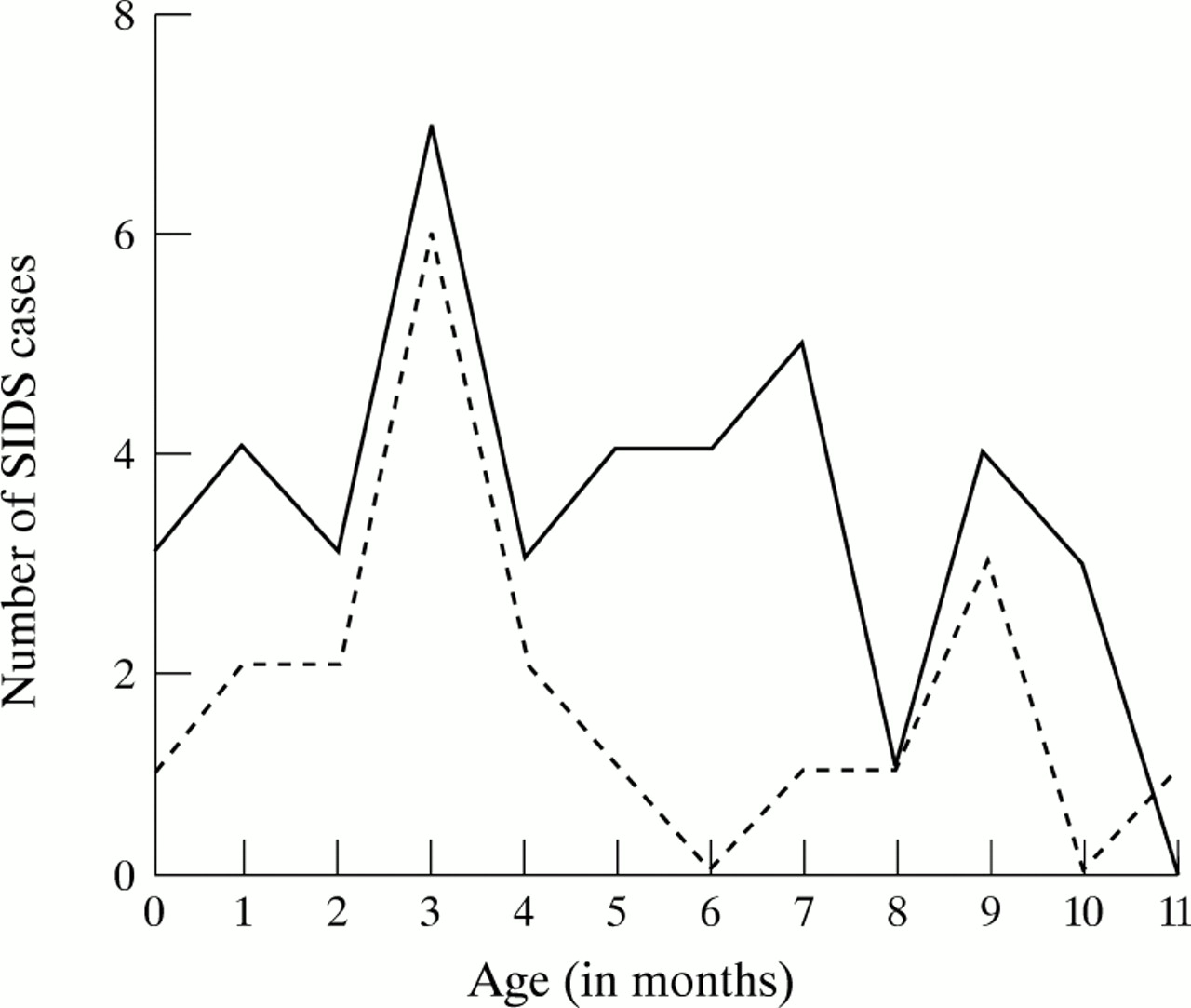
Age at death in months of SIDS cases. Solid line, boys; broken line, girls.
Deaths were classified according to season into two periods—six lowest temperature months (October to March, n = 19) v six highest temperature months (April to September, n = 27)—from March 1995 to March 1996. The null hypothesis of a uniform distribution over the two periods was tested using the χ2 test. The result of the test was not significant (χ2 = 1.72, df = 1, p = 0.24). From March 1996 to September 1996 the number of SIDS cases was 27.
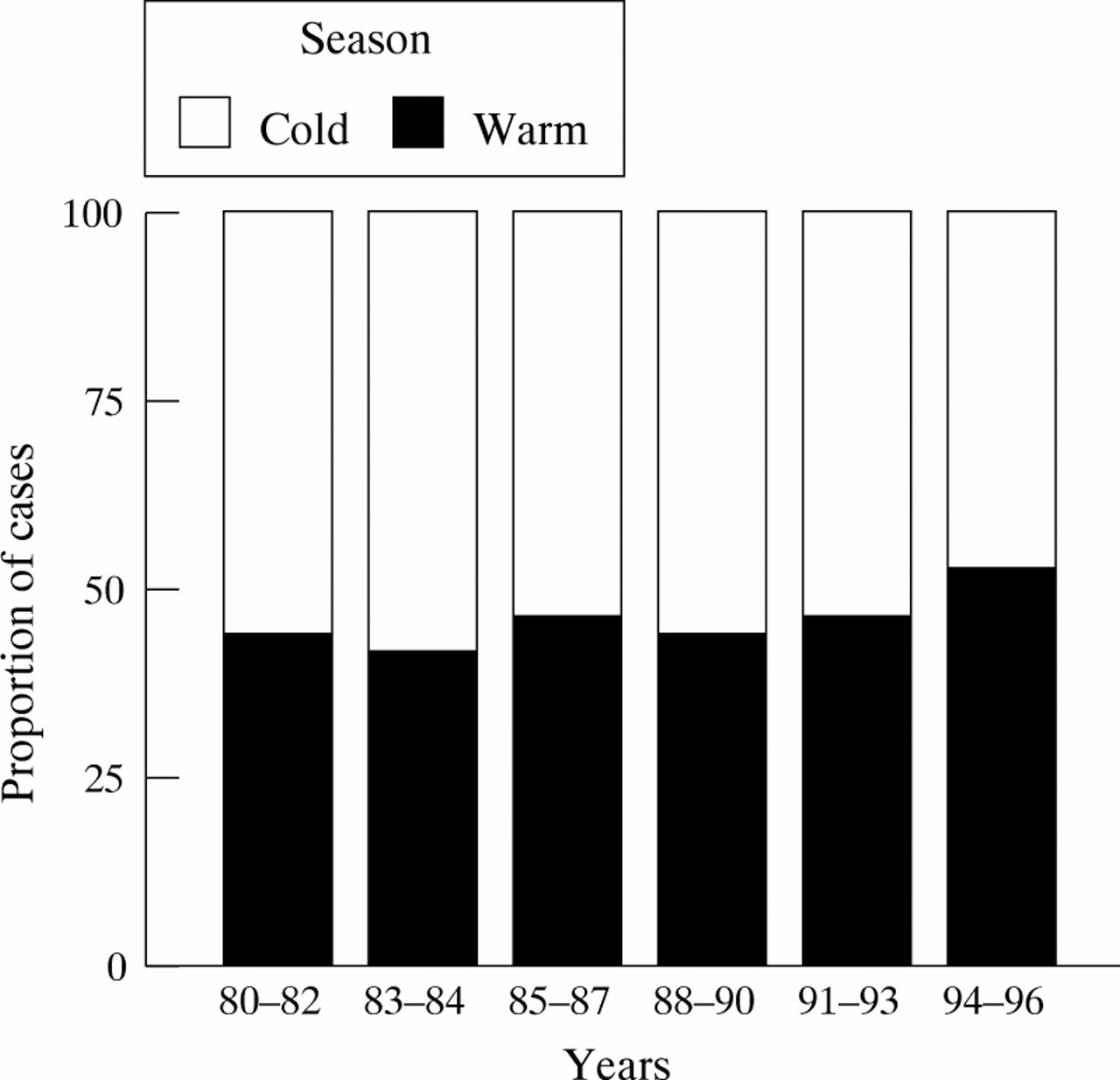
Figures 3 and 4, showing national data, demonstrate that the rate of SIDS is still higher in boys than girls, the age peak has flattened, and differences in distribution of SIDS cases over the cold and warm months decreased from 1980 to 1996.
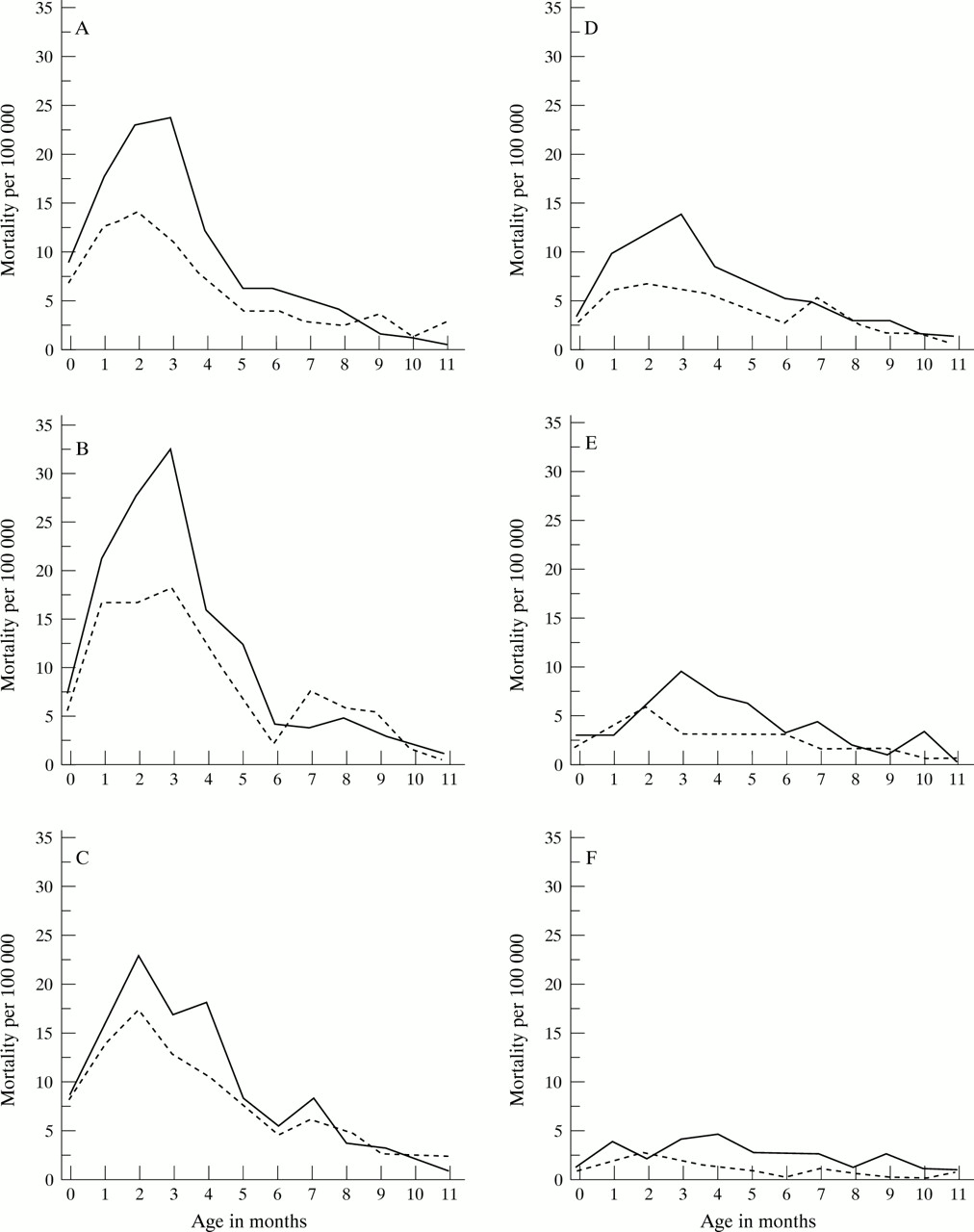
SIDS mortality per 100 000 liveborn infants aged 0–11 months during six periods: (a) 1980–82, (b) 1983–84, (c) 1985–87, (d) 1988–90, (e) 1991–93, (f) 1994–96 extended after publication of de Jonge and Hoogenboezem (1994).2 (Dutch Central Bureau of Statistics, 1996). Solid line, boys; broken line, girls.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Proportion of SIDS cases occurring during warm (April to September) and cold (October to March) seasons from 1980 to 1996 (Dutch Central Bureau of Statistics, Royal Dutch Meteorologic Institute, 1996).
Table 1 shows the confounders: infant’s age, placed to sleep in side or prone position, secondary prone sleeping, dummy (pacifier) use, use of a sleeping sack, duvet use, head and body totally covered, and a combination of the last two. The sleeping sack and the duvet were not significant. However, before we incorporated the combination of having used a duvet and ending up head and body covered, the sleeping sack had an OR of 0.27 (0.08–0.96) and the duvet an OR of 3.46 (1.01–11.90). The interaction of a duvet and head and body totally covered demonstrated that ending up under a duvet is associated with an increased risk. The analysis of these confounders has been described extensively elsewhere.18
Confounders for the determination of the well known risk factors for SIDS
Based on a literature review and earlier Dutch data4 5 25 27 well known risk factors were selected. These were explored by performing univariate analyses, after which we decided to include them in the multivariate models. Table 2 provides a description of these factors. We found a correlation between maternal psychological problems and smoking before and during pregnancy, and after birth (0.34, 0.34, 0.30, respectively p < 0.01).
Description of well known risk factors for SIDS
Table 3 shows three models: “immutable”, “mutable”, and a combination of the two. In the “immutable” model, we included stepwise factors that cannot be changed, but are of concern for general health care. Factors significant at the 5% level were included. In subsequent steps, a factor was excluded when p ⩾ 0.10 (table 3). The included factors were maternal age, twins, birth weight, and socioeconomic status. Gestation was not incorporated because it strongly correlated with birth weight. Twins remained a significant risk factor, even after correcting for gestational age and birth weight. Twelve of the cases were born at a gestational age below 37 weeks and 15 had a birth weight lower than 2500 g. Four of these cases were born with a very low birth weight (less than 1500 g) and before 32 weeks’ gestation.
Risk and preventive factors for SIDS in an “immutable”, a “mutable”, and a “combined” model, including the odds ratios (with 95% CI) adjusted for the confounders2-150
In the “mutable” model the immutable factors were left out of the analysis and possibly mutable factors were incorporated: passive smoking (a combined effect of parental smoking), breast feeding, alcohol use, and change of routine (table 3). Alcohol consumption the evening before reference sleep by the mother, not by the father, proved significant.
Finally, a “combined” model was made in which all factors were included (table 3). Young maternal age, twins, low socioeconomic status, alcohol use by the mother in the 24 hours before death, and bottle feeding remained significant risk factors. Low birth weight and change of routine tended to be risk factors and postnatal passive smoking no longer reached significance. Table 3 gives the increasing percentages of correctly predicted classifications for each model. For the model with only the confounders the percentage of correctly predicted classification is 88.1%. This percentage is increased by 5.26% after incorporating the well known risk factors.
Discussion
Our aim was to assess whether previously established risk factors, divided into immutable and mutable, retained their validity in the face of the reduced incidence of SIDS. Campaigns against prone sleeping were started in 1987 and, since 1994, duvets and cot buffers have been discouraged. In the Netherlands the “reduce the risks” recommendations are followed widely. Despite this, bedding factors and prone sleeping are still of major importance in the occurrence of SIDS.18
A SIDS group of 73 is small but sufficient to yield moderate effects with a power of 0.75–0.80 for general tests.22 Strict privacy laws in the Netherlands, with a necessarily circuitous route via municipal authorities to approach control families, resulted in considerable delay in interview time for controls. We therefore adjusted for age at reference sleep in the analyses. A time interval between the interview of cases and controls is not unusual, and comparable to the other 11 participating centres of the ECAS study.23
In the Netherlands, necropsy is not mandatory; about 60% to 70% of infants who die have a full postmortem examination. In this study, major pathological abnormalities acceptable as a cause of death were found at postmortem examination in 14 cases. These were excluded. The inclusion of 25 cases without necropsy does not invalidate the study.24
The higher incidence of boys with SIDS has been partly explained by the prevalence of parents to place boys in the prone position, as well as to boys turning to the prone position more than girls.18 25 Also, a sex specific sensitivity to smoking might play a role.26
In the Netherlands a change in age distribution of SIDS had already been noticed2 and the national data confirm this. One explanation could be that not placing infants in the prone position to sleep specifically prevents early SIDS. In the present study the previous peak incidence of SIDS at 2–3 months remains manifest.
We did not find a higher SIDS incidence in winter, nor did we find any association between colds and SIDS, although it is very difficult in a small case-control study to demonstrate any effect of colds on the risk of SIDS. An earlier study of SIDS registration at the Dutch Central Bureau of Statistics from 1969–72 showed no clear seasonal distribution, except for a preponderance of accidental mechanical suffocation in the summer.27 From 1980–93 a winter peak was found,2 but in the national data of 1994–96 there were more SIDS cases during the summer months (fig 4). With such a low incidence, chance variation becomes more likely so that further monitoring is necessary. Advice about room temperature, ventilation, and appropriate bedding might be responsible for the present absence of a winter peak. Before a definitive answer can be given on the role of the seasons, an extensive analysis should be performed on national data, taking into account the seasonality of births and age effects.
Young age of the mother at first birth remained a risk factor for SIDS, as in almost all previous epidemiological studies.28 Very young mothers might care differently for their babies than older mothers, and they may possibly have many worries, other than those about their child. Multiparity was no longer a significant risk factor, after adjusting for sleeping position. Mothers who still placed their infant prone had a higher parity than mothers who did not, which may provide an explanation.
Low socioeconomic status combines many risk factors. In the control group it correlated significantly (p < 0.05) with young maternal age, tog values during reference sleep, duvet use, and smoking.
It is known that infants born with a low birth weight, a short gestation, or both have an increased risk for SIDS as well as a generally increased death rate, such that the lower the birth weight, the higher the risk.3 4 Damage suffered in the prenatal and perinatal period, hypoxia,4 lung dysfunction, and brain stem dysfunction have been described as possible explanatory mechanisms that might impair ventilatory, circulatory, and arousal responsiveness.29 In the Netherlands, Wierenga and colleagues30 estimated that the incidence of SIDS in very low birthweight infants (less than 1500 g), and/or who had a very short gestation (less than 32 weeks), decreased from about 1 per 100 in 1983 to 1 per 1000 in 1995–96. The incidence of SIDS in all infants less than 2500 g, and/or with a gestation less than 37 weeks, remained unchanged compared to earlier studies— between 15% and 20% of the total births.
In the “combined” model low birth weight had an estimated odds ratio of 2.13 per 500 g less, but significance was not reached. However, an increased risk of SIDS among low birthweight infants is shown in virtually all studies. External factors might play a larger role than previously supposed in infants with a low birthweight and/or gestation less than 37 weeks, which together encompass 7% of all Dutch births.31 Firstly, the prevalence of prone sleeping position among low birthweight infants after discharge from hospital is higher compared to other infants.32 The new approach in the Netherlands is to get low birthweight infants and those with a gestation less than 37 weeks used to the supine position before leaving hospital but this may not always happen in practice. Secondly, we demonstrated that low birthweight infants sleep less frequently (13%) in the protective traditional cotton Dutch sleeping sack than do mature children (75%).18 Thirdly, low birth weight is partly a marker for socioeconomic status.33 Fourthly, an additional factor is that an infant with a low birth weight induces stress and fatigue in the family. Conditions may not have been optimal in some of these families and insufficient bonding between parents and child might have played a role.34 All the above factors, more often in combination than singly, probably play a role in the death of infants with a low birth weight, a short gestation, or both.
Twins are at increased risk for SIDS, even after adjustment for birth weight and gestational age.3 This could be spurious, because of the small numbers of the groups (six cases and two control twins), but is in accordance with previous studies. Vulnerability of twins could play a role,35 as could the extra stress on parents and their coping ability.
In the “mutable model”, parental postnatal passive smoking yielded a significant result (table 3). Like others, we found a dose-response effect with smoking.9 10 36 A relation between maternal smoking and fetal growth has been established, while the association between smoking and preterm birth is less certain.37 The positive correlation between maternal psychological problems and excessive smoking may be a reflection of stress or a sign of addiction.33 Smoking habits might reflect a health attitude, related to socioeconomic status. We demonstrated that before pregnancy, mothers of SIDS babies and control mothers differed little in respect to smoking habits. However, more control mothers than mothers of SIDS babies gave up smoking or reduced their smoking after conception.
When parental alcohol consumption the evening before the death was added to the logistic regression model, only alcohol use by the mother was significant. Probably in most families it is the mother who wakes up to feed the infant, even when formula fed. Fatigue combined with alcohol could play a role to the extent that the mother does not hear her child.
We demonstrated, as have others, an independent adverse effect of formula feeding after controlling for age, sleeping position, bedding, head covered, and dummy (pacifier) use.11 12 A protective effect of breast feeding has not been found universally, but this depends on which confounders are adjusted for.12 17Social and cultural factors are related to breast feeding.11 Adjustment for these factors may reveal the real effects of formula feeding. There are three possible explanations why breast feeding could be protective against SIDS. Firstly, breast milk itself is protective, perhaps by preventing or modifying infection. Secondly, the way infants suck may be of importance. The muscles of the mouth and lower jaw are under greater strain when breast feeding than when drinking from a bottle. The diameter of the pharynx depends on the tone of these muscles.38 Furthermore, a baby who is breast fed turns his or her neck seeking the breast thus training the neck muscles. This might influence the capability of head turning, when lying prone. Thirdly, psychosocial factors could be of importance. Eriksen39 demonstrated a strong association between maternal smoking and the frequency of starting supplemental feeding and stopping breast feeding. He found that the association was independent of demographic characteristics and that there was a dose response effect of smoking. As smoking is strongly associated with formula feeding the same psychological factors which interfere with starting breast feeding may play a role in continuing to breast feed.
Established risk factors and their associations have been previously described in terms of stress.33 40 41 The immutable risk factors could be interpreted cautiously as “stress increasing conditions” and the mutable as “parental reactions in the face of stress”. Conditions that may increase parental stress may include intrauterine growth retardation, giving birth to an infant with a low birth weight and/or short gestation, having twins, an emotionally unstable state and, to a certain extent, the socioeconomic situation. Stress alleviating reactions—independent of whether these are effective in the long run—may include sleeping together in one bed (either suppressing parental loneliness or because of fatigue), change of routine, alcohol use, smoking, and formula feeding, the latter two being strongly related.36
Stressed parents need help, but may not seek or accept help. Furthermore, advice about sleeping position and bedding may not reach parents under stress or may not be heeded by them. This means that postnatal care of young mothers, parents of prematurely and dysmaturely born infants and of twins, and families under stressful conditions should receive special attention. Intervention strategies should focus on early detection of these unfavourable conditions. Parents need to be informed specifically about preventive measures concerning SIDS and offered help and extra guidance on how to care for their child—for example, by public health nurses. These parents are easily identified by the combination of excessive smoking, alcohol consumption, and formula feeding. Removal of the psychological “benefit” of the stimulants is unlikely to occur by itself. We believe educational programmes are needed, including home based motivational counselling, to discourage smoking during pregnancy and postnatal passive smoking. Early identification should enable us to provide extra attention to these parents and help them to avoid pursuing unfavourable habits to combat stress. This might further decrease the incidence of SIDS.
Acknowledgments
We are indebted to all the parents who participated in this study, and to Dr O Huber-Bruning and S McClelland. We acknowledge the National Working Group Cot Death, GA de Jonge, and J Hoogenboezem (Dutch Central Bureau of Statistics). We also would like to thank the Royal Dutch Meteorologic Institute in De Bilt. This study was supported by the Praeventie Fonds, ‘s-Gravenhage, the Netherlands.
References
Linked Articles
- Rapid responses