Primary care management of postoperative shoulder, hip, and knee arthroplasty
BMJ 2017; 359 doi: https://doi.org/10.1136/bmj.j4431 (Published 18 October 2017) Cite this as: BMJ 2017;359:j4431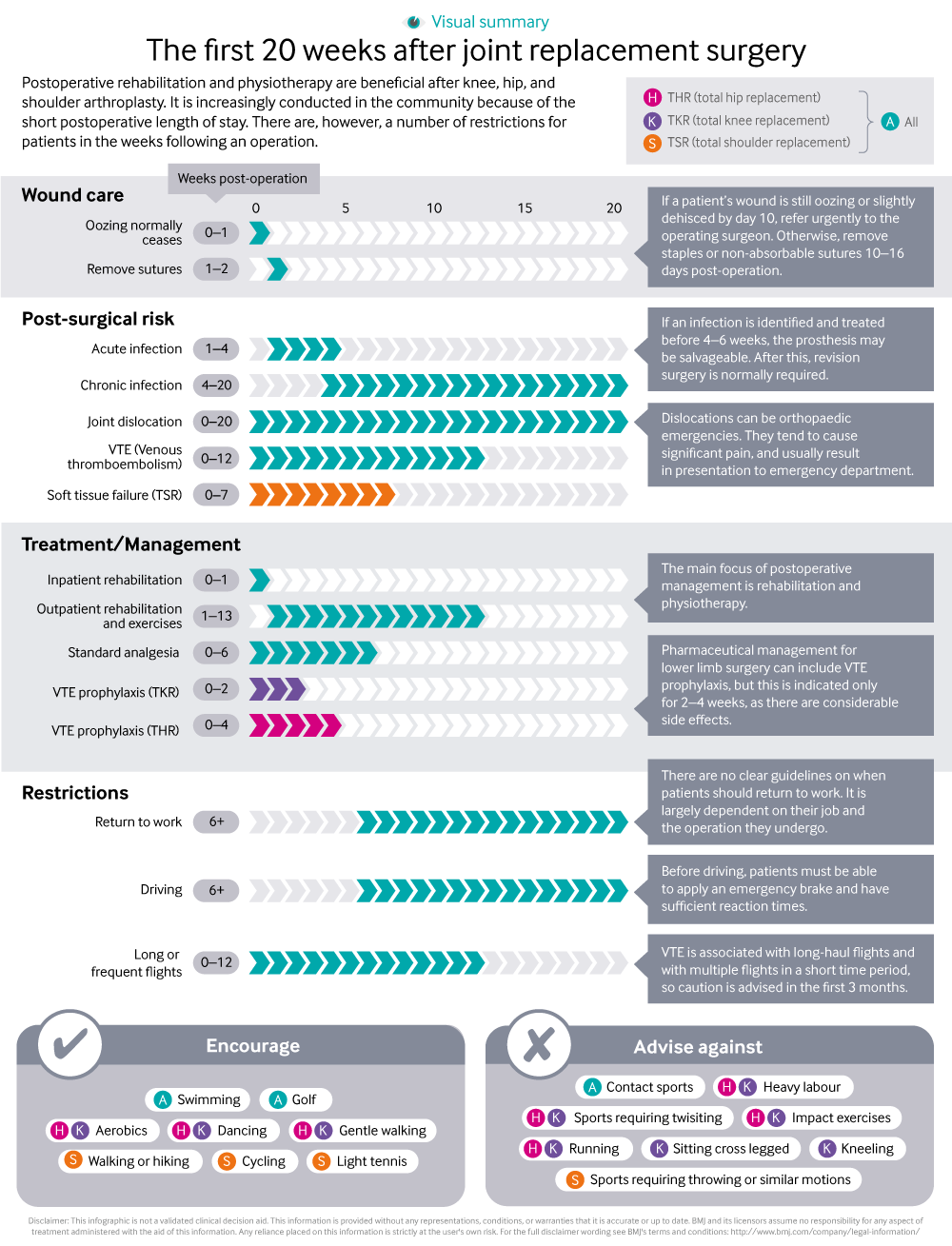
Infographic available
A visual summary of management and restrictions for people following joint replacement surgery.

All rapid responses
Rapid responses are electronic comments to the editor. They enable our users to debate issues raised in articles published on bmj.com. A rapid response is first posted online. If you need the URL (web address) of an individual response, simply click on the response headline and copy the URL from the browser window. A proportion of responses will, after editing, be published online and in the print journal as letters, which are indexed in PubMed. Rapid responses are not indexed in PubMed and they are not journal articles. The BMJ reserves the right to remove responses which are being wilfully misrepresented as published articles or when it is brought to our attention that a response spreads misinformation.
From March 2022, the word limit for rapid responses will be 600 words not including references and author details. We will no longer post responses that exceed this limit.
The word limit for letters selected from posted responses remains 300 words.
Thank you for the very helpful list of activities to be encouraged/avoided after this surgery
However, many patients will also be anxious to know when they can resume sexual intercourse, and what positions they should avoid and for how long.
Can you help?
Competing interests: No competing interests
We applaud the Practice Pointer from Aresti et al, as arthroplasty management has advanced significantly and data from effective research collaboration in Orthopaedics and the National Joint Registry is driving improvements in quality of care. However, their article does not necessarily fairly represent where the new evidence for enhanced recovery has originated; and may not go far enough in recommending ‘that restrictions (after hip replacement) are by default adhered to unless the surgeon instructs to the contrary.’
Much as we appreciate the citation of our own publication (1) for the beneficial outcomes of enhanced recovery , credit should really be given in large part to the fast-track approach pioneered in Copenhagen by Husted (2) and Kehlet (3). Mobilising the same day & aiming for discharge within 48 hours is primarily directed at improving outcomes and reducing complications (4) , but also reduces costs. There is increasing evidence this strategy is successful for all three (5 6) .
As well as the systematic review (7) and physiotherapy viewpoint (8) cited there is other data supporting abandoning universal precautions after hip replacement. This includes a Cochrane systematic review on post-hip replacement on assistive devices, hip precautions, environmental modifications and training to prevent dislocation and improve function after hip arthroplasty (9), which included only 3 RCTs. While this concluded more high quality data is needed, the data reviewed included one small trial where hip precautions were abandoned (10) , which didn’t increase dislocation but was powered to show significantly improved function & recovery time (despite n=81) and one trial of 265 patients (303 hips) where randomisation to using equipment or not showed only one dislocation- related to an abduction pillow in the aids group (11). Peak estimated the costs of aids at $655 per patient (about £500 at current exchange rates). However, compelling evidence we can and should safely change practice comes from Henrik Husted, whose unit abandoned hip precautions and use of equipment like raised toilet seats in 2010 and recently published observational data from four years before and after the switch (12) . This large representative study can be interpreted with the caveats relevant to any observational study. After 1st August 2010 ‘They were specifically told that no restrictions applied for them, which was reinforced in writing.’ Dislocation rates were equivalent before and after the change with a non-significant trend to fewer dislocations (2.8% vs 3.4% at 90 days) and significant reduction in revision for dislocation (0.6% vs 1.7%; p<0.02). Even avoidable dislocation was comparable (6/1329 0.5% vs 4/946 0.4%).
Not every clinical question needs a randomized controlled trial to answer it and not every orthopaedic surgeon has the desire or the time to review the evidence for themselves. Ververeli et al has shown improved function when precautions are removed in a randomised trial (10) and robust observational data has already shown that the major potential risk is not increased by abandoning hip precautions. The van der Weegan systematic review cited by Aresti et al is very clear ‘A more liberal lifestyle restrictions and precautions protocol will not lead to worse dislocation rates after total hip arthroplasty, but will lead to earlier and better resumption of activities and higher patient satisfaction. These results appear to hold up for various surgical approaches’ (7). So is it time for the NHS to abandon routine hip precautions & aids, rather than leaving this to each surgeon? This could save up to £40million per annum (assuming a lower cost than USA of £400 per patient for aids and 101,651 hip replacements cited in the the 14th National Joint Registry Annual Report; 13 ) and improve outcomes.
References
1 Malviya A, Martin K, Harper I, et al. Enhanced recovery program for hip and knee replacement reduces death rate. Acta Orthop2011;359:577-81
2 Husted H, Hansen HC, Holm G, Bach-Dal C, Rud K, Andersen KL, Kehlet H. Length of stay in total hip and knee arthroplasty in Denmark I: volume, morbidity, mortality and resource utilization. A national survey in orthopaedic departments in Denmark.[Article in Danish] Ugeskr Laeger. 2006 May 29;168(22):2139-43.
3 Kehlet H, Wilmore DW. Multimodal strategies to improve surgical outcome. Am J Surg 2002; 183 (6): 630-41.
4 Husted H. Fast-track hip and knee arthroplasty: clinical and organizational aspects. Acta Orthop Suppl. 2012 Oct;83(346):1-39. doi: 10.3109/17453674.2012.700593. Review.
5 Husted H, Otte KS, Kristensen BB, Ørsnes T, Wong C, Kehlet H. Low risk of thromboembolic complications after fast-track hip and knee arthroplasty. Acta Orthop. 2010 Oct;81(5):599-605. doi: 10.3109/17453674.2010.525196.
6 Sutton JC 3rd, Antoniou J, Epure LM, Huk OL, Zukor DJ, Bergeron SG.Hospital Discharge within 2 Days Following Total Hip or Knee Arthroplasty Does Not Increase Major-Complication and Readmission Rates. J Bone Joint Surg Am. 2016 Sep 7;98(17):1419-28. doi: 10.2106/JBJS.15.01109.
7 van der Weegen W, Kornuijt A, Das D. Do lifestyle restrictions and precautions prevent dislocation after total hip arthroplasty? A systematic review and meta-analysis of the literature. Clin Rehabil2016;359:329-39.
8 Chartered Society of Physiotherapy. ATOCP conference: Trauma and orthopaedic physios vote for the abolishment of hip precautions after surgery. 2016. www.csp.org.uk/news/2016/11/29/atocp-conference-trauma-orthopaedic-physios-vote-abolishment-hip-precautions-after-s.
9 Smith TO, Jepson P, Beswick A, Sands G, Drummond A, Davis ET, Sackley CM. Assistive devices, hip precautions, environmental modifications and training to prevent dislocation and improve function after hip arthroplasty. Cochrane Database of Systematic Reviews 2016, Issue 7. Art. No.: CD010815. DOI: 10.1002/14651858.CD010815.pub2
10 Ververeli PA, Lebby EB, Tyler C, Fouad C. Evaluation of reducing postoperative hip precautions in total hip replacement: a randomized prospective study. Orthopedics 2009;32(12):889.
11 Peak EL, Parvizi J, Ciminiello M, Purtill JJ, Sharkey PF, Hozack WJ, et al. The role of patient restrictions in reducing the prevalence of early dislocation following total hip arthroplasty: a randomized, prospective study. Journal of Bone and Joint Surgery 2005;87(2):247–53.
12 Gromov K, Troelsen A, Otte KS, Ørsnes T, Ladelund S, Husted H. Removal of restrictions following primary THA with posterolateral approach does not increase the risk of early dislocation. Acta Orthopaedica 2015;86(4):463–8.
13 National Joint Registry 14th Annual Report. http://www.njrreports.org.uk/Portals/0/PDFdownloads/NJR%2014th%20Annual%... accessed 8th November 2017
Competing interests: No competing interests
A few points
1. Do the authors ensure that (unexpected events apart) the SAME physiotherapist carries out preop assessment and education of the patient AND post-op care?
It seems self-evident that this is far better than different physios preop and postop.
2. Can the authors give data for wound dehiscence - a) after sutures, b) after clips?
Where dehiscence did occur, was it because of poor nutritional state
OR
Poor technique? (inadvertent inversion of wound edges)
3. Here I ask Mr Alam and colleagues -
Why should a clean ORTHOPAEDIC wound require preop antibiotics?
If the fear is that circulating bacteria in the blood might decide to find a “nest” in the raw bones or indeed in the surgically damaged tissues (a perfectly reasonable scenario) then it seems reasonable to continue the antibiotic for 48 hours post-op.
4. I ask the authors and Mr Alam and his colleagues -
Surely the GP (educated in the UK, or in a reputable medical school abroad, or having spent six months working in orthopaedics or in general surgery) should be considered capable of FIRST taking a swab ftom the oozing site, SECOND, starting antibiotics IF he/she condiders necessary and then, THIRD, referring the patient straightaway to the Team which operated upon him/her.
I would appreciate replies on the points raised.
Competing interests: No competing interests
Dear Sir
We found the ‘Practice Pointer’ by Aresti et al on Postoperative management of shoulder, hip or knee arthroplasty very useful in explaining what to expect in the first 20 weeks after joint replacement, especially the infographic. 1
For the past three years, we have been running a multidisciplinary team meeting (MDT) to review and advise on the management of bone and joint infections including those following joint replacement surgery. As the patients are discharged very soon after surgery (< 5 days) many of the infections become apparent in the community. These patients are seen by GPs or community nurses. In our experience, some of the GPs and nurses have made an incorrect diagnosis of infection in the immediate postoperative period based on presence of redness and oozing of serosanguinous fluid from the wound. Invariably these patients are commenced on antibiotics, often without taking wound swabs.
In England, all NHS hospitals performing joint replacement surgery are mandated to report surgical site infections (SSI) occurring within a month of the surgery. As a result of infection being identified in self-completion post-discharge surveillance questionnaires, we recently reviewed three patients who were diagnosed and treated for superficial SSI of knee arthroplasty in the community. On review, two of the patients did not have any evidence of infection at the time of diagnosis and one had prolonged oozing, without other signs of infection. All three had fully healed wounds one month after surgery. Incorrect diagnosis of postoperative infection has implications for the patient (anxiety and unnecessary antibiotic treatment) and the organisation (misleading infection rates).
We have recently developed a care pathway where GPs and community nurses are advised not to treat cases of suspected postoperative infection of arthroplasty but to urgently refer to a nurse in the orthopaedic department. The nurse assesses the patient and refers to an orthopaedic surgeon if she suspects an infection.
Competing interests: No competing interests
I am disappointed that the authors of this Practice Pointer did not even mention Unicompartmental Knee replacement (UKR) . Up to 50% of knees requiring arthroplasty are suitable for a UKR. (Willis-Owen et al. UKA in the UK NHS. Knee 2009)
UKR patients have a shorter length of stay, and a lower complication, readmission and mortality rate. (Lidddle et al. Adverse outcomes after TKR + UKR in 101,330 matched pts. Lancet 2014) GPs can improve the postoperative experience for their patients with arthritic knees by referring them to a surgeon who does a significant number of UKRs. Unfortunately we are few and far between.
Competing interests: No competing interests
I was amazed to read that enhanced recovery programmes after hip arthroplasty are now “fully implemented” in the NHS (1).
This was certainly not my experience when I had a displaced neck of femur fracture eleven months ago. I saw from my ‘neighbours’ in the ward that my problems were not a personal one-off.
I don’t think, either, that the problems I saw are restricted to the central London hospital I was treated in. Perry et al reviewed data from the UK’s National Hip Fracture Database in 2016. They found that only 32% of adults with a displaced intracapsular fracture of the femoral neck who were eligible under NICE criteria had a total hip replacement (THA). Of those who underwent THA, 42% did not meet the NICE eligibility criteria.(2) As the accompanying editorial commented, “the degree of non-adherence to [the] guidance was remarkable.” (3)
White, writing less than two months before my operation, reported that, even in trials, “current models of service delivery for hip fractures are unlikely to be able to provide timely total hip arthroplasty for suitable patients.”(4)
Even if the surgery can be got right, this ‘practice pointer’ was aimed at primary care, but did not mention osteoporosis - I had to insist on a DEXA scan for myself before I could get the appropriate medication - or other co-morbidities, when these are surely likely to affect, and be affected by, the short and long-term outcomes of major surgery. I felt there was an especial difficulty with, and for, the large number of patients with some degree of dementia. Their distress was evident when they cried out through most nights, increasing exhaustion and so deconditioning for all of the inpatients.
And it’s really important to get hip fractures right. Just the hospital costs have been estimated at £1131 million a year in the UK. Incidence is expected to rise by 32 % in 2025: with hospital costs expected to increase to £1493 million.(5)
1. Aresti N, Kassam J and Kutty S. Primary care management of postoperative shoulder, hip, and knee arthroplasty. BMJ 2017;359:j4431
2. Perry DC. Inequalities in use of total hip arthroplasty for hip fracture: population based study BMJ 2016;353:i2021
3. Chaudhry H. Total hip arthroplasty after hip fracture BMJ 2016;353:i2217
4. Huxley C. A process evaluation of the WHiTE Two trial comparing total hip arthroplasty with and without dual mobility component in the treatment of displaced intracapsular fractures of the proximal femur. Bone Joint Res. 2016 Oct; 5(10): 444–452.
5. Leal J et al. Impact of hip fracture on hospital care costs: a population-based study
Osteoporos Int. 2016; 27: 549–558.
Competing interests: For my THA, I begged to be given a spinal anaesthetic. After it was made clear to me that this was unusual, the anaesthetist failed to achieve a spinal block, so I had to have a GA. 10 hours with only water in ‘recovery’ because of bed shortages did not help my post op nutrition. Catheterisation was routine and, after the catheter bag was placed above my bladder, I had bypass incontinence and a UTI. The severe shooting pains through the nights for several months after I was discharged, made the exhaustion and inevitable deconditioning worse. I had to wait a month before an OT gave me any advice about washing at home other than telling me not to get in a bath or shower, and not to sit on the stool they had given me. The article doesn’t mention the constipation with opioid analgesia - this can only be ignored by someone who has not suffered from it. I was told that senna would 'soften' my stools, but was not surprised when this did not happen. I was also not surprised that the ward staff had ‘lost’ the iPad for patient feedback on my discharge: I told one of the night nurses when she gave me someone else’s medication, and it didnt go down well at all. Especially when she couldnt find some of my medication, and I presumed she’d given that to another patient. She had clearly thought more deeply when she came back at, I think it was 2 or 3 am, to insist on shaking my hand and telling me that we were ‘friends after all’. I’m still not as fit as I was before my fracture.
I was surprised to read that swimming was recommended as an activity for patients who have had shoulder replacement, although activities such as tennis were not. Most swimming strokes - certainly front crawl, butterfly and backstroke - require a significant range of movement from the shoulder. Even breaststroke requires more movement than one would usually make with the shoulder day to day.
I wonder what stroke the authors were thinking with? I can't say I would be comfortable with recommending that someone with a shoulder replacement go swimming.
Competing interests: No competing interests
Re: Primary care management of postoperative shoulder, hip, and knee arthroplasty. The authors remain silent while tgere are SEVEN responses
Dear Authors
Seven of us (readers) raised some points.
Could you not spare a few minutes to respond to us? After all, the BMJ is a vehicle for enlightenment .
Thank you
JK Anand
Competing interests: No competing interests