Effects on birth weight and perinatal mortality of maternal dietary supplements in rural gambia: 5 year randomised controlled trial
BMJ 1997; 315 doi: https://doi.org/10.1136/bmj.315.7111.786 (Published 27 September 1997) Cite this as: BMJ 1997;315:786
- Sana M Ceesay, senior scientista,
- Andrew M Prentice (andrew.prentice{at}MRC-Dunn.cam.ac.uk), senior scientistb,
- Timothy J Cole, senior scientistb,
- Frances Foord, research midwifea,
- Elizabeth M E Poskitt, consultant paediatriciana,
- Lawrence T Weaver, consultant paediatricianb,
- Roger G Whitehead, directorb
- a MRC Dunn Nutrition Unit, Keneba, Gambia, West Africa
- b MRC Dunn Clinical Nutrition Centre, Cambridge CB2 2DH
- Correspondence to: Dr Prentice
- Accepted 21 May 1997
Abstract
Objective: To test the efficacy in terms of birth weight and infant survival of a diet supplement programme in pregnant African women through a primary healthcare system.
Design: 5 year controlled trial of all pregnant women in 28 villages randomised to daily supplementation with high energy groundnut biscuits (4.3MJ/day) for about 20 weeks before delivery (intervention) or after delivery (control).
Setting: Rural Gambia.
Subjects: Chronically undernourished women (twin bearers excluded), yielding 2047 singleton live births and 35 stillbirths.
Main outcome measures: Birth weight; prevalence of low birth weight (<2500 g); head circumference; birth length; gestational age; prevalence of stillbirths; neonatal and postneonatal mortality.
Results: Supplementation increased weight gain in pregnancy and significantly increased birth weight, particularly during the nutritionally debilitating hungry season (June to October). Weight gain increased by 201 g (P<0.001) in the hungry season, by 94 g (P<0.01) in the harvest season (November to May), and by 136 g (P<0.001) over the whole year. The odds ratio for low birthweight babies in supplemented women was 0.61 (95% confidence interval 0.47 to 0.79, P<0.001). Head circumference was significantly increased (P<0.01), but by only 3.1 mm. Birth length and duration of gestation were not affected. Supplementation significantly reduced perinatal mortality: the odds ratio was 0.47 (0.23 to 0.99, P<0.05) for stillbirths and 0.54 (0.35 to 0.85, P<0.01) for all deaths in first week of life. Mortality after 7 days was unaffected.
Conclusion: Prenatal dietary supplementation reduced retardation in intrauterine growth when effectively targeted at genuinely at-risk mothers. This was associated with a substantial reduction in the prevalence of stillbirths and in early neonatal mortality. The intervention can be successfully delivered through a primary healthcare system.
Key messages
In developing countries chronic maternal undernutrition is a prime contributor to the birth of over 25 million low birthweight babies annually and to high rates of neonatal mortality.
An absence of well designed field trials has created uncertainty about the potential efficacy of maternal feeding programmes
This large scale randomised controlled trial shows that dietary supplementation in pregnancy can be highly effective in reducing the proportion of low birthweight babies and perinatal mortality
Incorporating supplementary feeding into a rural primary healthcare system is feasible
Late pregnancy is the period most amenable to intervention
Introduction
Low birth weight is a major contributor to neonatal and postneonatal mortality. Twenty five million babies a year are born below 2500 g, the World Health Organisation's cut off point for low birth weight, and over 90% of these are born in developing countries where perinatal and infant mortality is already high.1
Considerable controversy still remains about whether dietary supplementation in pregnancy can increase birth weight. Some authors argue that the case at best is unproved.2 3 Kramer performed a meta-analysis that showed only modest increases in maternal weight gain and fetal growth.4 Others have shown that when data are disaggregated certain subgroups of women do benefit,5 6 7 8 9 10 though Kramer's meta-analysis failed to find evidence that undernourished women benefited more than those who were adequately nourished.4 Interpretation is often hampered by inadequate experimental design.2
We reported a highly significant beneficial effect of supplementation in a trial involving 379 rural Gambian women.6 11 This trial was criticised, and was not entered in Kramer's analysis because it used historical controls (a condition imposed by an ethics committee). Additionally, the supplement was complex and expensive, and its distribution and consumption were carried out under intensive experimental conditions.
In the present study we tested the efficacy of a cheaper dietary supplement provided under realistic field conditions through the primary healthcare system in the Gambia. We report results from a 5 year prospective randomised controlled trial in 28 rural villages, with birth weight and infant survival as the primary outcome measures.
Methods
Design
The study was conducted among rural, subsistence-farming communities in the West Kiang region (population about 12 000) of the Gambia. Detailed descriptions of nutritional conditions are available elsewhere.12 13 Briefly, a diet chronically marginal for many nutrients is exacerbated by a hungry (wet) season (June to October), when food stocks from the previous harvest are depleted. These food shortages are compounded by arduous farm work during the same season and result in rapid weight loss averaging 3–6 kg in adults each hungry season. These periods of negative energy balance are associated with a decrease in average birth weight and an increase in the proportion of low birthweight babies.6
At the beginning of 1989 all women of childbearing age (15 to 45 years) were recruited from 28 villages for baseline anthropometric and demographic measurements after a description of the study at village meetings. New immigrants and girls reaching menarche were added as the study progressed. The villages were randomised to intervention (supplement provided from around 20 weeks' gestation to term) or control (supplement provided for 20 weeks after delivery) using a stratified design according to village size. From July 1989 all eligible pregnant women were given a more detailed description of the study and invited to enrol; over 95% agreed and remained in the trial throughout. Most pregnancies were identified by 16–18 weeks by a mobile midwifery service and traditional village birth attendants, but the women were sometimes reluctant to admit pregnancy this early. Supplementation was therefore started as close as possible to 20 weeks' gestation as judged by clinical examination. The analysis presented here covers 2047 normal singleton live births (and 35 stillbirths used for mortality analysis only) from 1460 different women who delivered during October 1989 to October 1994. Initial calculations of sample size indicated that a 3 year trial would provide sufficient power for detecting the most limiting outcome variable (mortality), but lower than expected death rates forced a 2 year extension. The study and extension were approved by a joint ethics committee of the Medical Research Council and the Gambian government.
Health care
Women in both the control and the intervention villages received routine antenatal care (interview; abdominal palpation; blood pressure and haemoglobin and urine protein concentrations; treatment or referral as indicated) from midwives in a mobile clinic that visited each village twice monthly. All women received graded, combined iron and folate supplements according to their haemoglobin concentration. Tetanus toxoid was given to all women not previously protected, and during the hungry season all women received a weekly prophylactic dose of chloroquine.
Supplement
The supplement biscuits contained roasted groundnuts, rice flour, sugar, and groundnut oil, and they provided a maximum possible daily intake (two biscuits) of 4250 kJ energy, 22 g protein, 56 g fat, 47 mg calcium, and 1.8 mg iron. The local ingredients for the biscuits were prepared at a single centre by village women, and the biscuits were cooked using traditional clay ovens in two of the villages. Biscuits were then regularly distributed to the two birth attendants in each village, who issued them to participating women. Compliance was intensively encouraged and recorded by the birth attendants, in whose presence the biscuits had to be consumed.
Measurements
Maternal height (baseline), maternal weight (fortnightly), parity, birth weight, birth length, head circumference, and gestational age within 48 hours of delivery were assessed by eight fieldworkers. Birth weights were measured to the nearest 20 g with portable spring balances and tared sling (CMS Weighing Equipment, London), regularly checked with standard weights. Maternal weights were recorded to the nearest 200 g on spring scales (same supplier). Birth length was measured to the nearest 5 mm using neonatal length mats (TALC Teaching Aids, St Albans, England). Gestational age was assessed by the Parkin method (a simplified Dubowitz procedure), which scores four external characteristics: skin colour, skin texture, ear firmness, and breast development.14 The method has 95% confidence intervals of 15 days and is more appropriate for fieldworkers than the full Dubowitz score. Head circumference was measured to the nearest millimetre with graduated tapes (Henley Medical Supplies, Welwyn Garden City, England) at 48 hours after delivery. The fieldworkers were trained and cross compared in anthropometric techniques and Parkin scoring in the delivery wards of the Gambia's main hospital. The linearity of the curve and small error bars for birth weight by gestational age (see figure 1) lend confidence to the fieldworkers' ability to assess gestational age. Stillbirths were recorded by the birth attendants and cross checked by our fieldworkers and the mobile midwives. Infant deaths were recorded by a government-appointed village recorder and cross checked by fieldworkers when each infant became due for follow up anthropometry.
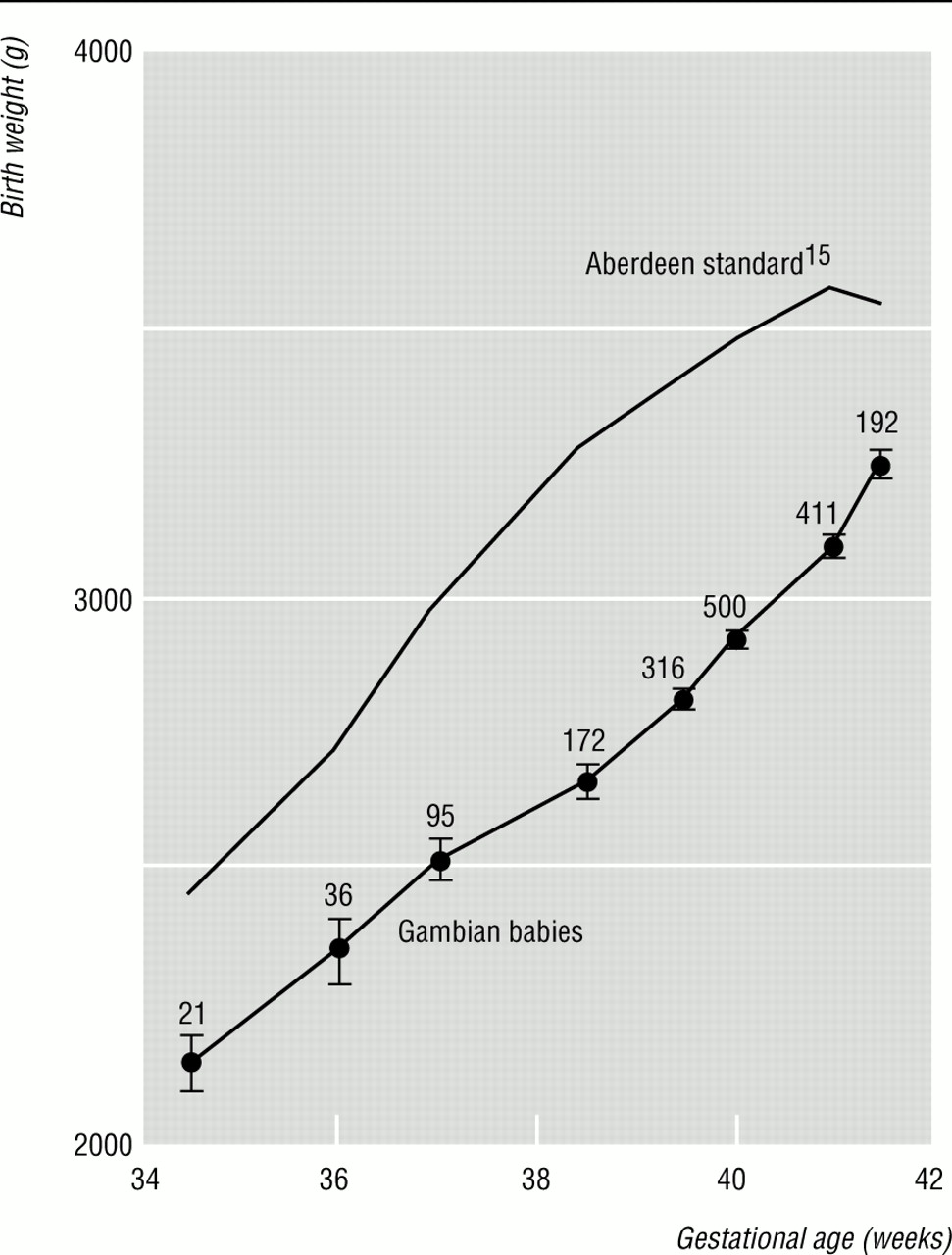
Comparison of intrauterine growth curves for Gambian and Scottish babies. Numbers of Gambian births are indicated
{kind=link}
Statistical analysis
Randomisation of the intervention by village required multilevel (or three stage random effects) modelling to estimate variances at the village, mother, and baby levels (Multi-Level Models Program, Institute of Education, University of London, 1995). The multilevel modelling used multiple regression, with separate error terms for village, mother, and baby levels. Supplement was entered either as a binary variable or as the number of days for which each mother received the supplement. Birth order was entered as a binary variable identifying primigravidity versus multigravidity (more predictive than birth order as a continuous variable). Maternal weight was entered as weight after delivery, and weight gain as the slope of each subject's individual regression line for all weights during pregnancy. Gestational age was entered as the raw Parkin score as this was more predictive than the derived weeks of gestation due to non-linearity of the Parkin conversion. In this analysis the hungry season was defined as June to October on the basis of environmental and nutritional events and because post hoc analysis indicated that this selection yielded the greatest discrimination between hungry and harvest season effects (harvest (dry) season is November to May). The characteristics for the control and intervention groups are summarised in table 1. There were no significant differences except for maternal weight and body mass index (weight (kg)/(height (m)2)), measured after delivery, which respectively were 1.2 kg and 0.6 greater in the intervention group as a result of supplementation (both P<0.001).
Characteristics of 1460 chronically undernourished rural Gambian women who delivered between October 1989 and October 1994 (2047 singleton livebirths and 35 stillbirths). Values are number (percentages) or means (SD)
Results
Normal influences on pregnancy in West Kiang
Table 2 shows that gestational age, maternal parity, sex of the baby, and season of the year all have highly significant effects on birth weight that can be adjusted for when analysing the effects of supplementation. The coefficients are similar to those that we reported previously for this community.6 Maternal postpartum weight (coefficient 9.4 g/kg, SE 1.2 g/kg, P<0.01) and weight gain in pregnancy (299 g/kg/month, SE 79 g/kg/month, P<0.001) also influenced birth weight but were not included in the analysis of intervention effects as this would falsely eliminate any beneficial effect of supplementation mediated through increased maternal weight gain.
Factors influencing birth weight in rural Gambia*
Figure 1 compares the intrauterine growth curves for West Kiang with the Aberdeen standards15, selected as representing births at sea level in a well nourished population. Both curves were generated cross sectionally by plotting weight at birth against gestational age. At 35 weeks' gestation the Gambian babies were about 250 g smaller than their well nourished counterparts. This difference increased to 600 g at term, with some indication of the gap narrowing post term. Adjustment for differences in maternal stature accounts for only 10% of this difference, leaving the rest unexplained and potentially related to undernutrition.
The usual seasonal variation in birth weight in rural Gambia is shown by the data for the control group in figure 2. Peak birth weights occurred at the end of the harvest season (April to May) and were about 250 g higher than in the trough during the hungry season. The coefficient for the hungry season effect in table 2 is appreciably smaller than the peak-to-trough difference because it compares the average values across the whole of the two seasons.

Seasonal pattern of mean birth weights in control and intervention villages
{kind=link}
Uptake of supplement
The mean number of days that women attended for supplement was 82 (SD 31) out of a possible total of about 135 as most women were recruited at 20–24 weeks' gestation. The birth attendants reported that most women ate their full allocation of biscuits when they attended.
Effects of supplementation
Birth outcome
Table 3 summarises the intervention effects after adjustment for sex, primiparity, and Parkin score. For the seasons combined, supplementation significantly increased birth weight (by 136 g, P<0.001) and head circumference (by 3.1 mm, P<0.01). Birth length was not affected. The effect of supplementation on birth weight was primarily achieved through a reduction in babies who were “small for their dates,” rather than a reduction in prematurity, as gestational age was not affected.
Multiple regression analysis of effect of supplementation on birth outcome after adjustments*
The effect on birth weight was greater in the hungry season (increase of 201 g v 94 g). The same was true for head circumference (3.9 mm v 2.5 mm) and for birth length (4.1 v decrease of 1 mm), although the length effects were non-significant. Figure 2 compares supplemented and control birth weights by calendar month. The biggest differences occurred in June, July, September, and October. The seasonal variation in birth weights was not totally eliminated by supplementation.
Because some Parkin scores were missing—for example, for babies born in hospital—and some parities were uncertain, the degrees of freedom for an unadjusted birthweight analysis increased from 1751 to 2047. With unadjusted analysis, birth weight increased by 213 g (P<0.001) in the hungry season, 68 g (P<0.01) in the harvest season, and 106 g (P<0.001) over the whole year. For other outcomes the significance levels for unadjusted data were also virtually identical; coefficients were very slightly lower.
The analysis was repeated, with days of supplementation in place of the binary intervention variable, to test whether heterogeneity in supplement uptake influenced outcome, This yielded similar t values to those listed in table 3, indicating that supplement uptake did not contribute additional predictive value. During the hungry season birth weight increased by 1.17 g/biscuit (SE 0.17 g)—an energy conversion ratio of 1 g/1.8MJ.
Distribution of birth weight and incidence of low birth weight
The cumulative distribution plots for supplemented and control birth weights were essentially parallel, indicating that the intervention shifted the whole distribution of birth weight towards heavier babies rather than having a selective effect on small babies.
Table 4 shows the numbers of low birthweight babies (<2500 g). Over the whole year supplementation reduced the prevalence from 176/1037 (17.0%) to 112/1010 (11.1%) (P<0.001, by the χ2 test). The effects during the hungry and harvest seasons were similar, although there were more low birthweight babies in the hungry season.
Numbers (percentage) of low birthweight babies (<2500 g) with odds ratios (95% confidence interval)
Effect of supplementation on perinatal and neonatal death rates
Discussion
This randomised controlled trial showed that the provision of a high energy, prenatal, dietary supplement significantly reduced retardation of intrauterine growth and perinatal mortality. The effects on birth weight were closely similar to those observed in our previous intensive trial in which a more complex and expensive supplement was provided under much more tightly controlled conditions.6 11 The current estimates of gains of 201 g, 94 g, and 136 g for hungry, harvest, and the whole year respectively, compared with 200 g, 13 g, and 116 g for the previous trial. Such similar results from trials using different designs (retrospective v contemporary controls), spanning 13 years of observation, and now covering 28 different villages, reinforces the credibility of the findings.
The ability of supplementation to reverse the retardation of fetal growth in the hungry season when provided for an average of only 82 days in the second half of pregnancy is consistent with findings from the Dutch “hunger winter” of 1944-5,16 and illustrates that fetal growth is most sensitive to nutritional deprivation in the last trimester of pregnancy. This is of considerable advantage in incorporating supplementation into a primary healthcare scheme as it does not seem necessary to intervene early in pregnancy, and women in late pregnancy form an easily identifiable subgroup.
Although there is considerable controversy about the likely efficacy of dietary supplementation,2 3 4 we have previously argued that positive effects are likely if supplements can be effectively targeted at women with a genuine need.6 7 Rural Gambian women represent one such group, especially during the hungry season. They have low weight gain in pregnancy (about 60% of the recommended optimum),6 they often lose body fat in pregnancy,17 they have a high ratio of fetal weight to total weight gain in pregnancy (>40% versus about 25% in well nourished women),18 and they exhibit profound energy-sparing metabolic adjustments in pregnancy.18 These adjustments seem to be invoked in an attempt to maintain positive energy balance in conditions of undernutrition, but they fail to protect fetal growth fully.
Supplementation was associated with a significant but small increase in head circumference. In both of our Gambian trials the effect of intervention was greatest in the hungry season and tended to restore birth weight to the level during the harvest season. The largest increase in head circumference (3 mm during the hungry season) translates to an increase of only 1 mm in diameter. This is unlikely to raise the prevalence of cephalopelvic disproportion, and the perinatal mortality data further dispel this concern.
On the basis of the shift in birthweight distribution in our previous trial and the known relations between birth weight and mortality5 19 we had estimated a 37% reduction in neonatal mortality (equivalent to an odds ratio of 0.60) but had inadequate sample power to test the prediction.6 The current trial yielded an odds ratio of 0.54 for total perinatal deaths. This included stillbirths, which were not incorporated into the earlier modelling. The benefit is greater than we had expected and would represent a major public health effect if replicated elsewhere. We know of no studies reporting significant beneficial effects of prenatal supplementation on the rate of stillbirths or subsequent mortality. Long term monitoring of growth and mortality in these cohorts is continuing. Extrapolation of the general principles of the theory on the “fetal origins of adult disease” 20 would suggest that supplementation may confer additional benefits to the future health of the babies. An analysis of 1077 deaths in this community has recently shown that being born in the hungry season predicts a major excess of premature adult mortality (P<0.0001), with infections and pregnancy related maternal deaths as the predominant causes.21
Conclusion
A simple dietary supplementation programme with minimal supervision through a primary healthcare system in rural villages can reduce the retardation of fetal growth when targeted at a population in whom there is real evidence of nutritional deprivation during pregnancy—for example, due to seasonal deprivation. These findings focus attention on late pregnancy as the period most amenable to interventions.
Acknowledgments
We thank Dr Mike Rowland for advice and help in the early phases of the trial; Dr Wally Gilks for performing the village randomisation; members of the West Kiang midwifery service; and the fieldworkers, village bakers, and traditional birth attendants for their invaluable work throughout the study.
Funding: Medical Research Council, Overseas Development Administration, and Nestlé Foundation.
Conflict of interest: None.