Preventing malaria in travellers
BMJ 2008; 336 doi: https://doi.org/10.1136/bmj.a153 (Published 12 June 2008) Cite this as: BMJ 2008;336:1362
- 1Liverpool School of Tropical Medicine, Liverpool L3 5QA
- 2National Travel Health Network and Centre, London WC1E 6AU
- 3London School of Hygiene and Tropical Medicine, London WC1E 7HT
- Correspondence to: D G Lalloo dlalloo{at}liverpool.ac.uk
Summary points
Malaria can be prevented by avoiding bites and using appropriate chemoprophylaxis
An individual harm-benefit assessment should be made for each traveller
The possibility of malaria should be kept in mind for any traveller returning from an endemic area
Protecting travellers against malaria is increasingly important as the number travelling overseas continues to rise, with a disproportionate increase in visits to tropical areas where malaria transmission may occur. Each year about 1700 cases of malaria occur in the United Kingdom, 1300 in the United States, and 3000 in France.1 2 3 In the UK, about 75% of these cases are caused by Plasmodium falciparum, which produces the most severe form of malaria; five to 16 deaths occur annually and are nearly always in cases of falciparum malaria.1
Most infections occur in travellers resident in the UK, rather than in visitors to the UK. Malaria is a major risk for travellers if they do not take chemoprophylaxis or if they take incorrect prophylaxis.4 5 This review explores how to protect travellers from malaria. Most of the evidence base for malaria prophylaxis comes from small randomised controlled trials or observational studies.
Approach to preventing malaria
A useful approach is the “ABCD” of malaria prevention: Awareness of risk, Bite avoidance, Compliance with chemoprophylaxis, and the prompt Diagnosis of malaria (box 1)
Box 1 Harm-benefit assessment based on the “ABCD” approach to malaria prevention*
Assessment and awareness of malaria risk
Detailed geographical location of trip (name of country alone not adequate); time of year may also be relevant. See www.nathnac.org or www.cdc.gov/malaria/travel/index.htm
Duration of time in the area
Activities to be undertaken (relates to likelihood of exposure to infected mosquitoes—urban environment is generally less risky than rural environment)
Bite avoidance
Protective clothing
Repellents
Longlife insecticide-treated netting
Chemoprophylaxis
Is chemoprophylaxis indicated or would bite avoidance be sufficient?
Does the area have chloroquine resistant P falciparum?
Consider medical history and other medications
Consider previous experience with antimalarials
Are there contraindications to mefloquine (history of psychiatric problems or epilepsy)?
Take patient choice and resources into consideration when making decision
Diagnosis
Consider diagnosis of malaria in travellers returning from endemic area
Arrange prompt diagnostic tests (malaria slides or rapid diagnostic tests)
*Detailed templates available6
Who is at risk and how does one assess it?
Factors determining individual risk
A detailed itinerary is necessary to assess risk. The degree of transmission varies markedly between different regions, even within a country, and at different times of the year. For example, the risk of acquiring malaria in West Africa may reach 6% per month of travel but on the Kenyan coast is 1% per month; in the Kenyan capital, Nairobi, transmission is extremely low.
In addition to geographical factors, an individual’s risk depends on the time spent in the endemic area and activities undertaken: camping in a jungle for three weeks poses a much higher risk than a three day visit to an urban area with air conditioned accommodation.
Four main species of malaria parasites infect humans after the bite of an infected Anopheles spp mosquito: P falciparum, P vivax, P ovale and P malariae. P falciparum and P vivax are the most common. Falciparum malaria predominates in sub-Saharan Africa, and vivax malaria in the Indian subcontinent, Mexico, Central America, and China; both species occur in South East Asia and South America.
Groups at particular risk
Less than half of travellers who acquire malaria have taken advice before travelling. Analysis of imported malaria indicates that certain groups are at particular risk, such as those taking last minute holidays and those visiting friends and relatives abroad.7 Travellers visiting friends and relatives abroad (also known as VFR travellers) account for 70% of all of the malaria imported into the UK1; limited evidence suggests that these travellers do not think of malaria as a serious or potentially fatal disease, are less likely to consult general practitioners or travel medicine specialists, and often travel to areas of high risk such as West Africa.7 8 Using intervention strategies for travellers visiting friends and relatives—such as increasing awareness in the community, dispelling myths about immunity or subsidising antimalarials—could considerably reduce imported malaria.9
How can bites be prevented?
Avoiding mosquito bites is critical. This will also help to prevent other vector borne diseases such as yellow fever or dengue. The peak time for malaria mosquitoes to bite is from dusk to dawn; during these times, using repellents and covering up with clothing impregnated with permethrin will help to prevent bites.10 Evidence from trials is strong that sleeping under impregnated bednets reduces the risk of malaria in endemic populations, and this is likely to be equally effective in travellers.11 All travellers should be advised to carry longlife impregnated nets. Several repellents are effective (box 2). The chemical DEET has been most thoroughly studied and is simplest to use as it needs only infrequent reapplication.12 It is safe in children aged over 2 months and in pregnant women.6 13 Most “natural” repellents have a limited duration of activity, and several popular measures are ineffective (box 3).
Box 2 Effective repellents
DEET 20-50% gives 6-12 hours of protection (no advantage from concentrations higher than 50%)12
Picaridin 20% (relatively limited availability in the UK) has a similar duration of protection to 20% DEET
Lemon eucalyptus oil is effective, but needs frequent reapplications
Box 3 Popular but ineffective malaria prevention practices
Homoeopathic prophylaxis (deaths reported)
Yeast, garlic, marmite, vitamin B-1
Electronic mosquito repellents
Some natural repellents, such as oil of citronella (effective for only 30-60 minutes, and reapplication is needed too frequently for citronella to be recommended12)
How do antimalarials work?
All malarial parasites develop in the liver after injection of sporozoites by the mosquito. After a minimum period of seven days, merozoites emerge from the liver and infect red blood cells, causing clinical symptoms of malaria. Infection with P vivax and P ovale may cause persistent liver forms (hypnozoites) that re-emerge months after initial infection. Most antimalarial drugs kill parasites when they are in the red blood cells rather than in the liver.14
How to choose a drug regimen
The choice of an effective drug for prophylaxis depends on (a) individual factors, such as health problems or medications (and whether medical resources are available at the destination), length of stay, and previous experience with antimalarials; and (b) the region visited, which defines the predominant malaria species and drug sensitivity (box 4). The benefits and drawbacks of each medication, including cost, should be thoroughly discussed with the traveller (table⇓).
Box 4 Antimalarial regimens
All regions
Atovaquone plus proguanil (Malarone)
Doxycycline
Mefloquine
Regions with limited chloroquine resistance
Chloroquine plus proguanil
Regions with chloroquine sensitivity
Chloroquine
Characteristics of different antimalarial drugs
The five main antimalarial regimens are chloroquine alone, chloroquine plus proguanil, atovaquone plus proguanil (Malarone), doxycycline, and mefloquine. Resistance of P falciparum to chloroquine (and to a lesser extent to other antimalarials) is a global problem, and chloroquine now has limited effectiveness in most of the world.
Areas where P falciparum is resistant to chloroquine
Three main drug options exist for prevention in the areas where P falciparum is resistant to chloroquine: atovaquone plus proguanil, doxycycline, and mefloquine. Some countries (such as the UK) also advocate chloroquine plus proguanil for the limited areas of low level resistance, such as parts of India and Indonesia. Randomised controlled trials show that the three main options all have similar efficacy (close to 90%) against P falciparum.15 16 Mefloquine should not be used for the limited areas of multidrug resistance, such as the rural, forested areas where Thailand has borders with Cambodia and Burma.14
Travellers must continue prophylactic regimens (except atovaquone plus proguanil) for four weeks after leaving the risk area as the drugs work by killing parasites during their development in the red blood cells (suppressive prophylaxis). The combination of atovaquone plus proguanil prevents the development of liver forms (causal prophylaxis) and therefore needs to be taken only for a week after leaving the risk area, making it ideal for short trips. However, atovaquone/proguanil is considerably more expensive than the other prophylactic regimens. P vivax and P ovale may persist as hypnozoites in the liver, and therefore infection may re-emerge many months after return (relapse) despite compliance with chemoprophylaxis.16
Areas where malaria is sensitive to chloroquine
Only Mexico and parts of Central America (areas north and west of the Panama Canal), of the Caribbean (Haiti and the Dominican Republic), of the Middle East, of North Africa, and of China have malaria sensitive to chloroquine (figure⇓ ). Chloroquine or exceptionally proguanil may be used in these regions.
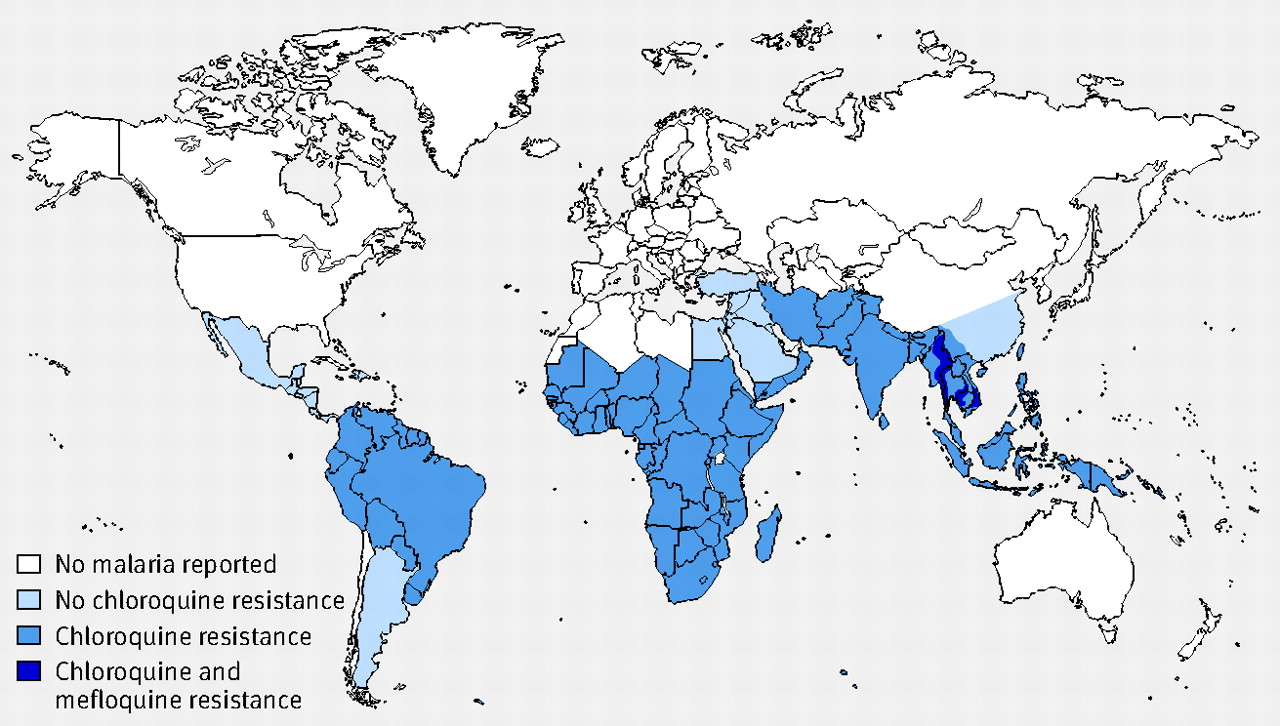
Malaria transmission and drug sensitivity across the world. Adapted from Canada Communicable Disease Report. Vol 30S1. Health Canada, 2004
{kind=link}
Adverse events
In randomised controlled trials of the tolerability of antimalarials, many patients report adverse events. However, the rate of adverse events is also high in placebo arms, making assessment of relation to the drug difficult.17 Discontinuation of prophylaxis is less than 5% for all drugs in most studies.17 18 Mild to moderate neuropsychiatric problems (headache or sleep disorder) are most common with mefloquine, particularly in women. The frequency of severe neuropsychiatric adverse reactions with mefloquine remains controversial, with best estimates of a frequency between 1 in 6000 to 1 in 20 000.19 Potential adverse events with mefloquine should be discussed with all travellers, and the drug should not be given to those with neuropsychiatric disorders. The table⇑ outlines the adverse events associated with each of the antimalarial agents.
Adherence
Adherence to chemoprophylaxis is a key component of success in preventing malaria. The occurrence of malaria in travellers who have returned home is almost always associated with the failure to take any chemoprophylaxis, taking incorrect chemoprophylaxis, or not complying with the drug regimen.1 Travellers should be made aware of the importance of completing the course of antimalarials.
Are there new developments on the horizon?
Other drugs
Primaquine has been used for treating hypnozoites of P vivax and P ovale for more than 50 years. Randomised controlled trials have also shown its efficacy as a “causal prophylactic” and in preventing establishment of hypnozoites.20 In the US, primaquine has recently been recommended as second line prophylaxis. However, it is contraindicated in those with glucose-6-phosphate dehydrogenase (G6PD) deficiency, and this enzyme must be checked before the drug is prescribed. Although not currently recommended in the UK, primaquine may be useful for short trips in travellers who have contraindications to other antimalarials.
Tafenoquine has similar properties to primaquine and has been shown to be effective in randomised controlled trials.21 It may be given in monthly or weekly doses and is well tolerated in individuals with a normal glucose-6-phosphate dehydrogenase level but is not yet licensed or released.
Malaria vaccine
A wholly protective vaccine for travellers will not be available in the near future. Considerable funding and research have led to a sporozoite based vaccine that has shown partial protection in African children. Nevertheless, awareness, bite prevention, and chemoprophylaxis will remain the mainstay of prevention for some time.
Are there alternative strategies to chemoprophylaxis?
Some countries, including Germany and Switzerland, recommend that when the risk of malaria is relatively low, travellers should not take chemoprophylaxis but should carry antimalarials, to be taken if they develop a fever (“standby” treatment).19 Although this approach has the advantage of avoiding potential adverse effects of chemoprophylaxis, observational evidence shows that standby antimalarials are often taken inappropriately.22 The availability of rapid self diagnosis malaria tests has not proved helpful either, as observational studies have shown that sick individuals often have difficulty performing the tests accurately.23 Current UK recommendations therefore do not support this approach.
What can be done for the “complex” traveller?
Pregnancy and breast feeding
Pregnant women have an increased risk of contracting malaria and of developing severe illness. If possible, they should be dissuaded from visiting risk areas. Extensive clinical experience shows that chloroquine and proguanil (with additional folate) are safe, but this combination has limited efficacy in areas where P falciparum is resistant to chloroquine. Doxycycline is contraindicated owing to its effects on skeletal development, and there are insufficient data (although no theoretical risk) for atovaquone plus proguanil. Some evidence supports the safety of mefloquine in the second and third trimesters, and it therefore remains the drug of choice for chloroquine resistance areas.6 24 Caution is needed with mefloquine in the first trimester because of limited data. DEET seems to be safe in pregnancy.13 Impregnated nets may be particularly useful for pregnant mothers.
Data are limited on the excretion of antimalarials in breast milk. Drugs that are contraindicated in pregnancy should not be taken if the mother is breast feeding. The amount of drug excreted in breast milk is insufficient to protect the infant, so separate medication is needed for the infant. Caution is needed with children at the lowest end of the weight band when both mother and child are taking mefloquine.
Children
Apart from doxycycline, all drugs can be used in children over 10 kg. Chloroquine plus proguanil can be used from birth, and mefloquine can be prescribed in those over 5 kg.6 Impregnated nets may be particularly useful for children.
Long term travellers
Long term travellers (those spending six months or more overseas) need a preventive strategy with a well tolerated regimen that will be followed consistently.25 Although few antimalarials are licensed for more than a year, this reflects a lack of controlled studies on long term use rather than evidence of harm. Knowing the epidemiological pattern of malaria and the degree of risk is also helpful in matching prevention to an individual. Continuous use of chloroquine for more than five years should be accompanied by ophthalmological screening.
What about when the traveller returns home?
Malaria prophylaxis is not 100% effective even with full adherence. All travellers and health professionals should consider the possibility of malaria if fever develops after travelling in a malaria endemic zone. Observational data show that most falciparum malaria will present within the first three months of return, but vivax malaria and ovale malaria can present much later. A malaria slide should always be obtained in a febrile patient who has visited a risk area, even if the symptoms suggest another cause.26
If a patient presents with an adverse reaction to an antimalarial after returning home, consider whether to switch antimalarials or discontinue them. Expert opinion suggests that in most circumstances, particularly if the patient is unwell, it is appropriate to stop prophylaxis and warn the patient that they have had inadequate prophylaxis and should therefore report fevers immediately.
Sources and selection criteria
We searched PubMed for relevant articles from 1966 to April 2007 using the key words “malaria”, “prevention”, “travellers”, “prophylaxis”, “adherence”, and individual drug names. We also searched the Cochrane Library for all malaria reviews relevant to travellers. We also drew on the UK guidelines for malaria prevention published by the Health Protection Agency6 and the malaria prevention guidelines published by the US, Canada, and the World Health Organization27 28 29 and Clinical Evidence.30
Additional educational resources
National Travel Health Network and Centre (www.nathnac.org)—General travel advice and detailed country recommendations and maps (for health professionals and travellers)
Fit For Travel (www.fitfortravel.scot.nhs.uk)—General guidance for travellers
Health Protection Agency’s malaria prevention guidelines (www.hpa.org.uk/infections/topics_az/malaria/guidelines.htm)—Highly detailed recommendations of all aspects of malaria prevention (for health professionals)
Centers for Disease Control and Prevention’s recommendations (www.cdc.gov/malaria/travel/index.htm)— General guidance (for health professionals and travellers)
World Health Organization: International Travel And Health (www.who.int/ith/en/index.html)—General guidance (for health professionals and travellers)
Questions for future research
How to engage those who are visiting friends and relatives
New agents for antimalarial prophylaxis
Role of standby treatment in areas of lower risk
Safety of antimalarials in pregnancy
Footnotes
Contributors: Both authors contributed to the conception and writing of this article. DGL is guarantor.
Competing interests: DGL has received educational support from GlaxoSmithKline to attend travel medicine meetings.
Provenance and peer review: Commissioned; externally peer reviewed.
References
Log in
Log in using your username and password
Log in through your institution
Subscribe from £173 *
Subscribe and get access to all BMJ articles, and much more.
* For online subscription
Access this article for 1 day for:
£38 / $45 / €42 (excludes VAT)
You can download a PDF version for your personal record.