Effect of statins on atrial fibrillation: collaborative meta-analysis of published and unpublished evidence from randomised controlled trials
BMJ 2011; 342 doi: https://doi.org/10.1136/bmj.d1250 (Published 16 March 2011) Cite this as: BMJ 2011;342:d1250
- Kazem Rahimi, James Martin senior fellow in essential healthcare1, cardiologist2,
- Jonathan Emberson, statistician3,
- Paul McGale, statistician3,
- William Majoni, nephrologist4,
- Amal Merhi, statistician3,
- Folkert W Asselbergs, cardiologist567,
- Vera Krane, nephrologist8,
- Peter W Macfarlane, emeritus professor9
- PWM is acting on behalf of the PROSPER Executive
- Correspondence to: K Rahimi kazem.rahimi{at}cardiov.ox.ac.uk
- Accepted 24 December 2010
Objective To examine whether statins can reduce the risk of atrial fibrillation.
Design Meta-analysis of published and unpublished results from larger scale statin trials, with comparison of the findings against the published results from smaller scale or shorter duration studies.
Data sources Medline, Embase, and Cochrane’s CENTRAL up to October 2010. Unpublished data from longer term trials were obtained through contact with investigators.
Study selection Randomised controlled trials comparing statin with no statin or comparing high dose versus standard dose statin; all longer term trials had at least 100 participants and at least six months’ follow-up.
Results In published data from 13 short term trials (4414 randomised patients, 659 events), statin treatment seemed to reduce the odds of an episode of atrial fibrillation by 39% (odds ratio 0.61, 95% confidence interval 0.51 to 0.74; P<0.001), but there was significant heterogeneity (P<0.001) between the trials. In contrast, among 22 longer term and mostly larger trials of statin versus control (105 791 randomised patients, 2535 events), statin treatment was not associated with a significant reduction in atrial fibrillation (0.95, 0.88 to 1.03; P=0.24) (P<0.001 for test of difference between the two sets of trials). Seven longer term trials of more intensive versus standard statin regimens (28 964 randomised patients and 1419 events) also showed no evidence of a reduction in the risk of atrial fibrillation (1.00, 0.90 to 1.12; P=0.99).
Conclusions The suggested beneficial effect of statins on atrial fibrillation from published shorter term studies is not supported by a comprehensive review of published and unpublished evidence from larger scale trials.
Introduction
Atrial fibrillation is the most common form of cardiac arrhythmia in clinical practice and its prevalence increases with age.1 In England and Wales, for instance, it has been estimated that about 0.7% of men and 0.4% of women aged 45-54 are affected, but these proportions rise to about 9% and 7%, respectively, by age 75-84.2 Moreover, because of increases in life expectancy in most countries, as well as consequent increases in the prevalence of heart failure, the overall global burden from atrial fibrillation is likely to increase substantially in the coming decades. Although not acutely life threatening, the haemodynamic compromise and increased risk of stroke associated with chronic atrial fibrillation1 3 can cause severe morbidity and mortality (especially among older people4 and those with heart failure5). Atrial fibrillation is therefore responsible for much impairment of quality of life6 and causes a substantial burden to health services,7 but there is little reliable evidence from large scale randomised controlled trials about how to prevent it.8
Recently, there has been some evidence for the protective role of statins in reducing the risk of atrial fibrillation. In particular, one meta-analysis identified six trials involving 386 events (165 statin v 221 control) and suggested that statins could reduce the risk of atrial fibrillation by 61% (95% confidence interval 15% to 82%).9 A second meta-analysis comprising six trials (five of which were included in the first meta-analysis), however, yielded a more modest (and non-significant) point estimate of 24% (−5% to 45%; 177 statin v 220 control).10 In both meta-analyses, the findings from the included trials were highly heterogeneous, and the highly selected populations of patients in these trials raised questions about the applicability of the findings to much larger populations at risk of atrial fibrillation. Thus, many experts have called for more research, acknowledging that the conduct of large scale randomised statin trials with atrial fibrillation as the primary outcome could pose numerous practical, financial, and ethical challenges.8 In the absence of such trials, the wealth of available information from many large scale randomised controlled trials that have collected but not necessarily published information on atrial fibrillation offers an opportunity to test the hypothesis generated by the previous meta-analyses.
We investigated whether longer term treatment with statins can reduce the risk of atrial fibrillation in a wide range of people by performing a meta-analysis of published and unpublished findings from all larger scale statin trials, many of which were conducted in populations at risk of atrial fibrillation because of underlying cardiac disease.
Methods
Search strategy for identification of relevant studies
We searched Medline (January 1966 to October 2010), Embase (January 1985 to 2010 week 40), and the Cochrane Central Register of Controlled Trials (Cochrane Library, issue 4, October 2010) for articles with a subject term “hydroxymethylglutaryl-coenzyme A reductase inhibitor” or any of the following terms: “hydroxymethylglutaryl-co A reductase inhibitor”, “statin”, “fluvastatin”, “pravastatin”, “lovastatin”, “simvastatin”, “atorvastatin”, or “rosuvastatin”. The search was limited to randomised controlled trials with no language restrictions.
Review methods and selection criteria
Two reviewers independently screened all titles and abstracts for randomised controlled trials with either a parallel or factorial design, at least one comparison of a statin versus a control regimen or a more versus less intensive statin regimen, and a total of 100 or more randomised participants followed up for at least six months. There were no restrictions on participants’ characteristics or study outcomes. We also hand searched the reference lists of these studies to ensure that we did not miss other relevant articles, such as meta-analyses of statin trials or other types of articles related to statins and cardiac arrhythmias. After removing duplicate reports, we examined full text articles of all remaining reports (fig 1⇓).

Fig 1 Search retrieval process for studies of statins
{kind=link}
Data abstraction
For each trial, we recorded the study’s or investigator’s name; mean duration of follow-up; year of publication of the primary findings; randomised treatments; summary information about the studied population (number of participants, mean age, number of men, and prevalence of myocardial infarction or heart failure at randomisation); and the primary outcome of the study. The number of patients with at least one reported episode of atrial fibrillation was recorded. In trials where information on atrial fibrillation had not previously been published, we asked the investigators to abstract the relevant numbers from their routine records of adverse events. Non-responders were sent a reminder after about three weeks and, when possible, were then contacted by telephone.
Updated search for short term trials
The two previous meta-analyses (both published in 2008)9 10 included statin trials that had previously published results on atrial fibrillation. Because these meta-analyses were themselves a few months old by the time our search for the longer term trials began, we also performed an updated search for any smaller published statin trials that had reported on atrial fibrillation and were published since the data search in the previous meta-analyses up to October 2010. Unpublished data from trials that did not have at least 100 participants randomised and at least six months’ follow-up were not sought.
Assessment of risk of bias
To identify potential sources of bias in the reported events of atrial fibrillation (according to the Cochrane Statistical Methods Group and the Cochrane Bias Methods Group) we considered sequence generation, concealment of allocation sequence, blinding, incomplete outcome data, selective outcome reporting, and any other potential sources of bias. Risk of bias at the individual trial level and across the two sets of trials was categorised into low, unclear, and high.
Statistical analysis
Our primary hypothesis was to test whether longer term treatment with statins reduces the risk of atrial fibrillation. We therefore considered the shorter term trials included in the two previous meta-analyses (as well as any further short term trials) separately from the longer term statin trials. Although the previous two meta-analyses had no restriction on the size or duration of the trials included, none of the trials included in those meta-analyses (or the six found subsequently) had a planned treatment duration of more than six months and a sample size of 100 or more participants, so our electronic searches identified a non-overlapping group of longer term trials. Our primary analyses were restricted to trials of statin versus control (that is, placebo or usual care). As the anti-inflammatory effect of statins—one of the key mechanisms for their potential anti-arrhythmic effects11 12—might be more pronounced in high dose statin treatment,13 we also carried out secondary analyses based on the trials that had compared a more intensive versus a standard statin regimen.
For every trial, we calculated the “observed minus expected” statistic (O−E) and its variance (V) from the number of patients who developed atrial fibrillation and the total number of patients in each treatment group, using standard formulas for 2×2 contingency tables. These (O−E) values, one from every trial, were summed to produce a grand total (G), with variance (V) equal to the sum of their separate variances. The value exp(G/V) is Peto’s “one step” estimate of the odds ratio, and its continuity corrected 95% confidence interval is given by exp(G/V ± (0.5/V + 1.96/√V)).14 Odds ratios are given with 95% confidence intervals for the overall results and with 99% confidence intervals (replacing 1.96 in the formula above by 2.576) for individual trial results and subgroup results. We assessed the heterogeneity between the different hypothesis testing trials by calculating S−G2/V, where S is the sum of (O−E)2/V for each trial, and testing this statistic against a χ2 distribution with degrees of freedom equal to one less than the number of trials. In forest plots, trials are shown in order of the amount of statistical information they contribute to the overall result. The summary odds ratios from the two sets of trials were compared with a standard χ2 test (on 1 degree of freedom).
To assess the potential for a differential effect of statins on atrial fibrillation in different clinical settings, we performed two separate subgroup analyses among the statin versus control trials. One assessed the effect of statins separately among trials in which reports were known to have been of first diagnosed episodes of atrial fibrillation, trials in which reports were known to have been recurrences of previously diagnosed paroxysmal atrial fibrillation, and trials in which it was unknown whether reports were first diagnosed or recurrent events. The other subgroup analysis tested whether the effect of statins might differ in people at different underlying risk of atrial fibrillation by looking at the treatment effects separately for three groups of trials, according to the predominant type of participants: patients without previous coronary heart disease, patients with previous coronary heart disease, and patients with known heart failure or end stage renal disease. (Trials that largely included patients with heart failure or end stage renal disease were considered together because of the large clinical overlap between these two groups of patients: heart failure is highly prevalent in people with kidney failure,15 and both groups are at increased risk of atrial fibrillation.16 17)
Statistical analyses were done with R version 2.2.1.18 All statistical tests were two sided, and all analyses were done on an intention to treat basis.
Results
Shorter term trials
The two previous meta-analyses9 10 contained data on seven trials,19 20 21 22 23 24 25 yielding a total of 3608 randomised patients and about 1050 person years of follow-up (0.3 years per patient). In addition, we identified six further statin trials that had published data on atrial fibrillation (but were not eligible to be considered as long term trials) (table 1)⇓.26 27 28 29 30 31 With the exception of one trial, all shorter term trials were restricted to patients in whom cardiac surgery or electrical cardioversion was planned. Most short term trials used sensitive event capturing methods and included short episodes of atrial fibrillation on continuous electrocardiographic monitoring as relevant study outcomes regardless of presence or absence of symptoms. The potential risk of bias was judged to be high in four of the trials and unclear in a further four.
Summary of characteristics of short term trials on effect of statins
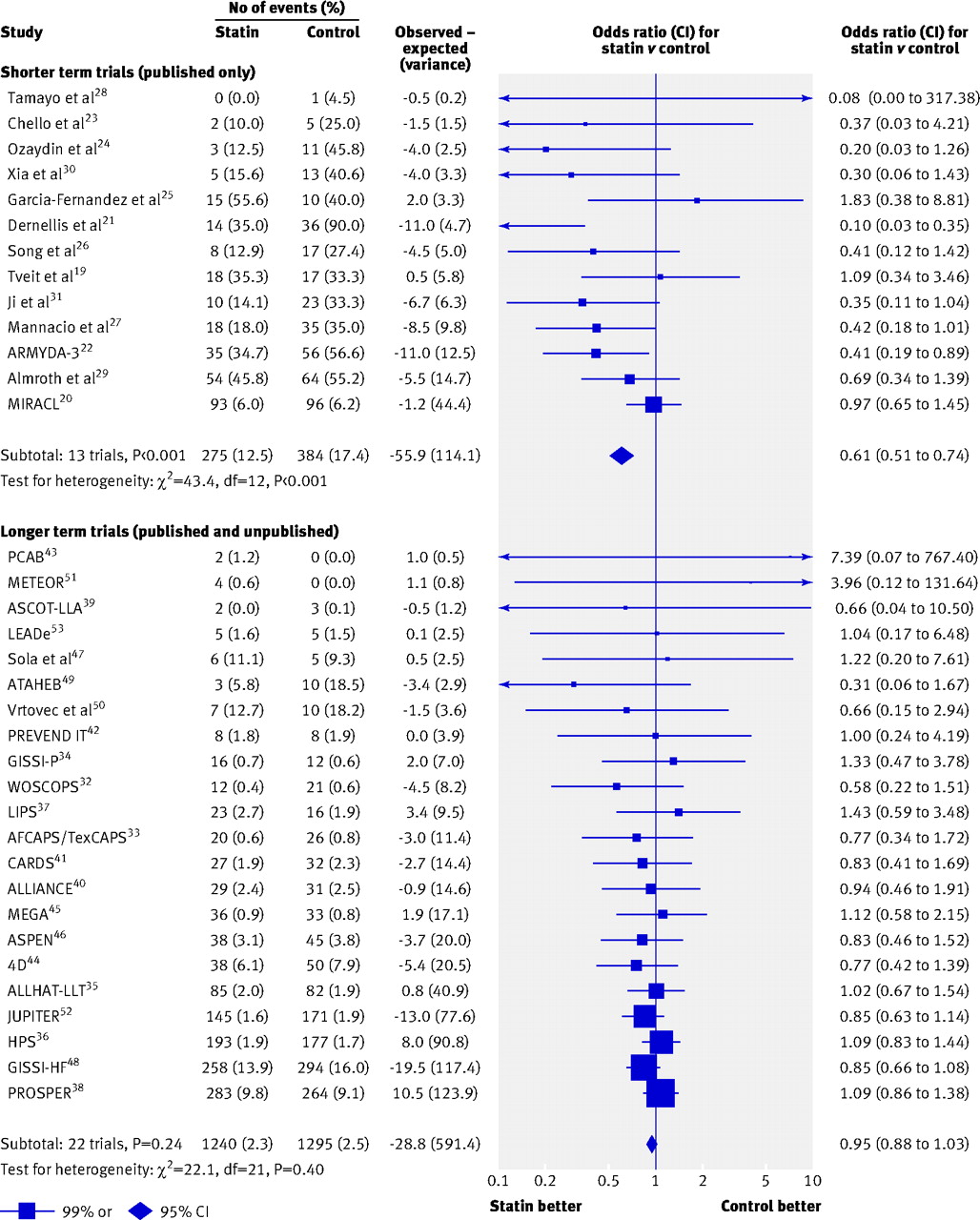
In the 13 shorter term trials combined (4414 patients, 1129 person years of follow-up), a report of atrial fibrillation on at least one occasion during follow-up occurred among 659 patients (fig 2)⇓. Within these trials, treatment with statins was associated with a reduced odds of atrial fibrillation, by 39% (275 (12.5%) in the statin group versus 384 (17.4%) in the control group (odds ratio 0.61, 95% confidence interval 0.51 to 0.74; P<0.001; fig 2⇓). There was significant heterogeneity between the trials (χ2=43.4, df=12, P<0.001), caused in part by one study with an extreme relative reduction in the odds of atrial fibrillation (14 (35%) v 36 (90%); continuity corrected χ2=23.2, df=1, P<0.001).21 Even within the 12 other trials, however, we observed a highly significant 34% reduction in the odds of atrial fibrillation (261 v 348; 0.66, 0.55 to 0.81), albeit still with significant heterogeneity between these 12 trials (χ2=26.9, df=11, P<0.001). In the largest trial, there was no significant reduction in risk (93 (6.0%) v 96 (6.2%) events; P=0.86).20 Exclusion of the four trials in which the potential for bias was thought to be high had little effect on the estimated odds ratio in the remaining nine trials (249 v 345; 0.62, 0.51 to 0.76).

Fig 2 Effect of statin treatment on atrial fibrillation in 13 shorter and 22 longer term trials of statin v control (test for difference: χ2=18.6, df=1, P<0.001)
{kind=link}
Longer term trials
Out of 4033 abstracts reviewed, we retrieved 218 papers describing 101 longer term trials for further examination, 79 of which met the inclusion criteria (fig 1)⇑. Of these 79 trials, atrial fibrillation was not recorded in 23 (18 000 patients and 68 000 person years) and data were not readily available to the investigators in 18 (21 000 patients, 83 000 person years). Of the remaining 38 trials, all except nine were included in the current meta-analysis (there was no response to our request for data for seven trials (4900 patients, 5900 person years), and information was not available in two trials because of restrictions on sharing unpublished data (10 000 patients, 37 000 person years)). Of the 29 included trials,13 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 six provided data on atrial fibrillation in the published reports32 48 49 54 57 and investigators in the remaining 23 provided the data on request. There were no obvious systematic differences between the trials that were and were not included.
Tables 2 and 3 show the characteristics of the 29 longer term trials.⇓ ⇓ Twenty two trials (including 105 791 randomised participants and 410 000 person years of follow-up) compared a statin with a control regimen and seven trials (including 28 964 randomised participants and 110 000 person years of follow-up) compared a more intensive with a standard statin regimen. Event information was mostly based on routinely collected data on adverse events, with the exception of six trials that used periodic electrocardiography, including at the end of the study,32 35 38 41 42 48 and one study that used a prespecified definition of atrial fibrillation based on pacemaker interrogation.49 Nine trials confirmed reports of atrial fibrillation.32 35 38 41 42 48 49 54 Of these, seven recorded baseline information about the presence or absence of atrial fibrillation (either as a clinical history or on ECG evidence) and hence could confirm that the numbers provided were first diagnosed occurrences of atrial fibrillation32 35 38 41 42 48 49 or definite recurrences of known paroxysmal atrial fibrillation.48 In all other trials, such information was not available, so a subset of the reported events could represent symptomatic recurrences of previously diagnosed atrial fibrillation. The potential risk of bias in the longer term trials was judged to be low in all but one trial.49 Exclusion of this trial had no effect on the results (as it contributed just 13 events).
Summary of characteristics of longer term (with at least six months’ follow-up) hypothesis testing trials: statin versus control regimen
Summary of characteristics of longer term (with at least six months’ follow-up) hypothesis testing trials: more intensive versus less intensive statin treatment
The primary analyses were restricted to the 22 longer term trials that compared a statin with a control regimen. In these trials, 2535 patients experienced an episode of atrial fibrillation. Statin treatment did not significantly reduce the risk of atrial fibrillation (1240 (2.3%) statin v 1295 (2.5%) control, odds ratio 0.95, 0.88 to 1.03; P=0.24), and there was no evidence that the effect of statin treatment varied within these trials (heterogeneity χ2=21.9, df=21, P=0.40; fig 2⇑). An uncorrected test of the combined results from the 13 short term and 22 long term trials would not be statistically appropriate because seven out of the 13 shorter term trials generated the hypothesis being tested in the longer term trials (which could lead to a point estimate, confidence interval, and P value that are appreciably biased).59 60 Consequently, the suggestion of a small reduction in risk when all 35 trials are considered together (0.89, 0.82 to 0.95; P=0.002) should be interpreted with caution.
In the seven longer term trials that examined a more intensive compared with a standard statin regimen, there was no evidence that higher dose statin reduced the risk of atrial fibrillation compared with standard dose statin (710 (4.9%) v 709 (4.9%), respectively; 1.00, 0.90 to 1.12; P=0.99; fig 3⇓).

Fig 3 Effect of statin treatment on atrial fibrillation in seven longer term trials of more intensive v standard statin regimens
{kind=link}
In subgroup analyses, there was no evidence that statin treatment was effective in preventing first diagnosed atrial fibrillation (574 (4.1%) statin v 597 (4.3%) control; fig 4⇓), and there was no evidence that the effect of statin treatment differed in trials that studied mainly people with no previous coronary heart disease, mainly people with previous coronary heart disease, or mainly people with heart failure or advanced chronic kidney disease (χ2=5.05, df=2, P=0.08 for heterogeneity between these three categories; fig 4⇓). Most of the longer term trials of statin versus control reported events that were not adjudicated, but when the analyses were restricted to those seven trials that had independently confirmed the events,32 35 38 41 42 48 49 there was also no significant reduction in the risk of atrial fibrillation (676 (4.7%) statin v 711 (5.0%) control; 0.94, 0.84 to 1.05; P=0.29).

Fig 4 Effect of statin treatment on atrial fibrillation in 22 longer term trials of statin v control, by subgroups of trial population. *Six trials could confirm that reported atrial fibrillation events were new (that is, incident) cases,32 35 38 41 42 49 and one trial48 provided atrial fibrillation events in both those with and without history of paroxysmal atrial fibrillation at baseline. †No previous coronary heart disease32 33 35 38 39 41 42 45 46 49 51 52 53; previous coronary heart disease34 36 37 40 43; previous heart failure or renal disease44 47 48 50
{kind=link}
Discussion
Despite previous suggestions, this meta-analysis of published and unpublished information from larger scale trials found no evidence for the use of statins in the prevention of atrial fibrillation. During recent years, statins have emerged as one of the most effective treatments to reduce the burden of cardiovascular disease worldwide.61 Because of their remarkably good safety profile and declining costs, there has been some interest in the potential use of statins as direct anti-arrhythmic or anti-inflammatory drugs.12 62 Various hypothetical mechanisms for such effects, mostly unrelated to their effects on low density lipoprotein particles (though still possibly dose related), have been proposed. The suggestion that such “pleiotropic effects” reduce atrial fibrillation by as much as one third, however, is not supported by our meta-analysis.
Interpretation of apparently contradictory findings
While several methodological and clinical differences between the shorter term and longer term trials preclude a meaningful combination of the results, they could help us understand the discrepant findings.
Firstly, the two sets of trials differed in methods of detection and verification of the outcome. The shorter term trials generally used more sensitive methods for event capturing than the longer term trials. For example, brief asymptomatic periods of atrial fibrillation that were detected on continuous cardiac monitoring were classified as events in some shorter term studies. In contrast, events in many of the longer term studies were based on clinical reports collected from adverse event forms that are more likely to be relevant to patients. In most longer term trials, atrial fibrillation was not a prespecified end point, and this might have resulted in underestimation of the true number of events and hence larger random errors in those particular studies.63 Such passive collection of event information is unlikely to have introduced any bias because under-reporting would be likely to occur similarly in each treatment group. The events in the longer term trials were also not generally adjudicated, but even when the analysis was restricted to those seven trials of statin versus control that had independently confirmed the events,32 35 38 41 42 48 49 there was no suggestion of a reduction in the risk of atrial fibrillation, indicating that lack of complete event adjudication is unlikely to have had a major impact on the results.
Secondly, the absolute risk of atrial fibrillation and the clinical condition of the patients included in the two sets of trials were quite different. Notwithstanding the differences in methods of event capturing used between the trials, the average underlying absolute risk of atrial fibrillation was higher in patients included in the shorter term trials than in those included in the longer term trials because of differences in selection criteria. While there is no a priori reason to suggest that absolute risk should influence the relative effect of treatment, it might sometimes help to explain some of the heterogeneity observed if, for example, it is associated with other biological or clinical factors that influence treatment effects. In the context of atrial fibrillation, future risk depends largely on the degree of atrial structural alterations (that is, atrial remodelling).64 If anything, drugs that are effective for the treatment of atrial fibrillation in people at low risk with a structurally normal heart might be expected to have less effect in those with structural abnormalities, as pre-existing atrial remodelling might be irreversible or less amenable to preventive medical treatment.65 We found no evidence that statins prevented atrial fibrillation in people with no history of heart disease, and there was no significant evidence of heterogeneity between trials that studied people at different underlying risk (fig 4⇑). With the exception of the MIRACL trial,20 all the shorter term trials selected either patients undergoing cardiac surgery, or electrical cardioversion, or patients with a history of atrial fibrillation. While it is unlikely that any potential pleiotropic effect of statins would be confined to these particular groups, there could be some other intermediary mechanisms that could, at least in part, account for the observed effect of statins in such settings. For example, myocardial damage is commonly encountered after coronary procedures66 and is a potential risk factor for atrial fibrillation.67 Therefore, a reduction in atrial fibrillation might result from just a short course of statin treatment if this abrogates myocardial tissue injury.27 68 In contrast with those undergoing cardiac surgery, however, the attributable risk for atrial fibrillation from coronary events in less selected populations of patients, such as those included in the longer term studies, is likely to be small. Thus, in the longer term studies any beneficial effects mediated through prevention of myocardial injury would be likely to be diluted by the much larger number of events that are unrelated to acute myocardial injury.
Thirdly, differences in selection criteria between the trials meant that the proportion of people with recurrences of known atrial fibrillation was much larger in the shorter term trials than in the longer term trials. The therapeutic goals in people with paroxysmal or persistent atrial fibrillation might differ from those with no known history of atrial fibrillation, as treatment in the former group is usually expected only to delay the next episode of atrial fibrillation or the transition to a permanent state. Although any such delays might be clinically valuable, in meta-analyses of longer term studies when information about timing of the events is not available, delays in recurrences are likely to be missed if a large proportion of individuals have experienced a recurrence by the end of the study. This might also obscure any beneficial effects on prevention of first diagnosed atrial fibrillation if recurrences of atrial fibrillation constitute a large proportion of total events. In the current analyses, however, we found no evidence that statins significantly reduced atrial fibrillation in the trials in which events were known to have been first diagnosed events (fig 4⇑). Furthermore, a pattern of early separation with a later convergence of risk curves was not reported in the longer term trials that provided a time based analysis.35 48
Fourthly, the differences between our findings and those of the earlier meta-analyses could be due, at least in part, to publication bias (that is, the tendency for trial results to be more likely to be published if they have strikingly positive results than if the results are negative or null).69 Publication bias can, along with other sources of bias, produce large apparent effects when treatments are actually ineffective, particularly when included studies are based on a limited number of events (as such studies are particularly susceptible to large random errors and hence much more likely than larger studies to lead to exaggerated estimates of treatment effect). Indeed, this point is perhaps well illustrated in the current context by the null findings of the MIRACL trial,20 which, despite being the largest study included in the earlier meta-analyses and despite being presented at a major medical conference in 2004, has not to our knowledge yet been published as a full report. In addition, the impact of the results from MIRACL on the overall estimates in the two previous meta-analyses9 10 was reduced because of the use of “random effect” approaches.
In the presence of heterogeneity, “random effect” approaches (which estimate the heterogeneity in treatment effects across trials and incorporate this variability into the estimate of the overall result) are commonly used. In certain circumstances, however, such approaches can lead to small potentially seriously biased studies gaining an inappropriately large statistical weight at the expense of larger more reliable studies.70 In contrast, we calculated our summary effect estimates by taking a simple weighted average of the like-with-like comparisons within each trial. While this method is often referred to as being a “fixed effect” method, the terminology is unsatisfactory because it misleadingly suggests that any heterogeneity between the true effects of treatment in different trials is assumed to be zero (whereas no such unjustified assumptions are involved). However, for comparison, when we applied a standard random effect to the meta-analysis of the 13 shorter term trials, the overall event rate ratio was 0.47 (0.30 to 0.72; P<0.001) and the difference between the overall results from the shorter and longer term studies remained significant (P<0.001).
Strength and limitations
Our meta-analysis sought to obtain both published and unpublished information from all eligible trials, and the large number of events this provided gave good statistical power to detect even modest treatment effects. We might still have missed relevant event information from at least nine further trials. It is unlikely that these data would have resulted in any material change to our primary conclusions, however, because they would have been expected only to have increased the total number of person years, and hence statistical information (that is, events), by about 10%. In addition, if an important reduction in atrial fibrillation had been observed in any single trial for which data were not made available to us, it seems likely that that result would have been published (as most of these trials were completed several years ago) and would hence have been identified by our literature search.
Conclusions and implications for clinicians and future researchers
In contrast with the unequivocal evidence for the beneficial effect of statins on atherosclerotic events in a wide range of people, there is currently no compelling evidence that longer term treatment with statins prevents atrial fibrillation. While our study does not exclude a real reduction in risk of about 10%, it casts doubt over the existence of any sustained and clinically relevant beneficial effect of statins for the prevention of atrial fibrillation. The effect of statins on atrial fibrillation in particular populations of patients with selection of outcomes that are relevant to patients and healthcare providers71 could be explored in future well designed randomised trials.
What is already known on this topic
Limited evidence from trials conducted in patients undergoing cardiac surgery or cardioversion suggests that statins might reduce the risk of atrial fibrillation by more than a third
What this study adds
A comprehensive review of both published and unpublished data from longer term trials showed no protective effect of statins on atrial fibrillation
Statins cannot currently be recommended for prevention of incident or recurrent atrial fibrillation
Notes
Cite this as: BMJ 2011;342:d1250
Footnotes
We are greatly indebted to the following people for their support and provision of unpublished data: D John Betteridge, Michiel Bots, Louise Bowman, Marco Bressers, Christopher Cannon, Rory Collins, Helen M. Colhoun, Luz Cubillos, Furio Colivicchi, Barry R Davis, David Demicco, Paul Durrington, Rana Fayyad, Howard H Feldman, John H Fuller, Wiek H van Gilst, Dick Goedhart, Antonio M Gotto Jr, Heather Halls, Graham Hitman, Lisa Holland, Bobby Khan, Robert Knopp, Michael Koren, John LaRosa, Lawrence Leiter, Aldo Maggioni, Haruo Makuuchi, Roberto Marchioli, Jennifer E Moon, Sabina A Murphy, Haruo Nakamura, Andrew Neil, Steven E Nissen, Terje Pederson, Sara Pressel, Paul Ridker, Patrick Serruys, Peter Sever, Sarah Sloan, Emiko Shimizu, Luigi Tavazzi, Chia-Ti Tsai, Bojan Vrtovec, Karl Wallendszus, Christoph Wanner, Alberto Zanchetti, and the PROSPER Executive (Gerard Blauw, Ed Bollen, Brendan Buckley, Ton van Craen, Ian Ford, J Wouter Jukema, Christopher Packard, Naveed Sattar, James Shepherd, David J Stott, Rudi Westendorp).
Contributors: KR designed the study. KR, WM, and PM reviewed the literature and extracted data. KR coordinated the collection of unpublished data. KR, JE, AM, and PM contributed to the statistical analysis. KR and JE drafted the initial report. All authors contributed to the interpretation of the results and the revision of the manuscript, and have approved the final version. KR is guarantor.
Funding: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. KR is supported by a senior fellowship from the James Martin School; JE acknowledges support from the BHF Centre of Research Excellence, Oxford (RE/08/004); and FWA is supported by a clinical fellowship from the Netherlands Organisation for Health Research and Development (ZonMw grant 90700342);
Competing interests: All authors have completed the Unified Competing Interest form at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare: no support from any organisation for the submitted work, no financial relationships with any organisations that might have an interest in the submitted work in the previous three years, no other relationships or activities that could appear to have influenced the submitted work.
Ethical approval: Not required.
Data sharing: No additional data available.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.