
- Kate Jolly, senior lecturer in public health and epidemiology1,
- Lucy Ingram, research midwife1,
- Khalid S Khan, professor of women’s health and clinical epidemiology2,
- Jonathan J Deeks, professor of biostatistics1,
- Nick Freemantle, professor of clinical epidemiology and biostatistics3,
- Christine MacArthur, professor of maternal and child epidemiology1
- 1Department of Public Health, Epidemiology and Biostatistics, University of Birmingham, Birmingham B15 2TT, UK
- 2Barts and the London School of Medicine, London, UK
- 3Department of Primary Care and Population Health, University College London, London, UK
- Correspondence to: K Jolly C.B.Jolly{at}bham.ac.uk
- Accepted 31 October 2011
Abstract
Objective To examine the effect of setting, intensity, and timing of peer support on breast feeding.
Design Systematic review and metaregression analysis of randomised controlled trials.
Data sources Cochrane Library, Medline, CINAHL, the National Research Register, and British Nursing Index were searched from inception or from 1980 to 2011.
Review methods Study selection, data abstraction, and quality assessment were carried out independently and in duplicate. Risk ratios and 95% confidence intervals were calculated for individual studies and pooled. Effects were estimated for studies grouped according to setting (high income countries, low or middle income countries, and the United Kingdom), intensity (<5 and ≥5 planned contacts), and timing of peer support (postnatal period with or without antenatal care), and analysed using metaregression for any and exclusive breast feeding at last study follow-up.
Results Peer support interventions had a significantly greater effect on any breast feeding in low or middle income countries (P<0.001), reducing the risk of not breast feeding at all by 30% (relative risk 0.70, 95% confidence interval 0.60 to 0.82) compared with a reduction of 7% (0.93, 0.87 to 1.00) in high income countries. Similarly, the risk of non-exclusive breast feeding decreased significantly more in low or middle income countries than in high income countries: 37% (0.63, 0.52 to 0.78) compared with 10% (0.90, 0.85 to 0.97); P=0.01. No significant effect on breast feeding was observed in UK based studies. Peer support had a greater effect on any breastfeeding rates when given at higher intensity (P=0.02) and only delivered in the postnatal period (P<0.001), although no differences were observed of its effect on exclusive breastfeeding rates by intensity or timing.
Conclusion Although peer support interventions increase breastfeeding continuation in low or middle income countries, especially exclusive breast feeding, this does not seem to apply in high income countries, particularly the United Kingdom, where breastfeeding support is part of routine postnatal healthcare. Peer support of low intensity does not seem to be effective. Policy relating to provision of peer support should be based on more specific evidence on setting and any new peer services in high income countries need to undergo concurrent evaluation.
Introduction
Breast feeding, both exclusively and partially, confers health benefits to infants and mothers. This led to the World Health Organization’s recommendation that all babies should be exclusively breast fed for the first six months after birth.1 Breastfeeding rates are, however, suboptimal in many countries.2 Overall, 76% of women in the United Kingdom and 74% in the United States reported initiation of breast feeding, but rates are considerably lower in some regions within countries. Although many low and middle income countries3 have high rates of some degree of breast feeding, exclusive breast feeding even up to four months is often low (50% in Bangladesh and 29% in Pakistan).2
A Cochrane systematic review4 of trials up to 2005 reported that lay support significantly reduced the risk of not breast feeding: not breast feeding at all (at end of studies) by 14% (95% confidence interval 2% to 24%) and not exclusively breast feeding by 28% (10% to 43%). The results of the studies for both analyses showed substantially statistically significant heterogeneity, with I2 values (a measure of the percentage of total variance across studies attributable to the heterogeneity rather than to chance) of 76% and 97%, respectively. In this situation, explanations for the observed differences in effects should be explored as these can provide useful information for generating guidance.
The UK National Institute for Health and Clinical Excellence issued guidance that peer support programmes should be used to increase breast feeding, especially among women with low incomes.5 However, none of the four UK based randomised controlled trials and the one quasi-randomised trial were able to show significant improvements in any or exclusive breastfeeding rates.6 7 8 9 10 We hypothesised that differences in effects between studies may result from different levels of routine support for breast feeding in different settings or the intensity or timing of the delivery of the peer support intervention. It is probable that in settings where the routine level of support for breastfeeding mothers is high, more intensive interventions would be required to achieve an effect.
We carried out a systematic review and meta-analyses of the effectiveness of peer support on breast feeding, investigating the effect of setting, intensity, and timing of the intervention on continuation of any and of exclusive breast feeding.
Methods
Peer support was defined as support offered by women who have received appropriate training and either have themselves breast fed or have the same socioeconomic background, ethnicity, or locality as the women they are supporting. Peer supporters may be voluntary or receive basic remuneration or expenses.
We looked at two outcomes: any breast feeding at the end of the study follow-up and exclusive breast feeding at the end of the study follow-up. We used each paper’s definition of exclusive breast feeding, which in most was the definition used by WHO.1
Literature search
We identified potentially relevant citations through a comprehensive electronic search of the following bibliographic databases and resources: British Nursing Index (1994-June 2011), CINAHL (1967-2011), the Cochrane Library, Embase (1974-June 2011), Medline (1948-June 2011), and controlled trials website (see web extra on bmj.com for search terms). We manually searched the reference lists of retrieved articles.
A form containing inclusion and exclusion criteria was used to select citations and papers. To be included the trials needed to have recruited pregnant or postpartum women, provided the peer support intervention in the antenatal and postnatal period or postnatal period only, had usual care as the comparator, reported any or exclusive breast feeding at least four weeks postpartum, and used randomisation to create the study groups.
No language restrictions were applied. Two reviewers (LI and KJ) obtained and assessed all citations and hard copies of potentially eligible papers for relevance. Uncertainties were resolved in consultation with other reviewers (CM and KSK).
Data extraction and risk of bias assessment
Two reviewers (LI and KJ) independently extracted data on participants, intervention (including setting, intensity, and timing of peer support) and comparator arms, study design, methods, and results. Where participants were missing from follow-up we assumed that they had stopped breast feeding, as is standard practice in meta-analyses in this specialty.4 11 The same two reviewers independently assessed the risk of bias according to the methods in the Cochrane handbook,12 documenting the quality of random sequence generation and allocation concealment, description of dropouts and withdrawals, blinded outcome assessment, and selective outcome reporting.
Data synthesis
Where available we used risk ratios, with 95% confidence intervals, or we calculated these from other reported data. Although trials typically discuss the relative proportions of women still breast feeding, we meta-analysed the relative risk of not breast feeding, as it is more likely to be constant across settings where initiation rates vary. Using the relative risk of not breast feeding predicts effective interventions to make a greater absolute impact in settings where more women fail to continue breast feeding than in settings where continued breast feeding is already common, whereas meta-analysis of the relative risk of still breast feeding would predict the opposite pattern, which is less tenable.13 We avoided odds ratios as they risk being misinterpreted when event rates are high, as with “any” breast feeding in low or middle income countries.14
We derived the relative risk of not breast feeding and not exclusively breast feeding at last study follow-up along with 95% confidence intervals and explored both clinical heterogeneity (by qualitatively comparing their characteristics among included studies) and statistical heterogeneity (using χ2 tests of heterogeneity and the I2 statistic to measure heterogeneity15). We combined results from included studies for each outcome to give an overall estimate of the treatment effect using random effects models throughout. For cluster trials we computed the design effect from data presented in the reports (intraclass correlation coefficients and cluster adjusted estimates) and adapted the standard errors of the relative risk to make appropriate allowance for clustering.14 For example, consider one scenario with a high continuation of breast feeding of 50% and another where continuation is less common, such as 20%. If peer support yielded a relative risk of 0.5 for not continuing breast feeding, this would predict that 25% (0.5×50%) more women (a total of 75%) would breast feed in the first scenario and 40% (0.5×80%) more (a total of 60%) in the second. The absolute benefit of the intervention would be largest in the scenario where most improvement could be made. This seems more tenable than the converse obtained by considering a relative risk of 2.0 for continuing breast feeding, which predicts increases in breast feeding of 50% (a total of 100%) in the first scenario compared with a smaller absolute increase of only 20% (a total of 40%) for the second scenario. Where intraclass correlation coefficients were not reported we computed a design effect using the mean intraclass correlation coefficient from the trials in which they were available.
We explored three a priori hypotheses for the differences in the effect of peer support on any and exclusive breast feeding: setting (high income and middle or low income countries16), intensity of the peer support intervention (<5 or ≥5 planned contacts); and timing of the support (antenatal and postnatal or postnatal only). For each hypothesis we subgrouped studies according to their characteristics and we used a random effects metaregression model to determine the significance of differences in effect between the subgroups for both outcomes. Owing to the restricted number of trials we entered only one covariate in each analysis. We investigated the effectiveness of peer support in the United Kingdom using meta-analysis only, not metaregression. This separate analysis was justified given the policy recommendation for peer support in the United Kingdom, against a highly developed routine community postnatal care service. For all analyses we used the metan and metareg functions in Stata (version 11).
Results
The search identified 2160 citations, of which 612 duplicates and review articles were excluded. Screening identified 32 potentially relevant citations for which full text articles were obtained and assessed for eligibility. Seventeen were eligible and included in the review,6 8 9 10 17 18 19 20 21 22 23 24 25 26 27 28 29 30 but only 15 had data that enabled inclusion in the quantitative syntheses. Data in two studies could be included only descriptively in the review (fig 1⇓).9 17 A large cluster randomised controlled trial reported its results separately for the three study countries,18 owing to differences in population breastfeeding rates, provision of healthcare, and population characteristics. The data for each country are included as separate studies in the meta-analyses.18

Fig 1 Identification of relevant literature on peer support to improve breastfeeding rates
{kind=link}
Description of studies
Four studies were based in the United Kingdom, five in the United States,17 19 20 21 22 two in Canada,23 24 two in Brazil,25 26 and one each in Mexico,27 Bangladesh,28 the Philippines,29 and sub-Saharan Africa (in Burkina Faso, Uganda, and South Africa)18 (table 1⇓). The number of planned contacts ranged from one to 10 or more, with five studies categorised as “less intensive” (<5 planned contacts)6 9 10 21 27 and 12 as “intensive” (≥5 contacts planned). The implementation of the peer support interventions was often poorly reported, with only five trials reporting both the number of contacts received and the proportion of women in the intervention groups who received some peer support.6 10 21 23 25 Six of the studies reported neither the number of actual contacts received nor the overall uptake of the intervention.18 24 26 27 28 29 Of the 17 studies, nine reported a peer support intervention that spanned the antenatal and postnatal periods, whereas eight reported a postnatal intervention only and were thus in women who had all initiated breast feeding, and one was a postnatal intervention to women with a baby on the neonatal intensive care unit who intended to breast feed.
Characteristics of included studies
In all but four of the 17 trials the peer supporters had previously breast fed a baby: in the others9 21 25 27 this was not specifically stated but is likely to have been the case in those countries where breastfeeding initiation rates are high. Peer supporters were also of similar age,22 culture,23 language,21 ethnicity,10 24 education, or socioeconomic status,23 25 or lived in the same locality as the women.9 18 Some of the peer supporters were paid employees,10 17 20 21 some received an honorarium28 or payment per visit,8 26 and others described the peers as volunteers, without a description of the payment.9 23 24 Apart from one trial,21 all trials offered peer support at home, usually in person, although in two trials support was by telephone.23 24 The training of the peer supporters ranged from two and a half hours plus a handbook23 up to an eight week course10 and was unspecified in only two trials.6 29
Risk of bias in included studies
Several studies did not give sufficient information to assess risk of bias in detail (table 2⇓). Sequence generation was generally adequately described, but concealment of the random allocation was less well described. Eight studies reported taking measures to blind those involved in the outcome assessment. Losses to follow-up ranged from 1% to 41% but were generally balanced across study arms, with only one study having a difference of more than 10% in follow-up rate between study arms,17 and in most studies characteristics were balanced between arms at baseline. One study did not undertake an intention to treat analysis, with exclusion of those who did not receive the intervention in the analysis.17
Assessment of risk of bias
Overall effect of peer support on breast feeding
Thirteen of the studies reported the outcome of any breast feeding. Overall, compared with usual care those allocated to peer support had a 15% significantly lower risk of not breast feeding at the last follow-up (relative risk 0.85, 95% confidence interval 0.77 to 0.94), but with significant heterogeneity: χ2=31.3 (P=0.002), I2=61.7%.
Twelve of the studies reported on exclusive breast feeding. Compared with usual care those allocated to peer support had an 18% significantly lower risk of not breast feeding exclusively at the last follow-up (0.82, 0.76 to 0.88), with significant heterogeneity: χ2=127, (P<0.001), I2=89.7%
One study17 reported a significant increase in any breast feeding in the mothers allocated peer support (odds ratio 2.81, 95% confidence interval 1.11 to 7.14), but not exclusive breast feeding (1.30, 0.30 to 6.65). Another study reported no difference in exclusive breast feeding at four months post partum.9
Setting
The relative risk of not breast feeding at last study follow-up in women allocated peer support was 30% lower than usual care in studies from low or middle income countries (relative risk 0.70, 95% confidence interval 0.60 to 0.81), but only 7% lower in studies from high income countries (0.93, 0.87 to 1.00) and specifically only 4% lower in studies from the United Kingdom (0.96, 0.89 to 1.04) (table 3⇓, fig 2⇓). Peer support interventions significantly reduced the risk of not exclusively breast feeding at last study follow-up compared with usual care in both high income countries and low or middle income countries, although the risk reduction of 37% in the setting of low or middle income countries was considerably larger than the 10% observed in high income countries (table 3, fig 3⇓). No significant effect was seen in the UK only trials (0.98, 0.96 to 1.01). This finding was supported by one study.9 The metaregression analysis showed that these differences in the effectiveness of the peer support intervention between high income countries and low or middle income countries were significant for both the any breastfeeding outcome (P<0.001) and the exclusive breastfeeding outcome (P=0.01).

Fig 2 Relative risk of not breast feeding at last study follow-up by setting
{kind=link}
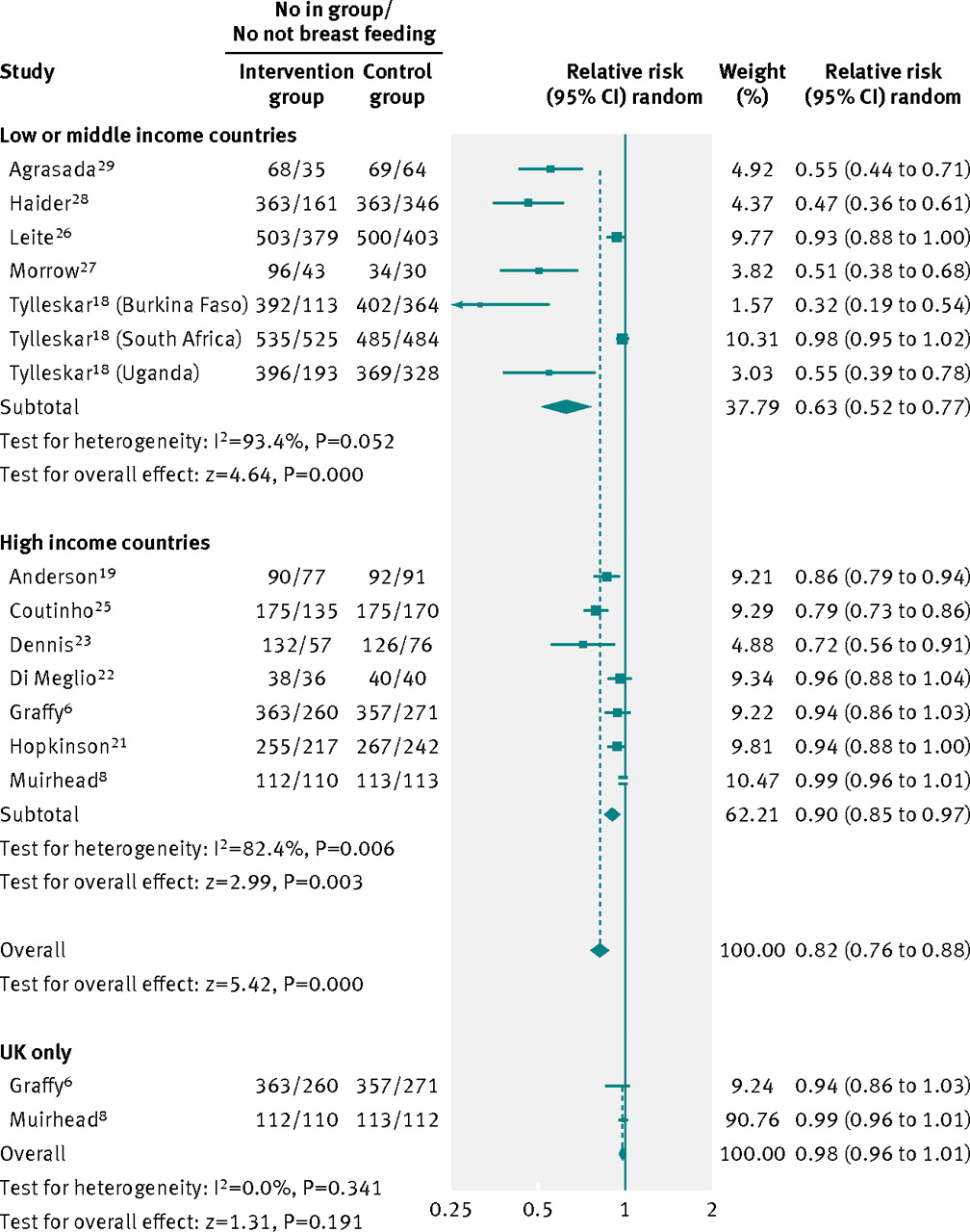
Fig 3 Relative risk of not exclusively breast feeding at last study follow-up by setting
{kind=link}
Relative risk of not breast feeding at last study follow-up
Intensity
Women in the more intensive interventions (≥5 contacts planned) had a significantly lower risk of not breast feeding at last follow-up compared with usual care (0.79, 0.71 to 0.89), whereas the less intensive interventions were not associated with lower rates of not breast feeding (0.99, 0.90 to 1.09) (table 3, fig 4⇓). This difference was significant in the metaregression analyses (P=0.02). The impact of the intervention on exclusive breast feeding (fig 5⇓) did not show a relation with intensity, the reductions in risk compared with usual care being similar (20% and 17%) in the two subgroups, and the small difference in the relative risk not being significant (P=0.73).

Fig 4 Relative risk of not breast feeding at last study follow-up by intensity
{kind=link}

Fig 5 Relative risk of not exclusively breast feeding at last study follow-up by intensity
{kind=link}
Timing of support
Combined antenatal and postnatal peer support was not associated with a significant improvement in not breast feeding at last study follow-up (0.94 0.88 to 1.01), whereas postnatal only interventions did significantly reduce not breast feeding (0.75, 0.63 to 0.89). Metaregression showed this difference to be significant (P<0.001). Combined antenatal and postnatal and postnatal only peer support interventions compared with usual care significantly reduced the risk of not exclusively breast feeding by a similar magnitude (table 3, figs 6⇓ and 7⇓).

Fig 6 Relative risk of not breast feeding at last study follow-up: timing of support
{kind=link}

Fig 7 Relative risk of not exclusively breast feeding at last study follow-up: timing of support
{kind=link}
Discussion
Our systematic review provides important clarification on the inconsistency of effects observed in trials of peer support for breast feeding in different settings, which is critical for generating guidance. We assessed the evidence from randomised controlled trials that compared breastfeeding continuation in women offered a peer support intervention, according to setting, intensity, and timing compared with usual care. Analyses according to setting clarify that peer support is effective in low or middle income countries and especially for exclusive breast feeding, which is critical in these settings. Our findings indicate, however, that peer support is likely to be ineffective for increasing breastfeeding rates in high income countries, in particular in the United Kingdom. Peer support provided at a low intensity (<5 planned contacts) seems to be ineffective for any breast feeding.
Comparison with existing literature
This review focused on the effectiveness of peer support on breast feeding, whereas previous reviews have included any lay support.4 11 Both these reviews reached similar conclusions to our overall findings and expressed caution in interpretation of the analysis of pooled data owing to the low quality of reporting of many of the trials4 and the heterogeneity identified.11 Neither review explored possible reasons for the heterogeneity, however, which we have done using prespecified categories of setting, intensity, and timing of support.
Peer support has been defined as “the provision of emotional, appraisal and informational assistance by a created social network member who possesses experiential knowledge of a specific behaviour or stressor and similar characteristics as the target population.”30 The overlap between the definitions of peer and lay support is considerable and the terms are often used interchangeably. In most cases the peers in our included trials shared the experience of motherhood and previous breast feeding, whereas in other trials language, ethnicity, age, and locality were the criteria for being a peer. Almost all of the trials of lay support were of peers, but a retrospective sensitivity analysis, which included trials of lay support as well as of peer support, did not alter our findings. Other trials have used peers in the provision of a structured educational programme31 or lay workers in complex interventions in which breast feeding was a minor component,32 33 which were not included within our definition of peer support.
The lack of effect of peer support on any or exclusive breast feeding in the UK trials and on any breast feeding in high income countries may well be a result of the amount of support for breast feeding provided as part of standard postnatal care. Even in some highly developed countries, such as Canada, little postnatal breastfeeding support is routinely provided by the health service. Most trials reported support for breast feeding in hospital, but many then described usual care, which requires women to specifically initiate contact to obtain support if they have difficulties with breast feeding. One study in the United States, for example, described the first routine postnatal contact to be at two weeks, after the period when many women give up breast feeding owing to difficulties such as positioning, discomfort, or insufficient milk.34 35 This was not the case for the trials in the United Kingdom, where home based midwifery support is provided routinely up to at least 10 days postnatally, and health visitors provide routine support after this time.
In the UK trials peer support was generally less intensive, with one trial not reporting this,8 and, apart from another trial,9 included antenatal support in addition to postnatal support. Some confounding of setting by intensity of support may exist because three of the five trials of a low intensity intervention were in the United Kingdom and only one in a low to middle income country. We do not know whether more intensive interventions in the United Kingdom might be effective, but they would necessarily be more costly if the peers were paid. Whether peer support targeted at women who have not breast fed before or who have no experience of breast feeding in their social groups might be of benefit is another question to be answered in the United Kingdom and other high income countries.
The effectiveness of peer support in increasing continuation of any and particularly exclusive breast feeding in low or middle income countries is critical. Breast feeding has been associated with significantly reduced deaths from neonatal sepsis36 and deaths from diarrhoea and acute respiratory tract infections in the first six months of life.37 Exclusive breast feeding, for which peer support had a substantial effect in low or middle income countries, is associated with a reduction in gastrointestinal infections,38 39 longer periods of maternal lactational amenorrhoea,40 and a non-significant reduction in infant growth at six months.40 Thus peer support should contribute towards the Millennium Development Goal 4 of reducing child mortality in under 5s. To put into context the effectiveness of peer support for increasing exclusive breast feeding in low or middle income countries, we calculated the number needed to treat for an additional woman to be exclusively breast feeding at six months. Assuming a rate of not exclusively breast feeding of 90% in the population, which is similar to that reported in several of the trials included in this review,18 26 27 29 and a relative risk of 0.63 (fig 3), three women would need to receive peer support for one additional woman to be practising exclusive breast feeding at six months.
That peer support provided in both antenatal and postnatal periods is ineffective at increasing any breast feeding is counterintuitive. This is probably because most trials that span both periods are also aimed at increasing breastfeeding initiation, thus the populations encompass much less motivated women. Those trials of only postnatal support are usually targeted at women who have already initiated breast feeding. In addition this comparison is confounded by setting since most women in low or middle income countries initiate breast feeding.
Strengths and limitations of the review
This review followed contemporary recommended methods.12 Searching was systematic and not limited by language of publication. To reduce the potential for confounding we restricted the review to randomised controlled trials.
The trials within this review used a range of definitions of exclusive breast feeding, most following the WHO definition, but others used less robust definitions, such as limitation to the previous week18 27 or no more than other liquids twice a week,21 which may affect this outcome. Support for breast feeding provided to the usual care groups was rarely well described, making it difficult to interpret fully the reasons for differences between trials and countries in the effectiveness of peer support. Although the intended schedule of contact by the peer supporters was usually described, the actual coverage8 24 26 27 28 29 and intensity of support8 17 19 20 24 26 27 28 29 was often not reported. It is thus hard to determine in some cases whether a lack of effect was due to ineffectiveness or to a low uptake of the intervention. We therefore had to use the planned intensity of support for our analyses. The lack of data on implementation of the interventions is a particular feature of peer support, possibly because of the nature of being a peer and sometimes a volunteer, rather than professionals who are used to recording activity. One trial from the United Kingdom9 that aimed to increase exclusive breast feeding as a secondary outcome to improving infant nutrition, did not start the peer support until after 10 weeks post partum, which limited the duration of this support. The results of this trial are only presented descriptively but are consistent with the findings of the other UK trials.
The trials set in low or middle income countries were more likely to focus on exclusive breast feeding, as the health gains are likely to be much greater in these settings. However, these countries are also less likely to have highly developed universal healthcare incorporating routine postnatal support and peer support is likely to have its greatest impact when compared with no routine support. It is therefore possible that the greater effect size for exclusive breast feeding is due to confounding by setting.
We used the outcome of “not breastfeeding at last study follow-up,” which was at three to six months for all but two of the trials, where follow-up was shorter. Sensitivity analyses to remove any possible bias that might have occurred as a result of differing follow-up durations were undertaken excluding the trials with shorter follow-up.21 22 The results remained much the same, except that relative risk of not exclusively breast feeding in not intensive interventions just reached statistical significance (relative risk 0.90, 95% confidence interval 0.83 to 0.98). Selecting the last study follow-up may also fail to show a shorter term effect on breastfeeding rates when the intervention was of short duration.
Implications for future research or clinical practice
Although overall, peer support interventions seem to be associated with increases in any and exclusive breast feeding, considerable inconsistency exists and seeking explanation for this is critical for public health policy.41 In low or middle income countries, peer support interventions are effective in increasing continuation of exclusive breast feeding and should be recommended. However, peer support interventions may not be effective where routine services to support breast feeding are already established, as in the United Kingdom or in some other high income countries. Policy relating to provision of peer support needs to be based on more context specific evidence. Alongside implementing such programmes in high income countries we strongly recommend a robust evaluation of outcomes.
What is already known on this topic
Meta-analyses of lay support for increasing breastfeeding rates suggest an effect on both any and exclusive breast feeding
These meta-analyses, however, showed considerable heterogeneity, which has not been investigated
What this study adds
In low or middle income countries, peer support interventions are effective in increasing continuation of exclusive breast feeding and should be recommended
Peer support interventions, however, may not be effective where there are routine services already established to support breast feeding, as in the United Kingdom or in some other high income countries
New peer support services in high income countries need to undergo concurrent evaluation
Notes
Cite this as: BMJ 2012;344:d8287
Footnotes
We thank T Tylleskar and colleagues for sharing the results of their study before publication.
Contributors: KJ, CM, KSK, and LI conceived the study. LI designed the search strategy. LI and KJ selected the papers for inclusion and abstracted the data. CM and KSK resolved differences in inclusion and abstraction. JJD and NF provided advice about the meta-analysis. JJD, KJ, and LI undertook the meta-analyses. KJ, CM, and LI wrote the first draft. All authors commented on and approved the final version. KJ is the guarantor.
Funding: KJ, CM, and LI are part funded by the National Institute for Health Research through the Collaborations for Leadership in Applied Health Research and Care for Birmingham and Black Country (CLAHRC-BBC) programme. The views expressed in this publication are those of the authors and not necessarily those of the National Institute for Health Research, the Department of Health, University of Birmingham, University College London, or the CLAHRC-BBC steering group.
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; CM, KJ, KSK, NF, and LI were investigators of one of the included trials.
Ethical approval: Not required.
Data sharing: No additional data available.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.