Long term results of growth hormone treatment in France in children of short stature: population, register based study
BMJ 1997; 315 doi: https://doi.org/10.1136/bmj.315.7110.708 (Published 20 September 1997) Cite this as: BMJ 1997;315:708
- Joёl Coste⇑, associate professor of biostatisticsa (coste{at}cochin.univ-paris5.fr),
- Muriel Letrait, statisticianb,
- Jean Claude Carel, research associatec,
- Jean Pierre Tresca, associate professor of biochemistryb,
- Pierre Chatelain, professor of paediatricsc,
- Pierre Rochiccioli, professor of paediatricsc,
- Jean Louis Chaussain, professor of paediatricsc,
- Jean Claude Job, emeritus professor of paediatricsc
- a Département de Biostatistique et d'Informatique Médicale (Faculté Cochin, Université Paris V), Achard 7, Hôpital Cochin, 27 rue du Faubourg Saint-Jacques, 75674 Paris Cedex 14, France
- b Institut de Recherche Thérapeutique, Hôpital Cochin, Paris
- c Association France Hypophyse, Paris
- Correspondence to: Dr Coste
- Accepted 28 May 1997
Abstract
Objectives: To describe the growth of children treated with growth hormone and to evaluate the prognostic factors for height at the end of treatment.
Design: Register based cohort study.
Setting: French national register of all children treated with growth hormone.
Subjects: 3233 short stature children (3165 of whom were deficient in growth hormone) who were treated with growth hormone (excluding children with Turner's syndrome) and whose treatment started between 1973 and 1989, last data being recorded in December 1993.
Main outcome measures: Annual changes in height, and height at the end of treatment.
Results: Mean height SD score at the end of treatment, after a mean of 4.3 years, was −2, corresponding to gain in mean height SD score of 1 and to a height SD score of 1.1 below target height. In all, 923 children prematurely stopped taking growth hormone treatment, mainly because of insufficient response (insufficient growth) or tiredness. Variables that predicted height at the end of treatment were age, target height, aetiology of short stature, use of puberty inhibitors, and type of growth hormone.
Conclusions: The outcome of children of short stature with growth hormone deficiency who were treated with growth hormone has been less favourable than initially assumed. Growth hormone treatment has not restored normal growth to these children. The highly demanding nature and high costs of this treatment require an optimised prescription, and this remains to be determined.
Key messages
Key messages
Few data are available on the long term results of growth hormone treatment in children of short stature
Population based registers are ideal to provide information about the true use of treatments, characteristics of treated subjects and outcome as they are not distorted by selection criteria as in clinical trials or sponsored phase IV studies
The analysis of the data from the French register up to 1993 leads to a less optimistic view of the efficacy of growth hormone treatment than that generally held
Growth hormone treatment did not restore the genetic growth potential and thus should not be considered as a replacement treatment
Introduction
Growth hormone has been used for more than 30 years to treat short stature due to growth hormone deficiency. Knowledge about the long term results of this treatment, however, is limited. Most studies report short term results, usually after one year, in treated children. Prolonged follow up is rare,1 2 3 4 5 6 7 8 and even fewer studies have investigated factors influencing outcome.9 10 11 12 13 All studies used small groups of patients followed in specialist clinics1 2 3 4 5 7 8 10 or selected cohorts of children in clinical trials.6 9 11 12 13 Because treatment with growth hormone is demanding for the children and expensive for the community, it would only be justified if the long term outcome was satisfactory. Population, register based studies are the best approach to assessing final outcome.
We report a cohort study of all children of short stature, mainly with growth hormone deficiency, whose growth hormone treatment started in France between 1973 and 1989. We describe the growth of all treated children and identify the demographic, aetiological, clinical, and treatment factors that had a prognostic value for height at the scheduled end of treatment.
Material and methods
Subjects
The prescription of growth hormone has been regulated in France since 1973 under the medical control of Association France Hypophyse (the organisation responsible for prescribing growth hormone in France). Human extracted growth hormone—and from 1986-7 onwards growth hormone produced by recombinant DNA technology—was used. All deliveries of growth hormone to hospitals' pharmacies were registered, and relevant data on treated children were recorded on standardised charts. All children who started treatment before 31 December 1989 were identified. Only patients with Turner's syndrome (n=88), whose outcome has been reported elsewhere,14 were excluded, giving a study group of 3233 children.
Data collected
At baseline (start of treatment) and follow up visits (every 3 months until the treatment ended) the following data were recorded by individual paediatricians and communicated to Association France Hypophyse: height, weight, chronological age, bone age,15 stage of puberty,16 17 dose, frequency of injection, type of growth hormone (human or recombinant), and associated treatments. Parents' height, aetiology of short stature, and the results of two stimulation tests were provided. Growth hormone assays were performed by individual centres.
Growth hormone deficiency was diagnosed on the basis of auxometric data and growth hormone stimulation tests and was coded according to a standardised classification. The decision to continue or end the treatment was revised annually by Association France Hypophyse. The criterion for ending treatment was a growth velocity <20 mm in the previous 6 months with a bone age >=13 years for girls and >=14.5 years for boys.
Data from follow up visits were available until 31 December 1993. At that date, 1700 children had met the criterion for treatment to be ended, 923 had stopped treatment before meeting the criterion, and 610 who had not yet met the criterion were continuing treatment.
Analysis of growth and statistical methods
Growth was analysed as proposed by Cole.18 Standard deviation (SD) scores of height and weight for age and sex were calculated by using standards from a cohort of French individuals who had reached adult height in the late 1970s.19 Target height SD score was calculated as the mean of parental SD scores, obtained from standards of their (approximate) generation.20 The formula proposed by Ranke21 was used to account for the correlation between the heights of the parents.
The difference between the baseline height SD score and the score at later time points was calculated for 1, 2, 3, and 4 years of growth hormone treatment and at the end of treatment. Mean heights at the end of treatment corresponded to bone age 15.3 years (male) and 13.8 years (female) and were above 97.3% (male) and 97.8% (female) of adult height.22
A model for predicting height at the end of treatment (final height) was constructed in several stages.18 Firstly, the model had to predict outcome from demographic and auxometric information about the child at baseline (chronological and bone ages, stage of puberty, weight SD score, and target height SD score). Secondly, information about aetiology of short stature (diagnosis, peak concentration of growth hormone during stimulation tests) and about growth hormone treatment (dose, frequency of injection, type of growth hormone) and associated treatments were added to significant predictors of the preceding stage. The final stage was to test interactions between the treatment variables (dose, frequency of injection, type of growth hormone) and between these variables and weight and time interval.18 To account for the effect of regression towards the mean,23 all models included height SD score at baseline, time interval between baseline and final measurements, and the interaction between these two variables.18 As the main outcome response—final height SD score—was approximately normally distributed, no transformation was needed. Two potential predictors (mean dose and maximum stimulated peak concentration of growth hormone) were log transformed to yield more closely normally distributed variables.
The children who were treated after puberty had started were analysed separately and divided according to sex (age at puberty differs for girls and boys). The computations were performed with the SAS statistical package.24
Results
Characteristics of subjects and treatments
Baseline characteristics and methods of growth hormone treatment for 3233 children in France whose treatment started between 1973 and 1989. Values are numbers of children unless stated otherwise
Evolution of outcomes
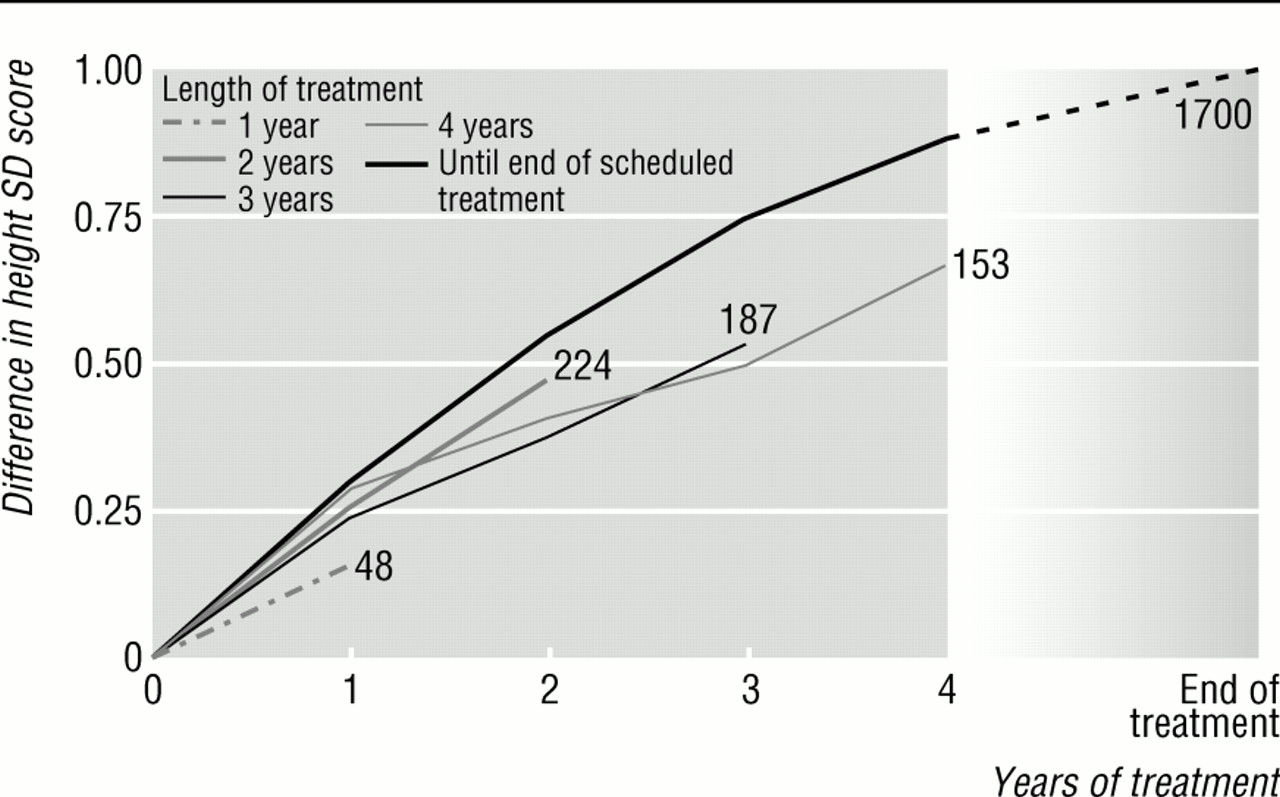
The mean annual change in height SD score was 0.3 during the first year of treatment, decreasing steadily thereafter (fig 1). Overall, the difference between the baseline height SD score and the final height score (after a mean of 4.3 years of treatment) was 1.0 (table 1). Thus the mean final height SD score was −2.0 (that is, 1.61 m for boys and 1.49 m for girls); the deficit in height SD score was −1.1 with respect to the genetic target.

Mean difference between height SD score at baseline and score at later time points, plotted against years of treatment for all children in study. Numbers refer to numbers of children in each category. Standard errors of mean SD scores are about 0.05
{kind=link}
Evolution of main outcome variables during follow up, according to pubertal state at baseline (start of treatment). Values are means (SD) unless stated otherwise
Altogether, 35% (923/2623) of children stopped receiving growth hormone treatment before the scheduled end of treatment (38% (668/1776) of children with idiopathic deficiency v 27% (215/784) of those with organic deficiency, P<0.0001; other baseline characteristics were similar for the continued or interrupted treatment groups (data not shown)). Interruption within the first 2 years of treatment was motivated by insufficient response (insufficient growth) in 98 children (fig 1) and by tiredness in 46.
Children whose treatment started after puberty responded less well to treatment from the first year of treatment onwards. In the pubertal group, the difference between the final height SD score and the baseline score was 0.8 for boys (treated for a mean of 2.8 years) and 0.5 for girls (2.7 years).
Prediction of final height
Model construction for final height SD score led to the three models shown in table 3. These models are similar and all include chronological age (with a second order polynomial decreasing effect) and target height. These two variables are the strongest predictors, which, together with effect variables in regression to the mean, explain 42% to 48% of outcome variance. Aetiology of short stature also had a predictive value for outcome. Craniospinal irradiation was always associated with a lower final height. Prepubertal children with idiopathic growth hormone deficiency responded less well to treatment than those with organic deficiency, whereas the opposite pattern was observed in pubertal children. Maximum stimulated peak concentration of growth hormone had an independent predictive value only in children treated before puberty. Variables in growth hormone treatment had much lower predictive value. Only type of growth hormone was related to the outcome: children who received human hormone had a mean height SD score 0.3 lower than children who received recombinant hormone; adjusting for mean dose of growth hormone and mean number of injections did not modify these associations. However, type of growth hormone explained only 1% of outcome variance. Puberty blockade was associated with a poorer outcome in children treated after puberty. The other study variables—namely, sex, weight SD score, pubertal stage, year that treatment started, mean dose of growth hormone, and mean number of injections—were not associated with outcome. Finally, we examined the correlation between the differences in height SD score at the start of treatment compared with the scores both after 1 year of treatment and at later time points: these correlations were low and inconsistent between groups.
Final prognostic models for final height SD score at the end of treatment, according to pubertal state at baseline (start of treatment)
Growth hormone deficiency v no deficiency
Sixty eight children of short stature but without growth hormone deficiency were treated on a compassionate basis. These children, mainly male (42) and prepubertal (56), had especially severe short stature (mean height SD score −3.4) and short parents (mean target height SD score −1.6). Annual height gains were low (fig 2), and 40 children stopped receiving treatment before the scheduled end of treatment. For those who were treated until the scheduled end, the final height SD score (mean duration of treatment 3.8 years) was −2.4. Analysis of the children with growth hormone deficiency provided results nearly identical to those obtained for the entire group (data not shown).
Mean difference between height SD score at baseline and score at later time points, plotted against years of treatment for short normal children. Numbers refer to numbers of children in each category. Standard errors of mean SD scores are about 0.10
{kind=link}
Discussion
Awareness of the value of population based registers to monitor efficacy and safety of treatments is improving.26 Registers can provide information about the true use of treatments, characteristics of treated people, and outcome. The information is not distorted by the restrictive selection criteria of clinical trials or sponsored phase IV studies.
The distribution of growth hormone in France was centrally controlled by a medical committee. Outcomes in this cohort were poorer than those previously reported.9 10 11 12 13 Despite years of a demanding treatment, treated children remained short—less than half had a final height SD score of above −2. The mean height gain after 1 year of treatment (SD score 0.3) was threefold to fivefold lower than gains reported by the Kabi international growth study11 12 and by Blethen et al.9 Similarly, the mean height gain by the end of treatment (SD score 1.0) was much lower that the nearly equivalent “final gain” reported by the Kabi international growth study (SD score 1.7 to 1.9, from 40 subjects13).
The large proportion of children (more than one third) whose treatment was prematurely stopped is another important finding. Clearly the treatment regimen is demanding, and children (or their doctors) may rapidly be discouraged, especially if the initial change in growth is not considered satisfactory. This observation strongly supports the need for analysing the results of growth hormone treatment according to the intention to treat principle.
Factors for predicting final height
This study identifies several factors that may be of predictive value for final height. In particular, chronological age, rather than bone age, is a strong predictor. The role of age, independent of treatment duration, was observed in both prepubertal and pubertal children. This relation possibly explains in part why the results were poorer for the children treated after the onset of puberty. This agrees with recent studies that identified age as the best prognostic feature.9 10 11 12 13 There are several possible explanations. Growth hormone deficiency causes a progressive and cumulative growth deficit, which is likely to be better compensated by early rather than late treatment.9 Also, as children age, growth is less directly influenced by growth hormone, and the influence of other factors such as sex steroids increases. Thirdly, children who are short at a given moment can be so because their growth velocity (known to vary substantially with time) had previously been low. The earlier this moment, the higher would be the expected subsequent growth velocity. This is consistent with a study by Greco et al, which reported that only one in three normal children of the 1958 birth cohort in Great Britain who were short at age 7 became a short adult.27
Target height was also highly predictive of final height. This result, also observed in most previously published studies,9 10 11 12 13 underlines the strong genetic influence on growth outcomes. This dependence should be carefully considered when interpreting outcomes in treated children who have a low target height—in particular, in those with idiopathic deficiency.9 12
Aetiology of short stature also predicted final height. As expected, craniospinal irradiation was associated with the worst outcome (as radiation has a large deleterious effect on vertebral growth). Results for other types of growth hormone deficiency were apparently conflicting. Outcome was better for prepubertal children with organic deficiency than with idiopathic deficiency. The opposite was found for patients treated after the onset of puberty. This again suggests that pubertal growth may be less influenced by growth hormone than by other factors—for example, sex steroids—so that compensation of growth hormone deficiency would be less effective than before puberty. Besides, the outcome for short children without deficiency was especially poor, a result which supports recent studies suggesting that growth hormone treatment has little value for such children.28
The only treatment variable that predicted height at the end of treatment was type of growth hormone (human or recombinant). Recombinant growth hormone was superior to the human type, a reassuring result as comparative trials, stopped because of Creutzfeldt-Jakob disease, were inconclusive. Unlike some short term studies,9 10 11 12 we did not find any relation between final height and mean (log) dose of growth hormone or frequency of injections. Puberty inhibitor was associated with poorer outcome in adolescent children, whereas most did not have precocious puberty. This fits with a recent report indicating that puberty blockade does not improve height gain in children with normal puberty.29 The independent predictive values of weight and maximum stimulated peak concentration of growth hormone remain unclear. We did not find consistent association between final height and these two variables, in agreement with some13 but not other studies.9 12
Despite the significant proportion of children who discontinued growth hormone treatment before the scheduled end of treatment, the evidence of a weak or no correlation between the difference in height SD score at the start of treatment compared with the scores both after 1 year of treatment and at later time points does not support the concept of responsiveness to growth hormone in growth hormone deficiency. This has implications for clinical practice: the final outcome cannot be predicted by the initial response.
Methodological considerations
Several methodological aspects of this study should be considered. Firstly, 65 % of treated children received only, or partly, human growth hormone. Thus the outcome described may be less favourable than the current outcome with generalised treatment with recombinant growth hormone. However, the scarcity of growth hormone treatment before 1987 is likely to have led to a better selection of short children being treated. Secondly, doses and injection frequencies of growth hormone were 30% to 50% lower than currently recommended in several countries. However, we did not find any relation between dose or frequency and height gain (perhaps partly because of the relatively narrow ranges of treatment methods). Thirdly, adult heights of treated children were not available, and a surrogate had to be used—height at the scheduled end of treatment, which corresponds at least to 97.3% (male) and 97.8% (female) of adult height in normal individuals.22 However, it seems unlikely that these children would gain much, in terms of the height SD score, after the discontinuation criteria had been met and treatment stopped. Fourthly, all data were obtained from routine examination in daily practice, and their reliability may therefore be questioned. In particular, the use of different growth hormone tests and assays may have resulted in substantial variability of reported peak concentrations of growth hormone and thus have limited the power to show a predictive value for this variable. Fifthly, analysis of data from observation cohorts such as ours should not be confused with data from controlled studies. Little information is available on the spontaneous adult height of the children with growth hormone deficiency, a highly heterogeneous group. However, a thorough analysis of our results allows the design of rational trials to reassess the clinical utility of growth hormone treatment in, for example, idiopathic forms of the deficiency. Finally, all analyses were adjusted on height at baseline and time between measurement to allow for regression to the mean.18 We also used height SD score rather than height itself since the standardised value eliminates the large dependency of height on age and sex.
Conclusion
This large, register based cohort study suggests that the outcome among children treated with growth hormone in the years 1973-93 was not as good as expected. Growth hormone treatment did not restore the genetic growth pattern and thus should not be considered as a replacement treatment, and even less as a “panacea” for children of short stature.30 Our findings, together with recent evidence on the limitations of growth hormone deficiency diagnostic tests,31 32 raise questions about indications for and methods of growth hormone treatment. Further research is needed to determine optimal use of these treatments. The large costs (Fr80 000; £10 000 a year in France for the cost of growth hormone alone) and highly demanding characteristics of growth hormone treatment require sensible prescription.
Acknowledgments
We thank the many paediatric endocrinologists who collected the clinical data and contributed to the validation of these; and to T J Cole for his comments on an earlier draft of this paper.
Funding: This study was supported by a grant from the French Ministry of Health (Direction Générale de la Santé).
Conflict of interest: None.