Use of weekly, low dose, high frequency ultrasound for hard to heal venous leg ulcers: the VenUS III randomised controlled trial
BMJ 2011; 342 doi: https://doi.org/10.1136/bmj.d1092 (Published 08 March 2011) Cite this as: BMJ 2011;342:d1092
- Judith M Watson, research fellow1,
- Arthur R Kang’ombe, trial statistician1,
- Marta O Soares, research fellow1,
- Ling-Hsiang Chuang, trial health economist1,
- Gill Worthy, statistician2,
- J Martin Bland, professor of health statistics1,
- Cynthia Iglesias, senior research fellow1,
- Nicky Cullum, professor, deputy head of department 1,
- David Torgerson, professor, director of York Trials Unit1,
- E Andrea Nelson, professor of wound healing, director of research3
- on behalf of the VenUS III Team
- 1Department of Health Sciences, University of York, UK
- 2Kleijnen Systematic Reviews, Escrick, York, UK
- 3School of Healthcare, University of Leeds, Leeds LS2 9JT, UK
- Correspondence to: E A Nelson e.a.nelson{at}leeds.ac.uk
- Accepted 6 January 2011
Abstract
Objective To assess the clinical effectiveness of weekly delivery of low dose, high frequency therapeutic ultrasound in conjunction with standard care for hard to heal venous leg ulcers.
Design Multicentre, pragmatic, two arm randomised controlled trial.
Setting Community and district nurse led services, community leg ulcer clinics, and hospital outpatient leg ulcer clinics in 12 urban and rural settings (11 in the United Kingdom and one in the Republic of Ireland).
Participants 337 patients with at least one venous leg ulcer of >6 months’ duration or >5 cm2 area and an ankle brachial pressure index of ≥0.8.
Interventions Weekly administration of low dose, high frequency ultrasound therapy (0.5 W/cm2, 1 MHz, pulsed pattern of 1:4) for up to 12 weeks plus standard care compared with standard care alone.
Main outcome measures Primary outcome was time to healing of the largest eligible leg ulcer. Secondary outcomes were proportion of patients healed by 12 months, percentage and absolute change in ulcer size, proportion of time participants were ulcer-free, health related quality of life, and adverse events.
Results The two groups showed no significant difference in the time to healing of the reference leg ulcer (log rank test, P=0.61). After adjustment for baseline ulcer area, baseline ulcer duration, use of compression bandaging, and study centre, there was still no evidence of a difference in time to healing (hazard ratio 0.99 (95% confidence interval 0.70 to 1.40), P=0.97). The median time to healing of the reference leg ulcer was inestimable. There was no significant difference between groups in the proportion of participants with all ulcers healed by 12 months (72/168 in ultrasound group v 78/169 in standard care group, P=0.39 for Fisher’s exact test) nor in the change in ulcer size at four weeks by treatment group (model estimate 0.05 (95% CI –0.09 to 0.19)). There was no difference in time to complete healing of all ulcers (log rank test, P=0.61), with median time to healing of 328 days (95% CI 235 to inestimable) with standard care and 365 days (224 days to inestimable) with ultrasound. There was no evidence of a difference in rates of recurrence of healed ulcers (17/31 with ultrasound v 14/31 with standard care, P=0.68 for Fisher’s exact test). There was no difference between the two groups in health related quality of life, both for the physical component score (model estimate 0.69 (–1.79 to 3.08)) and the mental component score (model estimate –0.93 (–3.30 to 1.44)), but there were significantly more adverse events in the ultrasound group (model estimate 0.30 (0.01 to 0.60)). There was a significant relation between time to ulcer healing and baseline ulcer area (hazard ratio 0.64 (0.55 to 0.75)) and baseline ulcer duration (hazard ratio 0.59 (0.50 to 0.71)), with larger and older ulcers taking longer to heal. In addition, those centres with high recruitment rates had the highest healing rates.
Conclusions Low dose, high frequency ultrasound administered weekly for 12 weeks during dressing changes in addition to standard care did not increase ulcer healing rates, affect quality of life, or reduce ulcer recurrence.
Trial registration ISRCTN21175670 and National Research Register N0484162339
Introduction
Leg ulceration is a chronic, recurring condition that affects 1.5–1.8% of adults in industrialised countries1 (with venous leg ulcers representing up to 84% of leg ulcers2) and has a considerable impact on health and quality of life.2 3 High compression bandaging is effective treatment,4 healing most new venous leg ulcers (<6 months’ duration) within a year.5 The priority is now to increase healing in ulcers with poorer prognostic profiles (bigger and older ulcers).
Ultrasound therapy is a standard treatment option for soft tissue injuries in physiotherapy clinics, and it is used in some centres for the management of chronic wounds6 and is recommended in some clinical practice guidelines.7 8 9 It is thought that using low intensity ultrasound (≤3 W/cm2) can be used to stimulate normal physiological responses to injury to aid repair.10 Other ultrasound regimens, delivered in a water bath, have been used with the primary aim of debriding wounds.11
A systematic review of trials of ultrasound therapy for treating venous leg ulcers suggested that it improved healing.12 Meta-analysis of the four trials that reported data on complete ulcer healing at 8–12 weeks produced a relative risk for healing of 1.44 (95% confidence interval 1.01 to 2.05). However, the trials identified were methodologically weak, heterogeneous, prone to bias, and varied widely in application regimens.
To investigate this further, we conducted a randomised controlled trial to compare the effect of standard ulcer care alone with standard care plus ultrasound treatment. We measured time to healing of the reference ulcer, health related quality of life, proportion of participants with ulcers healed at 12 months, percentage and absolute change in ulcer size, adverse events, and cost of treatments. The economic evaluation is reported separately.13
Methods
Ultrasound treatment
The dose at which ultrasound is delivered is related to its frequency (hertz), power (watts), pulsed or continuous cycle, and the duration of the treatment, which can produce many possible combinations.14 Therapeutic ultrasound has a frequency of 0.75–3.0 megahertz (MHz), and most machines used to deliver it are set at a frequency (that is, cycles per second) of either 1 or 3 MHz.15 The total amount of energy in an ultrasound beam is expressed in watts (W) indicating its power.15
At the time our study was designed, most evidence was available for ultrasound treatment at a frequency of 1 MHz and dose of 0.5 W/cm² (including the one study in the systematic review with only moderate risk of bias). Previous trials had evaluated ultrasound administered weekly, two or three times a week, or with declining frequency of administration. Administering ultrasound requires bandage removal, and hence our choice of treatment regimen balanced the costs of these visits against the potential reduction in healing time (if ultrasound were effective). We therefore chose a low dose, high frequency ultrasound treatment (1 MHz at 0.5 W/cm2) with a pulse pattern set at 1:4 and the duration of each treatment being determined by ulcer area. Treatment was delivered once weekly for up to 12 weeks.
Participants and setting
This was a pragmatic, multicentre, two arm, randomised controlled, open trial with equal randomisation carried out in 11 centres in the United Kingdom and one in the Republic of Ireland. Participants were recruited between March 2006 and December 2008 (end of extended recruitment period) from services led by community and district nurses, community leg ulcer clinics, and hospital outpatient leg ulcer clinics in urban and rural settings. Centres were recruited through staff from our known community of leg ulcer services and clinics. All venous leg ulcer patients on the treatment lists within these centres were assessed for trial inclusion by completion of a screening form by either their usual nursing team or a study research nurse. Systematic methods were used to approach and potentially recruit participants.
Nurse training
Before the trial started, participating nurses attended a training day in their centre which covered the rationale for the study, patient eligibility, recruitment and consent procedures, data collection, adverse event reporting, and the ultrasound application technique according to the manufacturer’s instructions and clinical expertise. Competency in ultrasound application was assessed at the end of the training. Trained nurses were permitted to train other local nurses to allow treatments to be maintained during staff absences. Continual support was available from the trial coordinator. Treatment fidelity checks were not undertaken.
This model of training reflected the likely investment in training that would be available in the National Health Service if the intervention proved successful and was rolled out to community nursing services and hospital outpatients. To maintain the pragmatic nature of the trial, we did not impose a regimen of observation of practice greater than there would be in standard care.
Patient eligibility
Eligible participants had venous leg ulcers of >6 months’ duration or >5 cm2 in size, or both. A participant was considered to have a venous leg ulcer if there was no other evident cause and clinical assessment suggested it was venous (moist, shallow, irregular shape, venous eczema, ankle oedema, lipodermatosclerosis, not confined to the foot) and participants had had an ankle brachial pressure index of ≥0.8 within the past three months. If participants had more than one ulcer, the largest eligible ulcer was defined as the reference ulcer, which would be followed throughout the study and, if allocated, receive the ultrasound therapy.
We originally planned to recruit only those able to tolerate high compression bandages. However, clinical collaborators argued that those who can tolerate only reduced compression therapy represent a particular challenge to treat and might benefit in particular from any effect of therapeutic ultrasound. We therefore removed the inclusion criterion of “willing and able to wear four-layer high compression bandaging.”
Participants were excluded if their leg ulcer was due to other causes, they were of childbearing age, were allergic to ultrasound contact gel, had poorly controlled diabetes (HbA1c >10% measured within the past three months), or had any of the known contraindications to ultrasound (including ankle or knee prosthesis or metal in the lower leg, suspected thrombophlebitis, active cellulitis, and suspected or confirmed local cancer or metastatic disease). The original protocol also stated the study would not recruit people with rheumatoid arthritis, peripheral arterial disease, or diabetes. However, after discussions with clinical collaborators, the first two criteria were removed as unnecessary, and the last was replaced by “poorly controlled diabetes.”
Ethical approval was gained for all changes. Participants gave written, informed consent.
Patient randomisation
Those patients deemed potentially eligible according to the screening form were seen by one of the trained nurses, who explained the study, confirmed eligibility, and obtained written consent. Consenting patients were randomised to receive ultrasound plus standard care or standard care alone. Randomisation was performed by the nurses telephoning an independent, secure, remote, randomisation service (York Trials Unit) thereby concealing treatment allocation. Randomisation was carried out by permuted block design with varying block sizes of four and six. Because of the nature of the intervention, it was not possible to blind either the patient or the nurse to the treatment.
Intervention
The ultrasound therapy was applied with a SoLo Therasonic 355 machine (EMS Physio, Wantage, UK). Before use, all the trial machines were tested by the National Physical Laboratory (Teddington, UK). Measurements were made of total acoustic power and effective radiating area, and these were within the tolerance of ±20% specified by IEC 60601-2-5 and IEC 61689. The machines were serviced regularly throughout the trial.
Treatment was given weekly at the patients’ regular dressing changes. After removal of all dressings and bandaging, the wound was cleaned as usual. The ultrasound transducer head was sterilised with alcohol wipes. Ultrasound was then applied to the skin surrounding the reference ulcer, using a water based contact gel recommended by the manufacturer, for 5–10 minutes by moving the transducer head in a slow, controlled manner around the edges of the ulcer in overlapping circles to cover the skin evenly. Ulcers of area <5 cm2 received ultrasound for five minutes, those of ≥10 cm2 received 10 minutes’ ultrasound. For ulcers between 5 cm2 and 10 cm2, treatment time in minutes equalled the ulcer area in cm² (ulcer of 6 cm2 area = 6 minutes’ treatment). After treatment, all traces of the contact gel were removed and the transducer head was cleaned with alcohol wipes. After the 12 weeks of ultrasound, participants returned to standard care alone.
Treatment before study enrolment was not formally recorded, but standard care comprised low adherent dressings and four-layer bandaging that was high compression, reduced compression, or no compression, depending on the patient’s tolerance, replaced at each weekly visit. Changes to this regimen, as deemed appropriate by the treating clinician, were recorded. Since standard care also reflected treatment as usual according to local practice, it could vary between centres.
Outcome measurement
The primary outcome was time to complete healing of the reference ulcer. Ulcer healing was defined as full epithelial cover without scab. Digital photographs of the reference ulcer were taken every four weeks, at point of healing, and seven days after healing by the treating nurse. Photographs were assessed by two remote, independent assessors who were blind to treatment allocation to determine the date of healing and to protect the study against assessment biases. Any discrepancies were referred to a third assessor. The primary outcome was calculated using the date of healing as decided by the blinded assessors. However, if no photographs were available for a patient, then the date of healing decided by the treating nurse was taken as the healed date.
Secondary outcomes (not all reported here but in our economic evaluation13) included the proportion of patients with ulcers healed at three, six, and 12 months, proportion of time ulcer-free, change in ulcer area, recurrence rates, health related quality of life, and adverse events. Ulcer area was calculated every four weeks (before ultrasound delivery) by the nurse tracing the perimeter on an acetate grid with a fine-nibbed pen, following a standard method that is accurate and reliable.16 As leg ulcer care is most commonly delivered in the home, it was not feasible to have a nurse blinded to the treatment attend dressing changes to trace the ulcer. Tracing data were measured using a computer package (Mouseyes).17
Patients’ perceptions of health outcome were assessed with the short form 12 (SF-12), which is sensitive to changes in venous ulcer healing status.18 Questionnaires were administered by post at three, six, nine, and 12 months.
Serious adverse events were defined as death, life threatening risk, hospitalisation, persistent or substantial disability or incapacity, and other medically important conditions (such as being newly diagnosed with diabetes). Other adverse events were classed as non-serious. Reporting nurses indicated whether, in their opinion, the event was related to the trial treatment. A list of possible treatment related adverse events was established a priori, based on the literature and the VenUS I and II trials5 19 (including pressure damage, infection, new ulcer, and ulcer deterioration).
Statistical analysis
All analyses were done in SAS version 9.1 and STATA version 10 on an intention to treat basis with a two sided 5% significance level. Scoring of the SF-12 questionnaire’s health related quality of life was done with the QualityMetric Health Outcomes Scoring Software 2.
Allowing for 10% attrition, we estimated that a total of 336 participants would provide 90% power to detect a reduction in the median time to healing from 22 weeks to 15 weeks. The control healing time was based on trial data for large or chronic ulcers: 13–37% of people with chronic and large ulcers heal at 24 weeks with high compression.20 Our target population included people with chronic or large ulcers, and from previous trials,5 we estimated that about 50% of ulcers in the standard care group would heal within 22 weeks. As ultrasound increases treatment time and is not currently used by community nurses, we anticipated that clinicians would require a moderate effect size for them to adopt this technology; hence a reduction in healing time from 22 to 15 weeks was deemed clinically meaningful. The minimum clinically important effect size is related to the ease of delivery of the intervention, its acceptability, and costs, both in initiation and ongoing delivery.
Our primary analysis compared time to complete healing of the reference ulcer between the two randomised groups using a Cox regression model.21 Shared centre frailty (random) effects were assumed to follow a γ distribution, and STATA was used to fit a Cox survival regression model. The analysis adjusted for centre as a random effect, ulcer area (from baseline tracing), ulcer duration, and whether the patient was treated with high compression bandaging (as fixed effects). These factors were chosen because they had been prognostic in other leg ulcer studies.5 19 The distribution of baseline ulcer area and baseline ulcer duration were highly skewed, so we used the logarithm of baseline ulcer area and ulcer duration in the subsequent analysis. Patients who withdrew from the study or whose reference ulcer had not healed by trial conclusion were treated as censored. If centres recruited five or fewer patients we repeated the analysis with no adjustment for centre as a sensitivity analysis.
The assumption of proportional hazards was checked by using log-log plots, by including interaction terms in the model (for each term with time), and by looking at plots of Schoenfeld residuals. Kaplan-Meier survival curves describing time to healing were produced for the two groups and the median time to healing with 95% confidence interval.
Cohen’s κ measure of inter-rater agreement was used to assess agreement between the two assessors of the photographs for healing. This was repeated to look at agreement between the final decision from the photograph assessment and the nurses’ date of healing. Ulcer area at week 4 was compared between treatment groups using analysis of covariance to adjust for baseline ulcer area, centre, ulcer duration, and use of compression bandaging.
We analysed the scores for the physical and mental health components of the SF-12 questionnaire using a multi-level regression model. The outcomes at each time point were used in a single model, with time points nested within participants to account for within-patient correlation in scores. The model was used to estimate the difference between treatments over the whole 12 month follow-up. The outcome modelled was the score at each follow-up assessment, and the covariates included in the model were centre, baseline ulcer area, ulcer duration, use of compression, and time (indicators for 0, 3, 6, 9 and 12 months). We assessed whether the pattern in quality of life scores over time was different between the two treatments by including an interaction term between treatment and time in the model.
We assessed the assumption of normally distributed data and, if necessary, used log transformations or other analysis methods.
We used a negative binomial model22 adjusting for the same covariates as the primary analyses, to compare the average number of adverse events experienced by each patient in the two treatment groups. Separate analyses were performed for serious and non-serious adverse events.
Results
Between January 2006 and December 2008, 1488 people with leg ulcers were screened across 12 centres, and 337 (22.6%) were randomised: 168 to ultrasound plus standard care and 169 to standard care. Figure 1⇓ shows the flow of participants through the trial, and table 1⇓ summarises their baseline characteristics.

{kind=link}
Baseline characteristics of 337 patients with venous leg ulcers who were randomised to standard care alone or to ultrasound plus standard care. Values are numbers (percentages) unless stated otherwise
Table 2⇓ gives details of the compression bandaging provided, for both groups, and the ultrasound treatment for the intervention group. Participants in the ultrasound group had a median of 11 ultrasound treatments during the 12 week ultrasound period (mean 10.25).
Treatment details for 337 patients with venous leg ulcers who were randomised to standard care alone or to ultrasound plus standard care
Primary outcomes
We found no evidence of a difference in time to healing between the two treatment groups with either the log rank test (log rank test statistic 0.25, P=0.61) or Wilcoxon’s rank sum test (Wilcoxon test statistic 0.33, P=0.56). Figure 2⇓ shows the Kaplan-Meier survival curve for time to healing of reference ulcers in both groups.

Fig 2 Kaplan-Meier survival curve for time to healing of reference ulcers among 337 patients with venous leg ulcers randomised to standard care alone or to ultrasound plus standard care
{kind=link}
For the Cox model, the proportional hazard assumption was tested and was not violated, either separately for each covariate (ultrasound v standard care (P=0.7230), log(area) (P=0.1467), log(duration) (P=0.2938), high compression (P=0.2030)) or globally (P=0.3548)). Hence, all hazard ratios were assumed constant during the follow-up period. From the Cox proportional hazards model, after adjustment for baseline ulcer area, baseline ulcer duration, use of compression bandaging, and study centre (as a random effect), there was still no evidence of a difference in time to healing between the two treatment groups (hazard ratio 0.99 (95% confidence interval 0.70 to 1.40), P=0.97). There was, however, significant heterogeneity in the healing rates among centres (P=0.0001) not explained by the covariates included in the model. We found that centres recruiting more participants were associated with higher healing rates than centres recruiting fewer participants.
The median time to complete healing of all ulcers in the standard care group was 328 days (95% confidence interval 235 days to inestimable) and in the ultrasound group was 365 days (224 days to inestimable). Figure 3⇓ shows the Kaplan-Meier survival curve for time to complete healing of all ulcers in both groups.
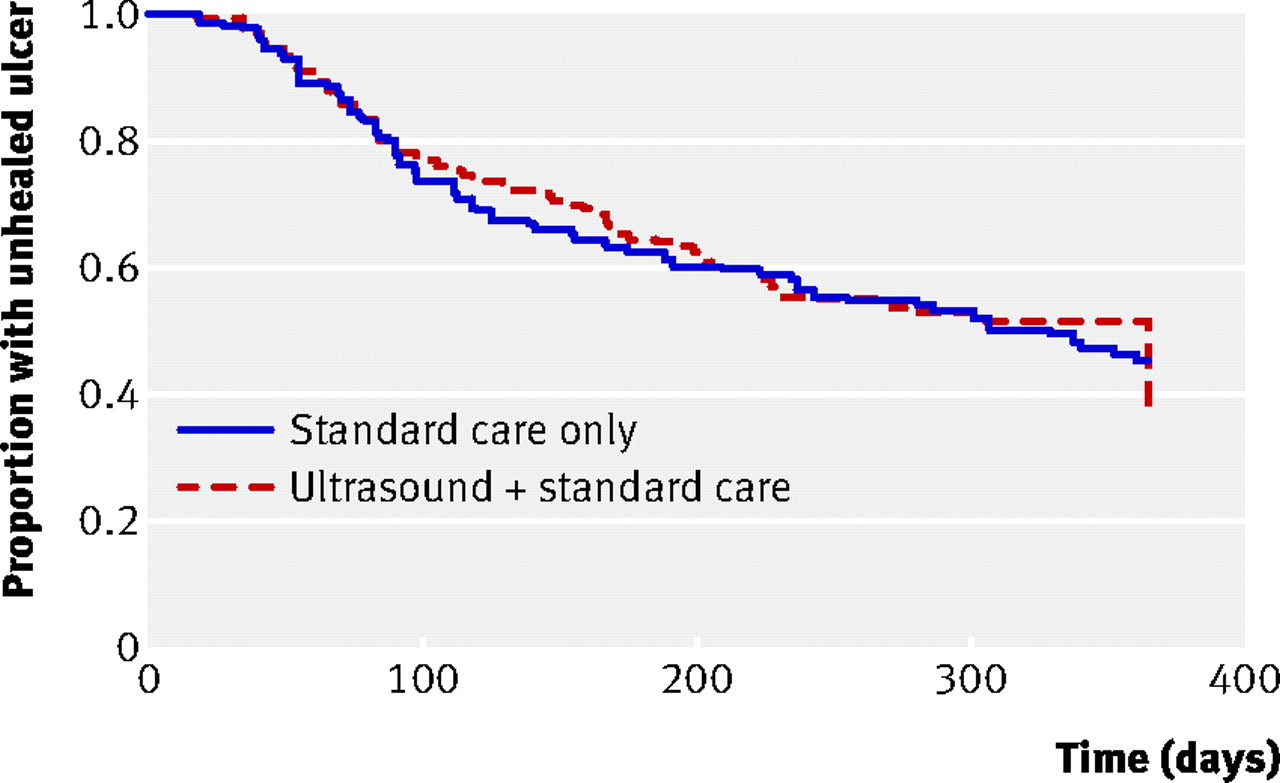
Fig 3 Kaplan-Meier survival curve for time to complete healing of all ulcers among 337 patients with venous leg ulcers randomised to standard care alone or to ultrasound plus standard care
{kind=link}
Secondary outcomes
There was no significant difference between the two groups in the proportion of participants with all ulcers healed (according to the nurse forms) by 12 months (72/168 in ultrasound group v 78/169 in standard care group, P=0.3854 for Fisher’s exact test). For comparison with other studies, there was no difference in the proportions of reference ulcers healed (according to blinded assessment of photographs) at three months (28/168 v 30/169 standard care, P=0.8854) or at six months (48/168 v 52/169, P=0.7208).
We used Cohen’s κ measure to assess the agreement between the two blinded assessors of the ulcer photographs and whether the assessors agreed with the unblinded nurse as to whether the reference ulcer had healed. The photograph assessors’ measure of agreement was estimated as 0.84 (95% confidence interval 0.78 to 0.90), and agreement between the assessors and the nurse was 0.76 (0.69 to 0.83).
Of the 133 participants with photographically confirmed healing of their reference ulcer, 124 were successfully contacted later to ascertain whether their ulcer had recurred. The remaining participants were not contacted for various reasons (including invalid or changed telephone number, telephone not answered, and patient moved). Overall, the reference ulcer had recurred in 31 (25%) of the 124 participants (14 (45%) from the standard care group, 17 (55%) from the ultrasound group). There was no significant difference in the recurrence rates between the two groups (P=0.68 for Fisher’s exact test).
We analysed ulcer area after four weeks of treatment to determine whether ultrasound affected rate of healing (baseline ulcer area was included in the model as a covariate). There was a non-significant ultrasound treatment effect (model estimate 0.05 (95% CI –0.09 to 0.19), P=0.50) and a non-significant ulcer compression effect (model estimate 0.02 (–0.19 to 0.24), P=0.84). Baseline ulcer area and duration both had significant effects on the initial change in ulcer area (model estimates 0.77 (0.72 to 0.84) and 0.13 (0.07 to 0.19) respectively, both P=0.0001): smaller and newer ulcers reduced in area more quickly. There was no evidence of any difference between centres (model estimate 0.01, P=0.15).
At baseline, the mean physical component summary score of the SF-12 questionnaire was 36.55 (SD 11.32) for the ultrasound group and 35.33 (11.47) for the standard care group (compared with a score of 43.93 (9.29) for people aged 65–74 years in the general US population), and the mean mental component summary score was 46.72 (11.52) for the ultrasound group and 47.11 (11.29) for the standard care group (compared with 51.57 (8.36) for the general US population). Response rates for the SF-12 questionnaires were 89%, 84%, 81%, and 86% at three, six, nine, and 12 months respectively. Figures 4⇓ and 5⇓ show little change in the physical and mental component scores over time: hence there was a constant linear trend of both scores against time. There was no evidence of a difference between the two treatment groups in the mean physical component summary scores (model estimate 0.69 (–1.79 to 3.08), P=0.58) or the mean mental component summary scores (model estimate –0.93 (–3.30 to 1.44), P=0.44).

Fig 4 Mean physical component summary score of the short form 12 (SF-12) questionnaire among 337 patients with venous leg ulcers randomised to standard care alone or to ultrasound plus standard care
{kind=link}

Fig 5 Mean mental component summary score of the short form 12 (SF-12) questionnaire among 337 patients with venous leg ulcers randomised to standard care alone or to ultrasound plus standard care
{kind=link}
There were 88 serious adverse events in 64 participants: 29 participants (45%) in the standard care group and 35 (55%) in the ultrasound group. There were 445 non-serious adverse events in 153 participants: 67 (44%) were in the standard care group and 86 (56%) in the ultrasound group. When we set the model response as the number of serious adverse events per patient throughout follow-up, we found no significant difference in adverse events due to treatment received (model estimate 0.23 (–0.34 to 0.79), P=0.39) or baseline use of compression bandaging (model estimate –0.16 (–0.98 to 0.65), P=0.66). There was weak evidence that larger baseline ulcer area and longer baseline ulcer duration were associated with more serious adverse events (model estimates 0.19 (–0.03 to 0.40), P=0.08, and 0.22 (–0.02 to 0.45), P=0.06, respectively).
The number of non-serious adverse events was significantly associated with the treatment received, with more events in the ultrasound group than the standard care group (model estimate 0.35 (0.02 to 0.67), P=0.04) but was not related to baseline ulcer area (model estimate 0.05 (–0.08 to 0.17), P=0.42), baseline ulcer duration (model estimate 0.08 (–0.06 to 0.22), P=0.24), and baseline compression use (model estimate −0.003 (–0.46 to 0.47), P=0.99).
Discussion
We found no evidence that therapeutic low dose, high hertz frequency ultrasound delivered once a week improves the healing of venous leg ulcers. We did observe a significant centre effect, such that rates of ulcer healing differed significantly between treatment centres. A centre’s healing rate was proportional to the number of participants. There was no evidence of ultrasound having an effect on healing when analysed by centre. As there was little change in the SF-12 questionnaire’s physical component summary score during the trial in either group and no evidence of a significant change in the mental component summary score over time, ultrasound showed no impact on health related quality of life.
Bandaging use was recorded 6473 times for the people treated with standard care and 8013 times for the people treated with ultrasound. Were the level of compression of bandages to differ significantly between the two groups, then this might introduce a performance bias. The proportion of visits at which high compression systems (four layer, three layer, or two layer) was used was 67% (5397/8013) for ultrasound and 72% (4641/6473) for standard care. The proportion of visits at which no compression was used was 3.4% (220/6473) in standard care and 5.7% (455/8013) in the ultrasound group. The modest differences in the level of compression used (fewer in the standard care group had no compression) were not significant, and hence performance bias is unlikely to account for the lack of evidence of benefit with ultrasound.
Although there were more adverse events in the ultrasound group than the standard care group, as ultrasound is not currently used in practice, it is possible that nurses were more likely to attribute adverse events (such as ulcer deterioration) to a treatment with which they are relatively unfamiliar. The overall adverse event rate (the number of people reporting any adverse event) was similar to that in the VenUS I trial,5 which reported an event rate of about 40%.
Strengths and limitations of study
The strengths of this study include the large sample size, wide inclusion criteria, blinded allocation, use of best available standard treatment, blinded outcome assessment, low loss to follow-up, collection of quality of life and effectiveness data, and long duration of follow-up. Limitations included the modest response rate from patients at 12 months in respect of the quality of life questionnaires.
In addition, there is the possibility of random error in the evaluation of the ulcer area when traced using the computer software.17 However, the ulcers were measured every four weeks for the purpose of dose adjustment, and, although this was done by the unblinded nurse, there is no reason for systematic errors (bias) being introduced as the primary outcome measure was time to complete healing as assessed by a blinded assessor. Any doubts regarding the potential errors in ulcer measurements confirm the importance of the more robust outcome measure of time to healing with the addition of a blinded outcome assessment to confirm this.
Rationale for this study
Reviews of earlier trial evidence for the effects of ultrasound in wound healing generally23 and leg ulcers specifically12 identified the potential benefit of ultrasound therapy for venous ulcer healing. However, a definitive study was needed since these trials were small, had methodological weaknesses, and had incomplete reporting and were at high risk of bias. Furthermore, the clinical contexts in which the trials had taken place (such as before the widespread introduction of high compression therapy) meant that their relevance to today’s leg ulcer management was uncertain. Since completion of our study, an updated systematic review has been published with eight trials included, six using high frequency ultrasound and two using low frequency ultrasound.24
We now know from prognostic studies and trials that high compression therapy heals some 80% of venous ulcers within 12 months and that ulcers smaller than 5 cm2 and of less than six months’ duration are likely to heal quickly.20 In designing this trial, we therefore felt that adding an adjuvant ultrasound therapy to the treatment of small or new ulcers was unwarranted. The sample size of a trial to find a benefit of adding ultrasound to the treatment of most venous ulcers would have to be very large given the high healing rate. We therefore recruited people with hard to heal ulcers—those for whom clinicians might consider additional interventions beyond standard care. On the whole, participants’ ulcers were large (12 cm2) and chronic (1 year duration), and those recruited were representative of the venous ulcer population in terms of age and sex.1
There are two explanations for our findings: firstly, that there is a treatment effect but our trial failed to detect it (due to chance or to methodological problems), or, secondly, ultrasound therapy at the dose and frequency used does not accelerate healing of hard to heal venous ulcers. We minimised the play of chance by having a large sample size. We minimised detection bias by using confirmed healing date by photographic assessment. The possibility that ultrasound machines did not deliver the prescribed dose was reduced by having them serviced and calibrated regularly, and we recorded all treatments given to ascertain if there was evidence of performance bias (such as extra treatments in the standard care group), which there was not.
Our decision to use low dose, high frequency ultrasound therapy (0.5 W/cm2, 1 MHz, pulsed pattern of 1:4) administered weekly was based on earlier evidence (the largest trial) and the need to balance the delivery of leg ulcer care in an efficient manner, with weekly visits to renew dressings and bandages, against the desire to deliver ultrasound more frequently. We stopped delivering ultrasound at 12 weeks as we felt this was a pragmatic approach to evaluating the addition of a novel therapy that took account of the extra treatment time required by the nurse. We felt that asking nurses to apply ultrasound for the whole trial period would have resulted in disillusionment if nurses felt that there was no discernable benefit, as this would increase the workload significantly: this would have hampered recruitment. The lack of any treatment effect, as seen in the Kaplan-Meier curves, seems consistent with there being no effect on healing rate within the first 12 weeks. Given the widely accepted use of compression therapy, replaced usually once or twice a week, it would be impractical to deliver ultrasound other than at the regular bandage renewal; hence our rationale for weekly ultrasound to integrate with current practice.
Implications of results
Here we report the largest trial undertaken of therapeutic ultrasound for wound healing.23 24 25 This trial is also much larger than any trial of ultrasound for fractures included in a recent systematic review26 and was conducted and reported in accordance with international guidelines for research excellence.27 28
We designed this trial in 2003, when there were seven trials summarised in a systematic review,12 two of which were not randomised. If we now add the VenUS III data into that meta-analysis (by taking our numbers of ulcers healed at 12 weeks), we find that, although more ulcers healed with ultrasound than with sham ultrasound or standard care, the difference was not statistically significant (P=0.095). Furthermore, VenUS III is the only trial to meet all the validity criteria of adequate randomisation, full allocation concealment, blinded outcome assessment, and analysis based on intention to treat, so we would argue that the VenUS III result is the most valid. The conclusion we therefore draw from all the evidence is that therapeutic ultrasound does not confer any benefit on the healing of hard to heal venous leg ulcers (that is, >5 cm2 in area or >6 months old, or both).
However, we evaluated only one ultrasound regimen, and so our results cannot be extrapolated to other regimens, such as those delivering ultrasound via a water bath to debride wounds. We identified a large variation in healing rates according to trial centres, with those centres recruiting more participants to the trial having higher healing rates overall. This centre effect may be a manifestation of a relation between the volume of throughput and the quality of care. This finding is worthy of further exploration. Other research questions include the evaluation of the effectiveness of this and alternative ultrasound regimens, say through value of information approaches.
Implications for clinicians are that there is no evidence to support the addition of ultrasound therapy to treatments for people with hard to heal leg ulcers.
What is already known on this topic?
Most venous leg ulcers heal in 6–12 months, but those with a duration of >6 months or that are larger than average are harder to heal
Clinical trials have suggested that therapeutic ultrasound can help heal leg ulcers, but these studies were methodologically weak, small in size, varied widely in application regimens, included people with small, new ulcers, which heal relatively quickly, or did not use optimal existing treatments
What this study adds
There is no evidence of a benefit in terms of time to ulcer healing, probability of ulcer having healed at 12 months, rate of reduction in ulcer area, or health related quality of life for people with hard to heal ulcers treated with weekly administration of low dose, high frequency, adjuvant ultrasound therapy (0.5 W/cm2, 1 MHz, pulsed pattern of 1:4) for up to 12 weeks
Notes
Cite this as: BMJ 2011;342:d1092
Footnotes
We thank the patients who took part in this trial; the research nurses, tissue viability teams, district nurses, and hospital outpatient staff who recruited patients and completed the trial documentation; principal investigators at each site; members of the trial steering committee (S Homer-Vanniasinkam (chair 2006), Su Mason (member 2006, then chair 2007–8), Kevin Burnand, Denise Howell, Timothy Rowlands, Nikki Stubbs); and members of the data monitoring and ethics committee (Robin Prescott (chair), Andrew Bradbury, Brenda King) who oversaw the study. We also thank Bernie Boyle, Susan Bradley, Melanie Burrows, Margaret Crookes, Joanne Dakin, Patricia Davies, Erica Denton, Mary Doherty, Sarah Fiori, Gemma Hancock, June Jones, Peter Jones, Denise Nightingale, Lesley Marland, Jeanette Marshall, Jane Mayes, Jane Megson, Sue Merryweather, Carol Muir, Pam Ross, Rebecca Stubbs, Debra Vickery, Victoria Warner, Shirley Williams, and Lindsey Worstenholme for recruiting participants into the study; Una Adderley, Gemma Hancock, and Susan O’Meara, who undertook the blinded outcomes assessment of ulcer photographs; and Mei-See Man, who carried out the ulcer tracing measurements.
The VenUS III collaborators (current and past) are Una Adderley, Paul Allcoat, Jacqui Ashton, JMB, Annemarie Brown, Sue Collins, L-HC, Ben Cross, NC, Carol Dealey, Jo Dumville, Kate Flemming, Liz Holey, CI, ARK, Linda McDermott-Scales, Janet McGowan, EAN, Angie Oswald, Sarah Pankhurst, Stephen Pye, Elizabeth McGinnis, MOS, Gerben ter Riet, DT, Kath Vowden, Peter Vowden, Michael Walker, Shernaz Walton, Val Wadsworth, JMW, GW, and Anne Witherow.
Contributors: EAN was the chief investigator, chaired the trial management group, and edited and approved the final draft of the paper. JMW was the trial coordinator and drafted the paper. GW and JMB designed the clinical analysis. JMB oversaw the conduct of the analysis. ARK conducted the clinical analysis. MOS contributed to the trial management group, designed the economic analyses, and oversaw the conduct of the analysis. L-HC undertook the economic analysis. CI participated in the design and conduct of the study. NC and DT contributed to the study design and coordination and commented on drafts of the paper. EAN is the guarantor of the paper.
Funding: This project was funded by the UK National Institute for Health Research (NIHR) Health Technology Assessment Programme (project No 02/37/03), and it will be published in full in the journal Health Technology Assessment. The NIHR had no role in the data collection, statistical analysis, or writing of this article or the decision to submit for publication. The views and opinions expressed herein are those of the authors and do not necessarily reflect those of the Department of Health. EMS Physio supplied the SoLo Therasonic 355 ultrasound machines at a discounted price, but had no role in the design of the trial or in the collection, analysis, and interpretation of the data.
Competing interests: All authors have completed the Unified Competing Interest form at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare: JW, AK, L-HC and EAN all received proportions of their salaries from this grant in order to conduct the study. All other authors declare no support from any organisation for the submitted work.
Ethical approval: The study was approved by York Multicentre Research Ethics Committee (MREC), local research ethics committees, and research and development departments.
Data sharing: No additional data available
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.